Article Text

Abstract
Objectives: To investigate the effectiveness of a counselling and education programme on work ability and work disability pension for employees in the construction industry.
Methods: Employees with a high disability risk of 38% or more in the following four years were included. Employees in the intervention group were either selected by an occupational physician or enrolled themselves. They received an assessment and individual programme focused on optimising work functioning, while the control group received care-as-usual. Data on work ability measured with the Work Ability Index (WAI) and work disability pensions were collected at baseline during a periodic occupational health examination and at 9, 18 and 26 months after the start of the intervention using a questionnaire.
Results: Most employees in both the intervention (n = 83) and control group (n = 209) were carpenters (43% and 37%) and bricklayers (7% and 15%). In the intervention group, 42% successfully completed the programme. Work ability in the intervention group was lower at baseline but showed an increase over time while work ability of the control group remained the same. The work ability in the intervention group improved slightly more (p = 0.09). No statistically significant differences in percentages of employees receiving a disability pension between the intervention and control group were found at 9 or 18 months and no differences in the age-adjusted percentages of employees receiving a disability pension were found between the groups at any measurement.
Conclusions: The programme was slightly effective in improving the work ability but not in reducing work disability pensions. A more comprehensive multidisciplinary intervention programme might be necessary.
Statistics from Altmetric.com
Workers in the construction industry are often exposed to hazardous working conditions, including the manual handling of loads, and exposure to vibration, noise, dust and chemicals.1 2 Adverse mental work conditions such as working under time pressure, employment without security or having boring work are also prevalent.3 It is, therefore, well recognised that construction workers are at a greater risk of developing health disorders and associated disabilities than workers in other industries and the general population.1 4 5 Several studies in Europe and the USA found that construction employees had a higher prevalence of musculoskeletal disorders, nervous complaints, allergies, lung diseases and hearing deficiencies.3 5–7 Moreover, accidents and falls are very common in the construction industry8 9 and they can result in serious injuries.
Among construction workers these health problems caused by the sustained heavy physical and/or mental working load, in addition to frequent accidents and injuries, are likely to reduce their work capacities and may lead to temporary absence from work and ultimately to permanent disability. A number of studies in European countries have shown a high incidence of permanent work incapacity among construction workers,4 10 mainly from musculoskeletal and cardiovascular diseases.1 4
It is important to prevent work disability pension because of the human and societal costs. Prevention of early retirement as a result of disability will become even more important, because the number of construction workers at risk for early retirement on health grounds is likely to rise in the near future as a result of the ageing population and work force.3 At the same time, recent changes in the social legislation in Europe3 11 12 and the recognition of disability pensioning as a social problem1 12 may imply that workers need to retire later than they have done in recent years.
In order to support workers at risk for a work-related disability in their efforts to remain in paid employment, early intervention programmes are needed that increase the work ability of workers whose capabilities at work no longer match the physical or mental requirements of their jobs. However, few such early intervention programmes for workers in the construction industry or elsewhere exist.13 14 It has been hypothesised that active management and coaching of the individual employee with difficulties prolonging his or her working life could prevent the construction worker at risk from early retirement by improving his work ability.15 16 Therefore, an intervention programme adopted on the individual capacities and focused on optimising work functioning was created for the construction industry. It was based on individual counselling, education and coaching in the workplace and/or support.
The aim of this study was to evaluate whether this occupational health intervention programme for construction workers at risk could (1) increase work ability and (2) reduce work disability pensions.
SUBJECTS AND METHODS
Subjects
All subjects were Dutch workers employed in the construction industry. Inclusion criteria for the intervention group were builders aged 18–64 years and working for a company in the province of North Holland, while the control group consisted of builders aged 40–64 years working for a company elsewhere in the Netherlands.
Design
This study consisted of a prospective intervention study with a longitudinal follow-up. The project included two steps: (1) the selection of workers at risk; and (2) the provision of a counselling and education programme.
The selection of workers at risk was based on a previously developed decision model for the identification of workers at risk for work disability in the forthcoming four years.17 For the intervention group, occupational physicians were asked to select workers at risk and refer these workers to the training programme. Workers at risk were identified during the voluntary periodic occupational health examination which takes place every 2–5 years, depending on the age of the worker. Approximately half of the employees attend the examination.
The occupational physician was asked to fill out the validated selection instrument and to calculate the risk of work disability, based on the following risk factors: work ability, age, sickness absence over three months in the previous year and musculoskeletal complaints.17 The risk factors were used in a decision model to calculate the probability of long-term disability in the next four years for a particular construction worker, subject to a specific combination of these four risk factors. The a priori probability was set equal to the overall long-term disability risk among the youngest construction workers (<30 years) with a relatively short exposure history. Compared to excellent work ability, the risk estimate for work disability was set with the relative risk at 2.5 for good work ability, 5.4 for moderate work ability and 10.7 for bad work ability. Age-dependent risks were set at odds ratios of 1.5, 2.0 and 3.0 for the age groups of 30–34 years, 35–44 years and 45–54 years, respectively. A sickness absence period of ⩾3 months had an odds ratio of 2.0, and severe musculoskeletal complaints had an odds ratio of 3.0.17
All occupational physicians in the programme were provided with computer software to calculate the risk of long-term disability based on the four risk factors. According to the protocol, only workers with a probability of long-term disability in the next four years of 38% or higher would be advised to contact the labour market organisation for enrolment in the counselling and education programme. The decision to take a cut-off point of 38% probability for long-term disability during four years was taken in collaboration with social parties in the construction industry. This probability is currently put into practice and, in the upcoming years, will be evaluated as to its effect on disability rates in the construction industry.17
The advice of contacting the labour market organisation was given by the occupational physician who performed the periodic occupational health examination and calculated the risk on long-term disability. Referral to and participation in the programme was at discretion of the employee. Alternatively, employees eligible for the intervention group who felt they would benefit from the programme, but were not scheduled for the periodical health check-up nor selected based on the decision instrument by their occupational physician, could also sign up for the programme themselves. The work disability risk of this group was assessed before the start of the programme. A total of 195 employees in the intervention group participated in the counselling and education programme, of whom 83 (43%) were selected by their occupational physicians during the periodical health check-up on the basis of a high risk of ⩾38% on receiving a disability pension within four years, or enrolled themselves and were assessed with the same high risk. Only the 83 employees with a high risk were selected for this study.
Employees in the control group were not eligible for the counselling and education programme and received care-as-usual: they were invited for a periodical health examination and received all the medical and occupational healthcare they would need. Furthermore, they could participate in regular work-related courses. However, they were not evaluated using the decision model and could not participate in the individually tailored counselling and education programme. A random sample of 1000 employees in the control group was selected by taking every 13th employee on the list of all employees over the age of 40 years in the control group who took part in the periodic occupational health examination between 1 September 2002 and 1 December 2002. Of the 1000 employees who were randomly drawn from the control group, 998 employees provided data on work ability and disability risk of whom 209 (21%) were assessed with a high risk of ⩾38% on a disability pension and 789 (79%) had a risk lower than 38% on a disability pension in the next four years. Only the 209 employees with a high risk were selected for this study.
As well as the baseline questionnaire, three further questionnaires were sent to participants in the intervention programme and to the random sample of employees in the control group in December 2002, September 2003 and May 2004, which was 9, 18 and 26 months after the onset of the study, respectively.
Counselling and education programme
The aim of the counselling and education programme was the enhancement of the individual work ability and the prevention of a disability pension. The programme comprised an assessment interview, additional assessment of labour market capabilities, devising an individual education programme, executing the individual education programme and a follow-up programme. The individual counselling and education programme could involve educational courses, individual counselling and coaching at the workplace. Occupational relocation could also be the goal of the programme. The counselling and education programme took place during working hours and was executed by an independent labour market organisation. A fully executed programme lasted half a year. The project started on 1 April 2002.
Measurements
Data on current work situation and work ability were collected at baseline with the periodic occupational health examination questionnaire.18 In a standard situation, this questionnaire only includes questions on work ability for workers older than 40 years, so the employees in the control group also had to be >40 years. For the employees in the intervention group, the occupational physicians were asked provide these additional questions on work ability to all employees.
Current work situation included working (yes/no) or receiving a disability pension (yes/no). Work ability was measured with the Work Ability Index (WAI)19 20 which covers seven dimensions, each of which is evaluated with the use of one or more questions: current work ability (1 question), work ability in relation to job demands (2 questions), number of current diseases (1 question with 15 items), work impairment due to diseases (1 question), sick leave days during past 12 months (1 question), own prognosis of work ability in next two years (1 question) and mental resources (3 questions). The WAI is a reliable21 and valid22 measure of work ability with scores ranging from 7–49. Scores 7–27 indicate poor work ability in need of restoring, scores 28–36 moderate work ability in need of improving, scores 37–43 good work ability in need of supporting, and scores 44–49 indicate excellent work ability in need of maintaining. These work ability classifications have been used to calculate a high disability risk. Additionally, data on age, sex, job position and health problems were collected at baseline with the periodic occupational health examination questionnaire.18
Longitudinal data on current work situation, receiving a disability pension and work ability were collected with the three follow-up questionnaires. Additionally, the process variables of participation in a training programme aimed at the current work or in a retraining programme aimed at obtaining other work were assessed with these questionnaires.
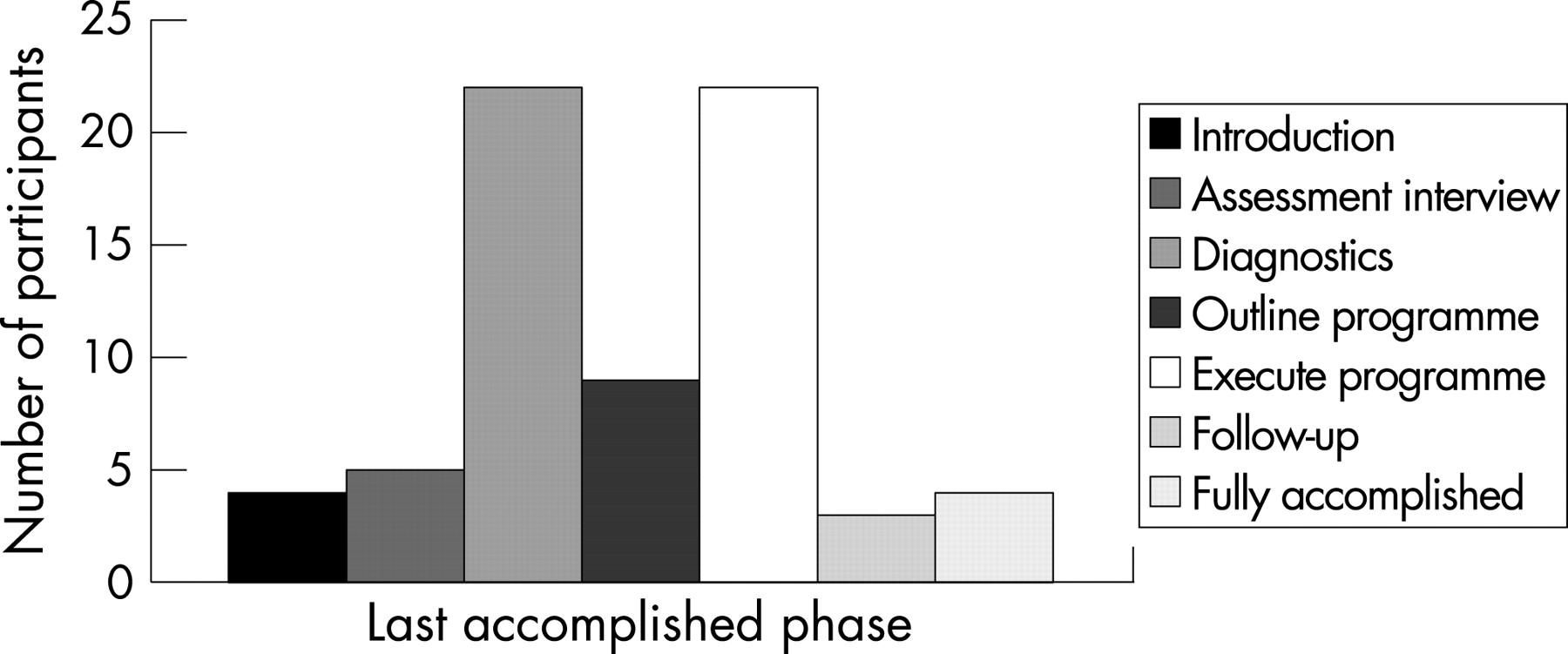
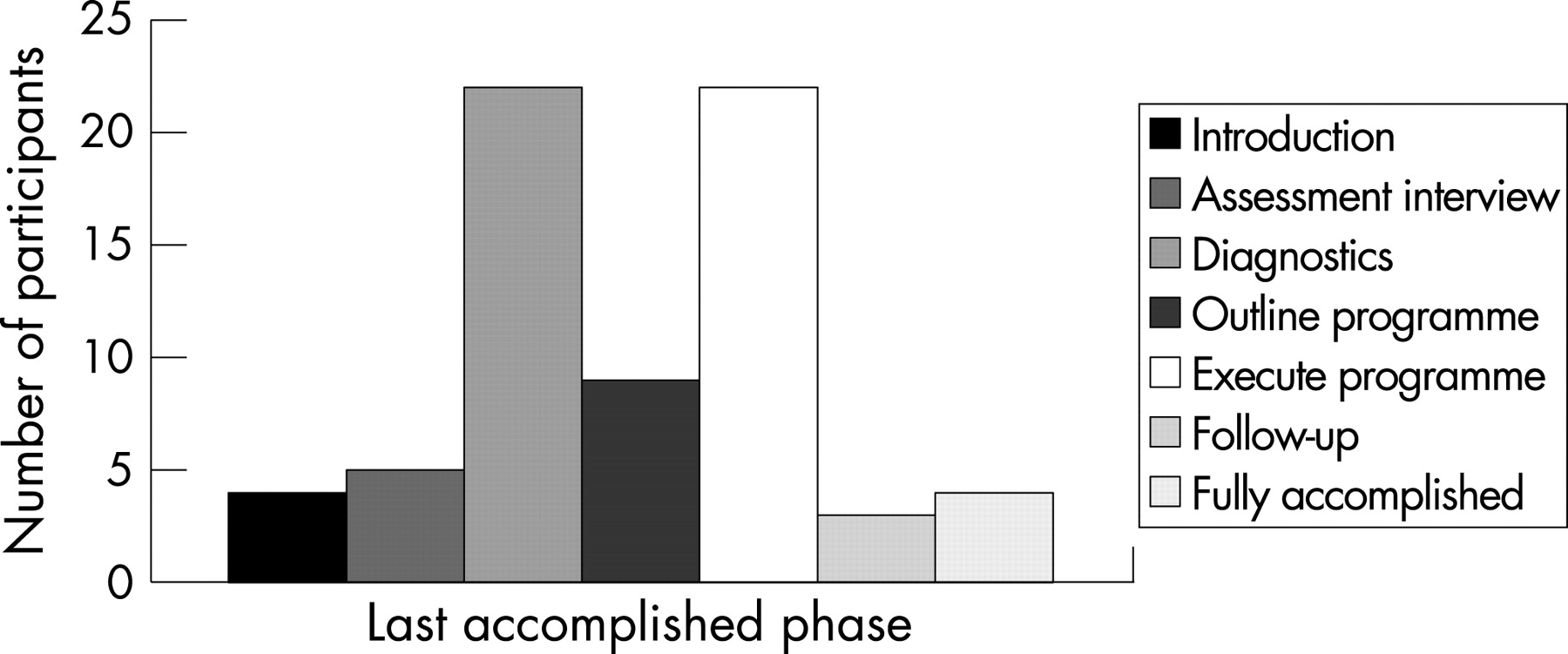
After the end of the project, the labour market organisation provided process variables on each participant in the programme which included participation in the following phases during the entire counselling and education programme: (1) introduction; (2) assessment interview; (3) further labour market capabilities assessment; (4) devising the individual training programme; (5) executing the individual training programme; (6) follow-up programme; or (7) accomplished programme (yes/no).
Statistical analysis
Only employees with a risk of long-term disability in the next four years of 38% or higher were selected from both the intervention and the control group for the analyses. Differences in baseline characteristics were tested with t tests for continuous variables and χ2 tests for categorical variables. The process variables were described. To assess if the programme was successfully executed, participation in the training programme was dichotomised as unsuccessful (phases 1, 2, 3, 4) and successful (phases 5, 6, 7).
Primary outcomes were work ability as measured with the WAI and work disability pensions. To analyse if providing the counselling and education programme had a subsequent effect on work ability, work ability scores in the intervention and the control group at 9, 18 and 26 months were analysed using a mixed-model analysis based on repeated measurements. To take possible differences in pre-test scores into account, the work ability score at baseline was entered as covariate. In all mixed model analyses, the main effects of time and the interaction effect of group×time were estimated. If an effect of the intervention on the WAI was found, separate analyses for the WAI dimensions of current work ability, work ability in relation to job demands, number of current diseases, work impairment due to diseases, sick leave days during past 12 months, own prognosis of work ability in next two years and mental resources was performed. A non-response analysis was executed in which the scores on the WAI at baseline were compared between the groups of employees who did and did not return the questionnaire at the second and third measurement.
The effect of the intervention on occurrence of work disability was evaluated with a generalised linear model, estimating the difference in disability risk between both groups, unadjusted and adjusted for age.
Differences in percentages with 95% confidence intervals were calculated based on the data gathered at 9, 18 and 26 months. All data were checked and analysed using the Statistical Package for the Social Sciences (SPSS 12) and SAS. A p value of <0.05 (two-sided) was considered statistically significant.
RESULTS
Subjects
Table 1 shows the baseline characteristics of the employees with a high risk of ⩾38% on receiving a disability pension within four years in the intervention (n = 83) and control group (n = 209).
The mean age of the participants in the intervention group was 43 years (range 19–58) while the mean age in the control group was 51 years (range 40–62) (p<0.001). The percentage of males in the intervention and control group was 99% and 97% respectively. Most employees in both intervention and control group were carpenters (43% and 37% respectively), bricklayers (7% and 15%), staff personnel (2% and 6%), and work foremen (both 5%).
A questionnaire was sent at 9, 18 and 26 months after the start of the intervention programme. At each time point, questionnaires were returned by 72%, 82% and 80% of those in the intervention group, and 76%, 86% and 87% in the control group, respectively.
Intervention programme and process variables
Figure 1 shows the last completed phase of the counselling and education programme for 69 participants in the intervention group (data missing from 14 participants). Several participants refrained from the programme after the introduction (6%) or the assessment interview (7%). A third of the employees left after the additional assessment of their labour market capabilities (32%) and an additional 13% after devising the individual training programme. Another third of the employees (32%) executed their individual programme and then left the programme, while some participants left during follow-up (4%) and some completed the entire programme (6%). Dichotomisation into successful completion of the programme (yes/no) resulted in 29 participants (42%) with a successful completion of the programme.
Nine months after the start of the programme, 11% of the employees in the intervention group indicated having participated in the last six months in a training programme aimed at their current work and 16% declared having participated in a retraining programme aimed at obtaining other work. After 18 months these percentages were 13% and 13%, and after 26 months were 9% and 13%, respectively.
Work ability
Figure 2 shows the WAI scores at baseline, 9 months, 18 months and 26 months for the employees who had a high risk on work disability in the next four years (>38%) at baseline. Employees in both the intervention (n = 83) and control group (n = 209) started with moderate work ability scores at baseline whereby the scores of the intervention group were statistically significantly (p<0.001) lower than those in the control group: 28.0 (SD 6.0) and 30.9 (SD 5.0). After correction for the baseline differences in WAI scores, results of the mixed model analysis showed no overall improvement over time (p = 0.52) and no differences in improvement over time between the groups, although the intervention group improved slightly more (p = 0.09). Analyses on the different dimensions of the WAI showed that this slight difference was caused by differences in the change of the dimensions work ability in relation to job demands (p = 0.012) and mental resources (p = 0.05), but not by differences in the change of the other dimensions. The non-response analysis comparing the scores on the WAI at baseline of the groups of employees who did and did not return the questionnaire at the second and third measurement indicated that there were no differences (p = 0.56 and p = 0.74, respectively).

{kind=link}
{kind=link}
Disability pension
The percentage of employees receiving a disability pension was analysed both with unadjusted data and adjusted for age. Table 2 shows that the overall percentages of employees receiving a disability pension were 3.1%, 6.4% and 8.3% at 9, 18 and 26 months, respectively. The percentage of employees receiving a disability pension in the intervention group increased more than in the control group, but no statistically significant differences in percentages of employees receiving a disability pension between the intervention and control group were found at 9 months (0.0% (95% CI −5.2 to 5.2)) or 18 months (5.7% (95% CI −1.1 to 12.5)). At the third measurement 26 months after the start of the programme, 17.9% of the employees in the intervention group versus 6.2% of the employees in the control group were receiving a disability pension, which was a statistically significant difference (11.7% (95% CI 4.6 to 18.7)). An additional age-adjusted generalised linear model analysis showed similar results: the age-adjusted estimated differences in percentages were 0.8%, 5.4% and 11.8%, but none of those were statistically significant differences (95% CI −4.8 to 6.5; −3.5 to 14.4; and 0.0 to 23.7, respectively).
DISCUSSION
The aim of this study was to evaluate if a counselling and education intervention programme for construction workers at high risk for disability pension could increase work ability and reduce future work disability pensions. A successful completion of the programme was achieved by almost half of the participants. Results showed that the work ability of participants in the intervention programme was lower at baseline than in the control group. The work ability of the employees in the intervention slightly improved over time while the work ability of the employees in the control group remained the same. However, when differences in baseline scores were taken into account, the improvement was not statistically significant.
The percentages of employees receiving a disability pension increased in both the intervention and control group. The difference in the percentages of employees receiving a disability pension was significant 26 months after the start of the programme, but when the data were adjusted for age, there was no statistically significant difference between the groups at any measurement point.
Interventions, be it on societal, organisational or individual level, need to be supported by evidence obtained through research.23 This study is one of few prospective controlled trials on prevention of early retirement in which the effect of the intervention on several outcome measures was investigated with a sufficiently long follow-up period.
However, a number of problems within the project were encountered. First, the selection of participants was found to be difficult. Fewer employees than expected were selected by their occupational physician via the selection instrument during the periodic occupational health examination. It might be possible that because it was outwith the daily practice of the occupational physicians to fill in the selection instrument and calculate the risk of work disability, they selected fewer patients than expected. Another possibility is that the intervention programme was offered to the employees but they chose not to engage in the project. Second, the majority of participants enrolled themselves in the programme. This self-enrolment shows a great need for our training programme from building industry employees but it resulted in fewer baseline data. Finally, a considerable number of participants did not complete the programme (57%). A possible reason for this non-compliance might be that the programme was too long. Another reason could be that the expectations of the employees did not match the content of the programme, because a third of the employees left the programme after the assessment of labour market capabilities.
With regard to the outcome measurements, work ability scores at baseline were lower in the intervention group compared to the control group, although those in the intervention group were younger and younger employees are known to have higher work ability scores.24 The WAI scores at baseline were 28 for the intervention group and 31 for the control group—both indicating moderate work ability in need of improvement.20 These baseline scores indicate that the selection process of the occupational physicians or the self-enrolment of the participants in the intervention group was appropriate because their work ability needed improvement. Moreover, these average baseline WAI scores of 28 and 31 were much lower than the average score of 40 of Finnish men in physical work, who were seven years older.24 However, the WAI selection instrument may be biased for workers aged over 55 years17 and this could have negatively influenced the effect of the intervention.
A positive finding of this study was that the work ability scores of the employees in the intervention group improved over time and the scores of those in the control group did not. Further analyses showed that this slight difference was caused by differences between the intervention and control group in the change of the dimensions of work ability in relation to job demands and of mental resources, but not by the other dimensions. It appears that the intervention programme resulted in a better fit of the workers’ capacities with their jobs and in improved mental resources, which included optimism, enjoyment and being active.
However, this slight improvement in work ability did not result in less disability. The age-adjusted percentages of employees in the intervention group receiving a disability pension did not differ to those in the control group at any point in time. Notably, at 26 months after the intervention the percentage of employees in the intervention group was almost statistically significantly higher than in the control group. One reason might be that the employees lost to follow-up were those receiving a disability pension. However, the non-response rates were similar in both groups, and non-response analysis showed that non-response was not related to work ability scores at baseline. Another possible reason is that the effect of the programme disappeared after two years and that follow-up sessions might be necessary to maintain the effect of the education and counselling programme.
It might also be possible that the prevention of work disability and the promotion of work ability started too late for this vulnerable group at high risk, as was also indicated by the high percentage of employees leaving the programme after the assessment of labour market capabilities. In that case, the individual counselling and education programme should start earlier and should therefore also be aimed at employees with an occupational disability risk of less than 38% in the next four years. Another possibility is that the intervention programme should have been more comprehensive for this high risk group to be more effective. Earlier studies showed that multidisciplinary interventions,13 25 early workplace interventions26 and organisational interventions27 are most effective in reducing disability pensions and sick leave days. Therefore, future research should put more emphasis on a comprehensive multidisciplinary approach and study a larger group of employees with a longer follow-up. An example of such a promising programme is the Swedish Galaxen model in which rehabilitation and prevention activities in the construction industry are provided. The model is multidisciplinary with representatives from the employers, trade union, employment office and professionals, and supplies the employee with a personal case manager.28 The Galaxen model therefore has more parties involved in the rehabilitation/disability prevention process than our programme and has more personal supervision.
Main messages
As construction workers are among those with the highest risk of work-related disability, interventions are needed that target workers at risk in order to prevent them from quitting the workforce.
In this study, employees with a high disability risk of 38% or higher in the next four years were randomised into an individual counselling and education programme or care as usual.
Work ability in the intervention group increased slightly more in the intervention group.
No differences in the age-adjusted percentages of employees receiving a disability pension were found between the groups at any measurement.
Policy implication
A more comprehensive multidisciplinary intervention programme might be necessary to reduce work disability pensions.
In conclusion, the counselling and education programme was slightly effective in improving work ability but not in reducing work disability pensions. Employees with a high risk for disability pension might need a more extended multidisciplinary intervention.
Acknowledgments
This study was supported by a grant from the social partners in the construction industry.
REFERENCES
Footnotes
Competing interests: None declared.
- Abbreviation:
- WAI
- Work Ability Index