Article Text

Abstract
Objectives To study possible effects of aerosol exposure on lung function, fractional exhaled nitric oxide (FeNO) and inflammatory markers in blood from Norwegian cement production workers across one work shift (0 to 8 h) and again 32 h after the non-exposed baseline registration.
Methods 95 workers from two cement plants in Norway were included. Assessment of lung function included spirometry and gas diffusion pre- and post-shift (0 and 8 h). FeNO concentrations were measured and blood samples collected at 0, 8 and 32 h. Blood analysis included cell counts of leucocytes and mediators of inflammation.
Results The median respirable aerosol level was 0.3 mg/m3 (range 0.02–6.2 mg/m3). FEV1, FEF25–75% and DLCO decreased by 37 ml (p=0.04), 170 ml/s (p<0.001) and 0.17 mmol/min/kPa (p=0.02), respectively, across the shift. A 2 ppm reduction in FeNO between 0 and 32 h was detected (p=0.01). The number of leucocytes increased by 0.6×109 cells/l (p<0.001) across the shift, while fibrinogen levels increased by 0.02 g/l (p<0.001) from 0 to 32 h. TNF-α level increased and IL-10 decreased across the shift. Baseline levels of fibrinogen were associated with the highest level of respirable dust, and increased by 0.39 g/l (95% CI 0.06 to 0.72).
Conclusions We observed small cross-shift changes in lung function and inflammatory markers among cement production workers, indicating that inflammatory effects may occur at exposure levels well below 1 mg/m3. However, because the associations between these acute changes and personal exposure measurements were weak and as the long-term consequences are unknown, these findings should be tested in a follow-up study.
- Epidemiology
- immunology
- exposure assessment
- lung function
- inorganic dusts
This is an open-access article distributed under the terms of the Creative Commons Attribution Non-commercial License, which permits use, distribution, and reproduction in any medium, provided the original work is properly cited, the use is non commercial and is otherwise in compliance with the license. See: http://creativecommons.org/licenses/by-nc/2.0/ and http://creativecommons.org/licenses/by-nc/2.0/legalcode.
Statistics from Altmetric.com
What this paper adds
There are no former studies of gas diffusion capacity, fractional exhaled nitric oxide (FeNO) or inflammatory markers in blood among cement production workers.
We observed a cross-shift reduction in forced expiratory volume in 1 s (FEV1), forced mid-expiratory flow rate (FEF)25–75% and FeNO levels and an increase in white blood cells and fibrinogen levels, together with augmented TNF-α and decreased IL-10 concentrations in low level-exposed cement production workers.
Because the correlations with personal exposure measurements were weak and as the long-term consequences of these acute changes in lung function indices and inflammatory mediators are unknown, the hypothesis that low-level cement aerosol exposure causes airway disease should be tested in a follow-up study.
Introduction
The raw materials needed for the production of cement are mainly limestone and sources of silica, aluminium and iron. These are quarried, crushed and milled to a raw meal, which is heated in a kiln to approximately 1450°C to form clinker (cement base). The clinker is milled together with calcium sulphate and other additives to produce cement of different qualities.
A substantial number of cross-sectional studies have found associations between aerosol exposure and adverse respiratory health effects in cement production workers.1–7 However, other studies do not show such associations.8 9 Most studies have limitations because of their cross-sectional design, selection bias and sparse quantitative exposure data.
In addition to the cross-sectional studies, there are two cross-shift studies that show acute effects among cement production workers. Reductions in forced expiratory volume in 1 s (FEV1), FEV1/forced vital capacity (FVC) and forced mid-expiratory flow rate (FEF)25–75% across a shift were observed among Saudi Arabian workers10 and a cross-shift decrease in peak expiratory flow (PEF) was demonstrated in a Tanzanian study.11 Both studies were conducted in workers exposed to respirable aerosol levels of between 7 and 15 mg/m3, which are well above the present occupational exposure limit (OEL) of 5 mg/m3 in most European countries. Hence, they do not provide information about health effects at lower levels of exposure.
Few studies have attempted to elucidate the underlying physiological mechanisms involved in cement-induced respiratory effects. Irritation of mucus membranes because of the alkaline properties of cement dust (wet cement has a pH of about 12) and the possibility that other content particles (quartz, chromium) cause inflammation have been suggested. In a recent experimental study, cement dust was found to activate macrophage tumour necrosis factor (TNF)-α production in rat alveolar macrophages.12 We have previously observed an increase in the proportion of neutrophils and levels of interleukin (IL)-1β in induced sputum samples from cement production workers.13 However, information on the effects of assessed exposure on gas diffusion capacity (DLCO), fractional exhaled nitric oxide (FeNO) or inflammatory markers in blood is lacking.
To study further the acute effects associated with cement dust exposure, we aimed to investigate possible cross-shift changes in lung function variables, FeNO and inflammatory markers in peripheral blood. Personal aerosol levels were obtained in order to analyse associations between exposure and effect.
Materials and methods
Design
Workers from two cement production plants in Norway were examined before and after a shift of exposed work during the winters of 2008 and 2009. At baseline, each worker was required to have been off work for at least 2 days. The workers were exposed to cement production dust between 0 and 8 h, and again between 24 and 32 h. The participants underwent spirometry, gas diffusion assessment, FeNO measurement and blood sampling at baseline (0 h) and after a work shift (8 h). In addition, a third examination was performed consisting of FeNO measurements and blood sampling 32 h after baseline in order to study possible delayed effects. Only non-smokers (defined as never-smokers or ex-smokers who had stopped smoking at least 1 year before the examination) underwent FeNO sampling.
After completion of the health examinations at baseline, each worker was given a back-pack containing equipment for personal exposure measurements. The sampling cassettes collected respirable, thoracic and inhalable aerosol fractions and were mounted on shoulder straps as close to the mouth as possible. To minimise bias caused by their position, samplers were carried in front of either the right or the left shoulder in a random pattern. At the end of the shift, the equipment was removed and a questionnaire on work tasks performed was completed before the workers underwent the second health examination. In this study, it was not feasible to collect aerosol measurements on the second day (between 24 and 32 h).
Subjects
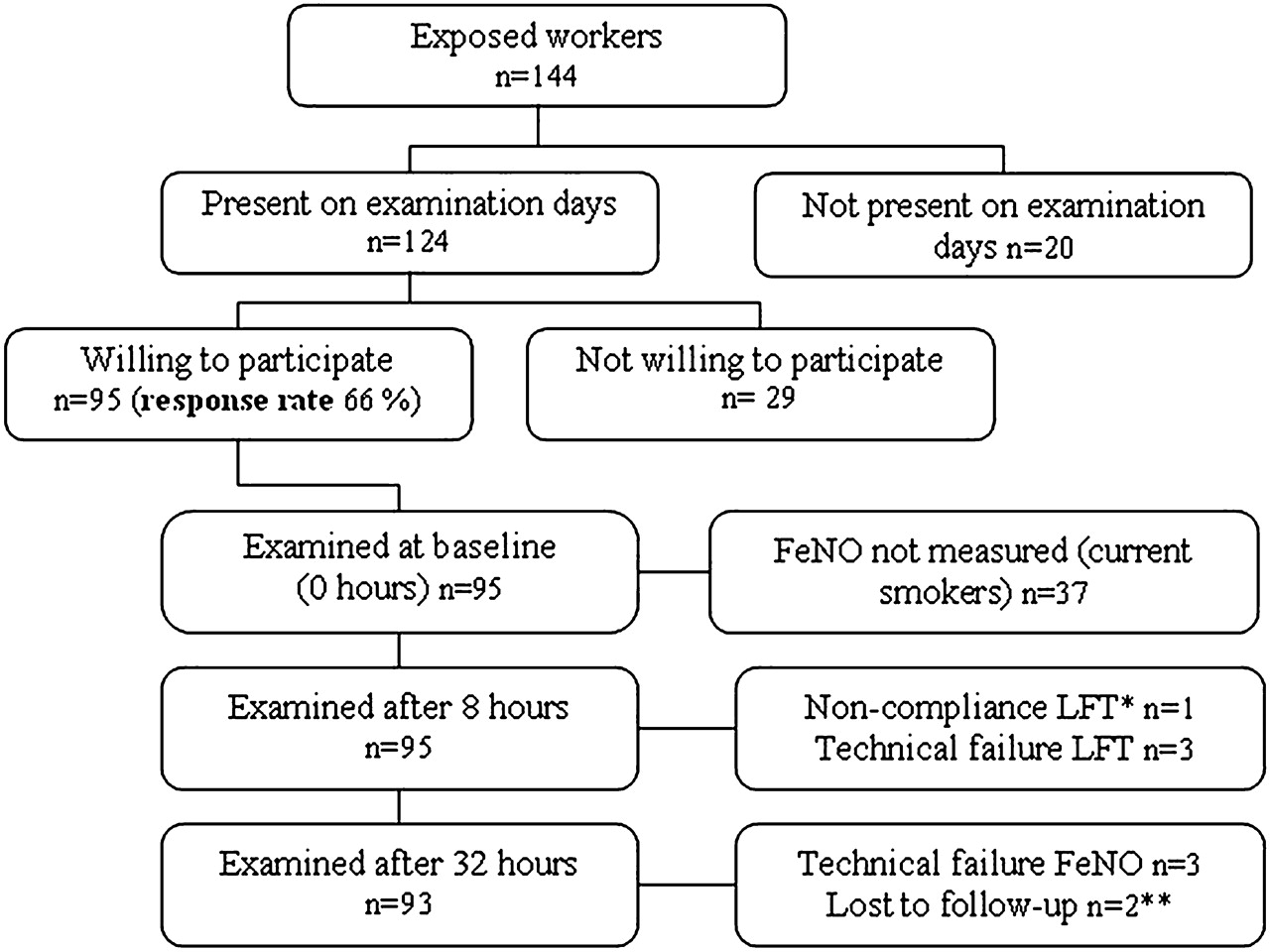
Exposed workers from the production and maintenance departments were identified from the company's register and invited to participate in the study. The eligible workers comprising of 144 subjects (5% females) were offered appointments for health examinations and exposure measurements. Of the 124 workers present on examination days, 95 (7% females) were willing to participate and were included in the study. The participation rate was 66%. A flowchart showing the inclusion and exclusion of workers is presented in figure 1 and the population characteristics are given in table 1.

{kind=link}
Flowchart for the inclusion and exclusion of cement production workers. *Lung function testing. **Workers who did not wish to participate 32 h after baseline.
Population characteristics given as mean (SD), duration of exposure and smoking status of cement production workers
The eligible workers received verbal and written information and informed consent was obtained from all participating subjects.
All included workers completed the investigation at baseline and at 8 h, but two workers did not attend for the third investigation (32 h). Spirometry was performed for all workers, but because of technical problems, the spirometry or gas diffusion tests could not be performed for three of the workers at 8 h. One worker did not meet the American Thoracic Society/European Respiratory Society (ATS/ERS) criteria for spirometry or gas diffusion14 15 and was excluded from the cross-shift analysis of lung function tests. Blood samples were not obtained on every occasion from eight subjects and for one subject we did not obtain any blood sample. The workers were asked: ‘Was your allergy confirmed by a physician?’ and ‘Was your asthma confirmed by a physician?’ If the answer was positive to either of these questions, they were defined as having doctor-diagnosed allergy or asthma.
Of the workers who did not want to participate in the study, two subjects had a known diagnosis of chronic obstructive pulmonary disease (COPD) and one of asthma. In the same group, eight workers had administrative jobs and were expected to have very low exposure or not to be exposed at all. Fourteen of the non-participants were non-smokers and 12 were smokers at the time of the measurements. We had no information on the smoking habits of three non-participating workers, but the smokers tended to be more heavily exposed to tobacco smoke than those included in the study.
Exposure assessment
The production of cement generates aerosols by mechanical and condensation processes and particle size ranges from ultra fine to above the inhalable. The workers in both departments reported day-to-day variation in work tasks and perceived exposure and that the use of respiratory equipment varied between individuals and tasks. Hence, the use of respirators was registered in order to allow comparison of outcomes between those who used a respirator and those who did not. The workers had access to Airstream-, P2- and P3-respirators, but we did not have information on which of these respirators the workers selected during this particular shift. The workers used respirators made by different manufacturers. The exposure measurements were performed outside the respirators.
The inhalable aerosol fraction that contains particles that enter the nose and mouth (<100 μm aerodynamic diameter, dae) was collected with the IOM inhalable dust sampler (SCK, Blandford Forum, Dorset, UK) equipped with a 25 mm cellulose-ester membrane filter with pore size 5 μm (SMWP02500; Millipore, Billerica, Massachusetts, USA) at a flow rate of 2.0 l/min. The thoracic fraction contains particles that pass the larynx (50% cut-off at dae=10 μm) and was collected with the BGI GK 2.69 respirable/thoracic sampler (BGI, Waltham, Massachusetts, USA) with 37 mm polyvinyl chloride filters with pore size 5 μm (Millipore, SKC and Pall, Port Washington, New York, USA) at a flow rate of 1.6 l/min.
The respirable fraction (50% cut-off at dae=4 μm) that enters the alveoli16 was collected by the respirable cyclone (Cassella, Amherst, New Hampshire, USA) with 37 mm polyvinyl chloride filters with pore size 5 μm at a flow rate of 2.2 l/min.
Lung function tests
Lung function tests were performed in accordance with ATS/ERS guidelines14 15 using the Jaeger Master Screen PFT (Erich Jaeger, Würzburg, Germany). The same investigator (AKMF) performed all lung function measurements. The workers were given standard instructions on the forced maximal expiratory manoeuvres and the transfer factor for the carbon monoxide (DLCO) test, with demonstration of the procedures. The tests were performed with the subject seated and breathing through the mouthpiece with a nose clip. The spirometer was calibrated with a 3 l syringe and test gas calibrations were performed using the instrument's automatic calibration programme. Both calibrations were performed daily. The best result, according to ATS/ERS criteria, of at least three manoeuvres of flow-volume measurements was used in the analysis. FVC, FEV1, FEF25–75% and forced expiratory flow rates at 25%, 50% and 75% of FVC expired (FEF25%, FEF50%, FEF75%) and PEF were measured.
Two measurements of DLCO were taken on each occasion and the average of the two results was used in the analysis. Effective alveolar volume was measured simultaneously by helium dilution and the gas transfer per unit effective alveolar volume (KCO) was calculated. The lung function measurements were performed before and after the work shift. Age, height, smoking habits and weight were registered. Lung function testing was performed subsequent to the exposure assessments, blood sampling and FeNO measurements to allow adjustment to indoor temperatures.
Fractional exhaled nitric oxide
FeNO in exhaled air was measured according to the ATS/ERS criteria17 using the NIOX MINO (Aerocrine, Solna, Sweden). This device provides FeNO measurements at 50 ml/s exhalation flow rate, expressed in parts per billion (ppb) using an electrochemical sensor. The accuracy range of the NIOX MINO device is ±3 ppb for measured values <30 ppb and 10% of the measured value for values >30 ppb, expressed as the standard deviation of 10 consecutive measurements. The measurements were performed before and after the work shift and again 32 h after baseline. Subjects were advised not to consume food or beverages 1 h before the measurements. Only non-smokers were selected for FeNO testing and the measurements were performed before the lung function measurements.
Assessment of blood parameters
Blood samples were collected at 0, 8 and 32 h in vacuum tubes containing citrate or EDTA as anticoagulant or containing no additives (serum). The citrate and serum tubes were centrifuged at 1400×g for 10 min. Plasma or serum was then aspirated and aliquoted into 1.5 ml Eppendorf polypropylene cryotubes within 1 h. The plasma and serum tubes were stored at −80°C until analysed. Leucocytes were analysed in EDTA blood samples within 48 h (in accordance with the instructions of the laboratory) using the Sysmex haematology system (Sysmex Europe, Hamburg, Germany) at the Oslo University Hospital, Ullevål, Oslo, Norway. The time period between the collection of blood samples and analysis at the laboratory was approximately the same for the two plants as transportation times were similar.
Quantitation of human serum C reactive protein (hsCRP) was performed using a high sensitive (hs) immunoturbidimetric assay on an Hitachi 917 Automatic Analyzer (Roche Diagnostics, Mannheim, Germany). The inter-assay variation (coefficient of variation, CV) was 5%. The fibrinogen concentration in citrate plasma samples was analysed using a clotting test on the STA-R Evolution (Diagnostica Stago, Asnières-sur-Seine, France). The inter-assay variation (CV) was 4%. D-dimer citrate plasma samples were analysed using an immunoturbidimetric method on the STA-R Evolution. The inter-assay variation (CV) was 3%.
The serum samples were analysed for cytokines using a microsphere-based multiplexing bioassay system with Xmap technology (Luminex, Austin, Texas, USA). TNF-α, IL-1β, IL-6, IL-8 and IL-10 were analysed using the Bio-Plex Human Group 1 assay 6-plex (Bio-Rad, Hercules, California, USA). Analysis was performed according to the instructions of the manufacturer. The inter-assay variations (CV %) were calculated from supernatant aliquots (n=8) of LPS exposed human monocytes, stored at −80°C: TNF-α 12%, IL-1β 8%, IL-6 12%, IL-8 16% and IL-10 15%. The detection limits were set as the lowest standard in each assay: TNF-α 0.16 pg/ml, IL-1β 0.06 pg/ml, IL-6 0.18 pg/ml, IL-8 0.04 pg/ml and IL-10 0.16 pg/ml.
Statistical methods
The Student paired t test was used to compare normally distributed continuous outcomes (the cross-shift changes in lung function indices). The Wilcoxon signed-rank test was used to compare the FeNO and inflammatory markers cross-shift. The Spearman rank test was used for correlations.
Independent variables considered to be biological important cofactors were included in the linear regression models. In addition, we included job task and location (plant 1 and 2) based on assumptions of differences in exposure levels. The cross-shift difference and the pre-shift level (8 h) of the health outcomes were analysed as dependent variables. Sex, age, height, body mass index, location (plant 1 or 2), report of doctor-diagnosed asthma, upper respiratory infection during the preceding 3 weeks, work tasks, life dose of tobacco (in kg), as well as the tertiles of the exposure levels (low, medium and high level as dummy variables compared to the lowest level) were included as independent variables for the lung function analysis. For the inflammatory markers, the above-mentioned independent variables, except for height and report of doctor-diagnosed asthma, were used in the regression model. Skewed variables were log-transformed in order to obtain acceptable linear regression models.
The study was designed with a power of 80% to detect a true difference of 1.5% between FEV1/FVC measured at two time points and a change in cytokine levels of 0.8 ng/l at a 5% significance level. At least 90 subjects were needed. Statistical analysis was performed using SPSS v 15.0 (SPSS).
Results
Exposure
Production workers performed inspection rounds throughout the plant, participated in solving problems which occurred during production (such as cleaning dust spills, carrying out minor mechanical work and opening up clogged production equipment) and also performed tasks in the control room. The maintenance workers maintained production equipment throughout the plant and inside their workshops. Respirable, thoracic and inhalable aerosol fraction measurements from the two cement producing plants are presented in table 2.
Exposure measurements by job category, and the values for workers using respirators compared to those without respirators
Six inhalable, four thoracic and eight respirable samplers did not obtain valid aerosol measurements; the most important reason was pump failure. The missing values were substituted with values predicted by linear regression models of the three aerosol fractions using the others as independent variables. The regression equation for the thoracic fraction was: log(thoracic value)=0.291+1.01 log(respirable value)−0.12(factor for plant 1). For the inhalable fraction: log(inhalable value)=0.82+0.96 log(thoracic value) and for the respirable fraction: log(respirable value)=−0.32+0.79 log(thoracic value). The variance explained by the regression models was 77–83%. The aerosol weight of samples was corrected with field blanks that had been weighed on the same day. When the weight was below the detection limit, the actual observed weight was used in the data analysis, and values of 0 or less were replaced by the lowest observed positive value within the job group divided by 2. Two of the samples were below the results of the field blanks.
The thoracic aerosol fraction was significantly higher in plant 2 than in plant 1, whereas there was no difference in the inhalable or respiratory fractions. In plant 1, 54% of the workers had been using respirators, while 23% had done so in plant 2. Of the 34 workers reporting use of respirators, 13 reported occasional use, 12 reported use most of the time and 9 reported use all the time. The aerosol concentrations were higher for those using respirators (table 2). The median respirable aerosol as a fraction of the inhalable aerosol was 10% and 8%, respectively, for plants 1 and 2. The thoracic aerosol as a fraction of the inhalable aerosol was 15% for plant 1 and 18% for plant 2.
Health effects
Lung function
We detected a decrease of 37 ml (p=0.04) and 170 ml/s (p<0.001), respectively, in FEV1 and FEF25–75% during the shift. There was a decrease in the gas diffusion capacity of 0.17 mmol/min/kPa (p=0.02) across the shift. Selected lung function and gas diffusion indices are presented in table 3.
Selected lung function variables pre- and post-shift (0 and 8 h) in cement production workers, in non-smoking workers and in those without doctor-diagnosed asthma or allergy
No associations between the changes in lung function variables and exposure were observed. This was the case for the whole group of workers and also when those who did not use respiratory protection were analysed separately.
FeNO and blood parameters
There was a decrease of 2 ppm (p=0.008) in FeNO between baseline values and those at 32 h after baseline. Furthermore, a significant cross-shift increase in white blood cells of 0.6×109 cells/l (p<0.001) was detected, while fibrinogen levels increased by 0.02 g/l (p<0.001) from baseline to 32 h. The TNF-α level increased, whereas IL-10 decreased across the shift. Thereafter, there was a decrease in all inflammatory markers except IL-10. The levels of inflammatory markers and FeNO at 0, 8 and 32 h are shown in table 4.
Blood parameters and FeNO levels pre-and post-shift (0 and 8 h) and at 32 h
The pattern of changes in inflammatory markers remained unchanged when those without doctor-diagnosed allergy or asthma were analysed separately. This was also the case for non-smokers.
There was a positive correlation between the differences (0 to 32 h) in fibrinogen and hsCRP (r=0.48; p<0.001). In a multiple linear regression model, the 0 h level of fibrinogen was associated with the highest respirable aerosol level (>0.4 mg/m3), and increased by 0.39 g/l (95% CI 0.06 to 0.72). There were no associations between the cross-shift changes of the inflammatory markers and the exposure variables for either the whole group of workers or when stratified for the variable regarding use of respiratory protection.
Discussion
We observed a cross-shift reduction in FEV1, FEF25–75%, DLCO and FeNO levels, and an increase in white blood cells and fibrinogen levels, together with elevated TNF-α levels and decreased IL-10 in low level-exposed cement production workers. No positive correlations between the cross-shift changes in lung function, FeNO or inflammatory markers and the measurements of personal exposure levels were detected.
Our finding of a cross-shift decrease in lung function indices agrees with the results of two earlier cross-shift studies among cement production workers exposed to higher levels of dust, which showed a reduction in FEV1, FEV1/FVC, FEF25–75% and/or PEF.10 11 Cross-shift studies are of particular interest because in occupationally exposed groups, a longitudinal decrease in lung function seems to be associated with a cross-shift reduction in these values.18 19 We did not detect an association between the changes in spirometric indices and individual exposures measured in this study. Nevertheless, because diurnal variation in spirometry in healthy, non-exposed subjects is shown to cause an increase during the first 6–8 h of time awake,20 the observed reduction in spirometric indices could possibly be associated with job tasks, peak exposure or other unknown conditions not measured in our study.
A cross-shift reduction in the gas diffusion capacity (assessed as DLCO and KCO) was observed. There are no prior studies on gas diffusion capacity among workers in this industry, but reduced gas diffusion capacity has been shown in other industries with dusty environments.21 A possible mechanism of a decrease in DLCO could be that a fraction of the aerosol small enough to reach the alveoli interacts with the alveolocapillary function and thereby reduces gas diffusion capacity. Another possibility is that exposures other than cement production dust, such as inhalation of carbon monoxide from vehicles or machines, could blockade the haemoglobin molecules and thereby lower the gas diffusion capacity. However, this will remain speculation until other studies on gas diffusion capacity have been reported among these workers.
The changes in lung function were not accompanied by cross-shift changes in FeNO levels, but a small significant decrease was observed when baseline values were compared with those measured at 32 h. Reduced FeNO levels are observed in smokers.22 23 Our finding could possibly indicate a similar response, but because the observed changes are minor and because we did not have measurements at 24 h, this finding needs to be confirmed by others.
There was an increase in the number of leucocytes across the shift. In light of this observation, it might be that cement dust causes an increase in neutrophil activity. This would be in agreement with our previous findings of an increased proportion of neutrophils and levels of IL-1β in induced sputum from these workers.13
It has been shown that inhalation of very fine dust from air pollution and from occupational exposures can induce the release of mediators that may influence blood coagulation.24–28 Thus, the observed increase in fibrinogen and hsCRP levels at 32 h accompanied by a positive correlation between the differences in fibrinogen and hsCRP could indicate an effect on blood coagulation among the workers. This finding could be induced by workplace exposure or perhaps more likely is a result of diurnal variation. Still, fibrinogen levels show low biological variability and the highest values in healthy, non-exposed subjects are recorded in the late morning.29 However, there was no change in the level of D-dimer and the observed difference in fibrinogen is small. Hence, the observed increase in fibrinogen levels should be interpreted with caution.
We observed an increase in TNF-α and a decrease in IL-10 across the shift. The diurnal rhythmicity of the pro-inflammatory cytokine TNF-α shows production peaks in the early morning with a subsequent fall during the day,30 whereas the anti-inflammatory cytokine IL-10 peaks during daytime.31 It is not clear if our finding of an inverse pattern represents an inflammatory response or if it is only a marker of exposure. The finding agrees with results from studies of cytokine levels in bronchial epithelial cells after exposure to cigarette smoke.32 33 However, the changes are small and because no associations with exposure were detected, it remains unclear if this finding represents a true response.
Our data show that levels of the pro-inflammatory cytokines IL-1β, IL-6 and IL-8 decreased during the observation period. These findings, together with the FeNO results, are probably indicative of no or low inflammatory activity. A decrease in cytokine levels could also possibly occur if the workers had higher levels of physical activity during the work shift than during the preceding period of rest, as shown in studies of healthy, non-exposed subjects.34 35 However, it is noted that the analysis of FeNO and inflammatory markers in our study is based on the examination of effects at three different time points only and it seems possible that other or additional time points (eg, 4 h and 24 h) could have revealed other patterns of response and made interpretation of these findings easier.
The changes in lung function indices and inflammatory markers across the shift were similar in those without doctor-diagnosed allergy or asthma as compared to the whole group of workers. In non-smokers the changes in spirometric indices were slightly stronger than in the whole group and the changes in inflammatory markers were similar. These findings indicate that the observed effects probably cannot be explained by allergy or smoking alone. However, a decrease in the DLCO level of 0.60 (95% CI 0.29 to 0.91) mmol/min/kPa among those with allergy or asthma was demonstrated, while there was no change among those without these conditions. This could possibly indicate that the changes in gas diffusion could be influenced by subjects with hyper-responsive airways.
The personal sampling of aerosol concentration allows correlation and linear regression analyses with exposure as a continuous variable. Surprisingly, no correlations were observed between exposure and cross-shift changes in the outcome variables. This was also the case when those using respirators and those not were analysed separately. The respirable aerosol level among the exposed workers in this study was well below the Norwegian OEL (respirable aerosol, 5 mg/m3), as was the thoracic fraction. In addition, the exposure measurements showed that the particle size of the aerosols in the measured periods for both plants was mostly inhalable and therefore will deposit in the upper respiratory system. Thus, other descriptors of exposure such as the chemical composition of the aerosol at different locations of the plant and peak exposures could be of importance and should be considered for inclusion in further studies. Furthermore, regression analysis showed that in the workers with the highest levels of exposure, the pre-shift level of fibrinogen was associated with exposure, indicating that previous exposure could also be of importance.
It is possible that individuals susceptible to adverse effects from cement aerosols had left the cement industry, leaving only robust subjects in the workforce to be included in the study. If this were the case, we would have underestimated the inflammatory effects of exposure. However, because workers are used as their own controls in this study, selection bias is probably less important.36 To reduce bias related to the collection of data, all lung function tests were performed by one researcher. Standard instructions were followed for spirometry, lung diffusion and FeNO and the blood samples were analysed by individuals blinded to exposure information.
Confounders that may not be controlled adequately or adjusted for in the analysis could include unknown respiratory irritants outside the workplace, especially in the period before the first health measurements were performed. It is also possible that a greater cross-shift change in lung function, FeNO, or in levels of inflammatory markers would have occurred if the period of non-exposure before baseline had been extended.
We observed a higher prevalence of smokers among the non-participants than among the included subjects. This is not considered to be a limitation of the study because it is likely that existing tobacco smoke-related inflammatory effects among these workers would have made detection of effects from the cement production aerosol difficult, resulting in an underestimation rather than in an overestimation of effects.
It is not clear whether the cross-shift changes in lung function indices and inflammatory markers as observed in this study represent an early stage of inflammation leading to respiratory disease or whether they represent an appropriate immune response without clinical consequences. However, until follow-up studies are completed and interpreted in relation to these questions, we recommend a reduction in exposure for workers with the highest exposure levels and that spirometric surveillance is carried out at regular intervals.
In conclusion, we observed small but significant cross-shift reductions in FEV1, FEF25–75%, DLCO and FeNO levels corresponding with increased numbers of leucocytes, elevated levels of fibrinogen and TNF-α and decreased levels of IL-10 in low level-exposed cement production workers. Because the correlations with exposure were weak and while the long-term consequences of these acute changes in lung function indices and inflammatory mediators are unknown, the hypothesis that low-grade cement aerosol exposure causes airway disease should be tested in a follow-up study.
Acknowledgments
We are grateful to the participants from the Norcem AS cement plants in Brevik and Kjøpsvik, Norway. We thank Harald Evenseth for help with the collection of exposure data.
References
Footnotes
Funding This study was supported by grants from the South-Eastern Norway Regional Health Authority and The European Cement Association (Cembureau).
Competing interests None.
Ethics approval This study was conducted with the approval of The National Committee for Medical and Health Research Ethics.
Provenance and peer review Not commissioned; externally peer reviewed.