Article Text

Abstract
Aims: To investigate time to pregnancy (TTP) in male lead workers in order to determine the dose-response relation between blood lead and decreased fecundity.
Methods: A total of 163 currently employed married male lead battery workers were classified into five categories of exposure based on questionnaire information and annual individual blood lead measurement. Information pertaining to the TTP was collected using personal interviews with 133 men and their spouses, with 280 valid pregnancies. The fecundability ratios (FRs) were calculated with the Cox discrete proportional hazard regression technique to evaluate the effects of lead exposure.
Results: After other factors associated with TTP were controlled for, there was a dose-response relation between blood lead level and TTP. The measured FRs were 0.90 (95% CI 0.61 to 1.34), 0.72 (0.46 to 1.11), 0.52 (0.35 to 0.77), and 0.40 (0.27 to 0.59) for concurrent blood lead levels of <20, 20–29, 30–39, and ⩾40 μg/dl, respectively. Paired self comparison was also performed for 41 couples that had pregnancies prior to lead exposure and pregnancies with male occupational lead exposure. The TTP was prolonged for 0.15 cycles by a 1 μg/dl increase in blood lead.
Conclusions: These results corroborate the hypothesis that a raised blood lead level affects fecundity. A blood lead level of less than 40 μg/dl may still significantly prolong TTP.
- AA, artificial abortion
- FR, fecundability ratio
- ICL, index of cumulative blood lead
- IUD, intrauterine device
- PbB, blood lead level
- SA, spontaneous abortion
- SD, standard deviation
- TTP, time to pregnancy
- fertility
- lead
- occupational exposure
Statistics from Altmetric.com
- AA, artificial abortion
- FR, fecundability ratio
- ICL, index of cumulative blood lead
- IUD, intrauterine device
- PbB, blood lead level
- SA, spontaneous abortion
- SD, standard deviation
- TTP, time to pregnancy
Toxic lead exposure is one of the most prevalent occupational and environmental health problems in the world today. Epidemiological studies have shown male reproductive toxicity such as semen quality and endocrine function,1–4 and male mediated adverse pregnancy outcomes such as spontaneous abortion, congenital malformation, and preterm birth.5–8 Some studies9–11 showed reduced fertility using a measure of fertility or infertility rate among males and families exposed to lead contamination, whereas another study12 did not. Moreover, three studies13–15 only revealed weak effects of decreased fertility using a measure of time to pregnancy (TTP) among the wives of the husbands exposed to lead contamination. There were limited and conflicting results between lead exposure and reduced fertility of the men, with no clear dose-response relation, especially at a threshold level.
Lead effect on human male fertility has been postulated to occur at blood levels greater than 40 μg/dl,3 which is the current occupational standard in the United States16 and many other countries, including Taiwan. The first evidence of such alterations at even lower blood lead level (PbB), for example, 20–50 μg/dl has, however, appeared in a few animal studies.17,18 Ng and colleagues2 also noted that luteinising hormone and follicle stimulating hormone showed a moderate increase in relation to PbB in the range 10–40 μg/dl. Circumstantial evidence suggests that occupational hazards of lead contamination may occur at less than the occupational threshold limit value of 40 μg/dl and may be associated with adverse effects on human sperm.19 However, Bonde and colleagues4 suggested that adverse effects of lead on sperm concentration and susceptibility to acid induced denaturation of sperm chromatin are unlikely at blood lead concentrations below 45 µg/dl. The lowest level of lead effect on male reproduction depends on different species or reproductive endpoints. Thus, we do not know whether a PbB of 40 µg/dl is enough to protect male workers in view of male and male mediated reproductive effects.
Because of the difficulty in obtaining human semen and the conservative nature of sexual norms in traditional Chinese culture, we selected the TTP of wives as a surrogate measure of male fecundity, as proposed by Baird and colleagues.20 TTP is considered to be an estimate of fecundity and is a composite measure of gametogenesis, transport of germ cells, fertilisation, transport of the embryo, and early survival of the fetus.21 The data pertaining to the TTP of wives collected using a brief questionnaire is valid at a group level with a recall time of 14 years or more.22 Disadvantages, however, include susceptibility to recall and selection biases,23 and the need for data pertaining to several potential confounders.20 Thus, avoidance of biases and control of confounding are crucial to any empirical study using TTP.
This study was conducted, retrospectively, in a face-to-face collection of TTP information from couples whose husbands were exposed to lead in their occupations within a broad range. The aim of the study was to determine the dose-response relation between blood lead and decreased fecundity, and investigated whether a PbB of 40 μg/dl provides adequate protection to lead workers.
METHODS
Study design and subjects
TTP was studied among the wives of men biologically monitored for exposure to lead. The study population consisted of all 163 married male workers employed at a lead battery plant of Taiwan in November 1998. All study participants provided informed consent, which was approved by the National Taiwan University College of Public Health Ethic Review Board. We conducted face-to-face interviews with all married male workers and their wives. At the plant, we interviewed each man first to gather the information on his demography, occupation, lifestyle, and past medical history. Our research physician and nurse then conducted a face-to-face interview with each worker’s wife at home with inquiries relating to pregnancies or infertility histories during the period 1984–98.
Main messages
-
The present study corroborates the hypothesis that decreased fecundity is significantly associated with male exposure to lead when concurrent blood lead level is less than 40 μg/dl.
Exposure assessment
Every worker was required to have blood lead levels checked during an annual health examination. The blood lead content was measured using inductively coupled plasma mass spectrometry (ICPMS) in a clinical laboratory at the Taipei Veteran’s General Hospital. The laboratory has regularly participated in our national quality control programme for blood lead determination since 199024 and serves as one of the reference laboratories in Taiwan.
The employment history and lead level were used as the basis for exposure categorisation. There were 153 TTPs without exposure and 127 TTPs whose husbands were exposed to lead. Among those with lead exposure, male exposure to lead was assessed within 80 days (the estimated period of spermatogenesis) prior to the time unprotected intercourse began. However, 53 occurred outside the period of blood lead sampling, and we used the average blood lead concentration before and after the TTP. TTPs were categorised into five groups based on blood lead concentrations (the concurrent PbB at the beginning of the calendar year when TTP started): non-exposed (pregnancy occurred prior to husband working in lead exposure environments); low (blood lead <20 μg/dl); moderate (blood lead 20–29 μg/dl); high (30–39 μg/dl); and very high exposed (⩾40 μg/dl).
We also estimated the index of cumulative blood lead level (ICL) before the beginning of the calendar year when the TTP started.25 Briefly, the ICL was calculated by the following formula: ICL = [∑0.5(PbBi+PbBi+1)Δti], expressed in μg/dl; it represented the cumulative dose of lead exposure between the beginning of employment and at the beginning of the calendar year when the TTP started.
Questionnaires
One of the key questions on the waiting time to pregnancy was phrased as follows: “How many menstrual cycles did it take to get pregnant after you had practised regular sexual intercourse without using any method of birth control?”.26 We asked about the last method of birth control and the exact time they stopped the practice to validate the exact TTP. If they used intrauterine devices, the TTP data were collected only when regular menstrual cycles could be ascertained after the intrauterine devices were removed.27 We also tried to confirm the date of first unprotected pregnancy. Somewhat predictably, since most Taiwanese women are unaware of their husbands’ occupational exposure rates,28 none in this survey knew the blood lead levels of their husbands. They also did not know our study objective—the relation between lead exposure and fertility. Moreover, our interviewers did not know the women’s husbands’ PbB levels before interview. Thus, our assessment of TTP was blind to the level of exposure.
Data on previous medical and occupational histories, and lifestyle factors such as smoking, and use of alcohol, tea, or other caffeinated beverages during each TTP for each couple (both husband and wife) were collected. In particular, husbands were asked about any illness or condition that could impair their ability to become a father, such as parotitis, orchitis, varicocele, or major systemic diseases. Wives were asked about their previous history: age at menarche, duration of the menstrual cycle, any treatment for menstrual irregularity, infertility, pelvic inflammatory disease, or endometriosis, and major abdominal surgery. Additional data on employment status and the main job tasks of the wife were collected for 12 months preceding each pregnancy. We also collected detailed data on the following potential confounding variables: men’s and women’s age at the beginning of pregnancy, exact date for each pregnancy, pregnancy sequence, and outcome.
Policy implications
-
The current occupational standard, 40 μg/dl, for blood lead does not provide adequate protection for male workers in light of the reproductive health considerations.
Inclusion and exclusion criteria
Thirty male workers were excluded because of difficulty to recall accurate TTP for the following reasons: spouse deceased or divorced (n = 3, including 5 live births), four couples diagnosed as infertile (one husband with varicocele, three with unknown causes but failure to become pregnant within 24 menstrual cycles), spouses with previous habitual abortions (n = 3, including 2 live births and 10 spontaneous abortions), spouses with irregular menses (n = 1, including 2 live births), and having the last delivery more than 14 years previously (n = 19, including 64 live births).
A total of 133 couples were thus included, consisting 321 pregnancies (fig 1). Forty one pregnancies were also excluded because of potentially large measurement errors or biases: inability to recall accurate TTP (19 pregnancies with 8 in the non-exposed group and 11 in the exposed group), contraceptive failures or unplanned pregnancies (18 pregnancies with 11 in the non-exposed and 7 in the exposed group), vaginal spotting found after stopping the use of an intrauterine device for longer than two months (2 pregnancies), and wives with endometriosis (2 pregnancies). The remaining 280 pregnancies qualified for analysis, which included 18 artificial abortions, two stillbirths (1 in the exposed and 1 in the non-exposed group), eight spontaneous abortions (4 in the exposed and 4 in the non-exposed group), and 252 live births.

Process of case selection. Numbers in parentheses indicate numbers of pregnancies. AA, artificial abortion; SA, spontaneous abortion; ?, unknown.
Statistical analysis
The outcome variable is the TTP; the exposure variables include males exposed to lead at the beginning of the calendar year when TTP started (five levels), ICL (four levels), and female lead exposure at the beginning of the calendar year when TTP started (yes/no). The potential confounding variables related to TTP included factors for males such as age at the beginning of TTP, use of tea or coffee, use of alcohol, and smoking, and female factors such as age at the beginning of TTP, use of tea, use of alcohol, smoking, contraceptive use before TTP, age at menarche, shift at work, calendar year of pregnancy, and pregnancy sequence.
Fecundability denotes the probability of obtaining a clinically recognised pregnancy in a menstrual cycle among couples not pregnant during previous cycles. The fecundability ratio (FR) measures the odds of a conception among the exposed divided by the odds among those not exposed. FRs were calculated with 95% confidence intervals (CIs) using the Cox proportional hazards regression model with discrete ties29 to evaluate the effect of lead exposure. We censored TTPs of more than 13 cycles to avoid medical intervention, and because 97.5% of TTPs conceived within one year of unprotected intercourse. In the multiple regression models, we used a change-in-estimate criterion to identify confounding variables. We included multiple pregnancies per couple, violating the assumption of independence and causing underestimation of the variance. Thus, we also randomly selected one pregnancy per couple and restricted the first pregnancy only in the models.
Moreover, we conducted a self comparison analysis for couples with a pregnancy before lead exposure and another one after the exposure. The difference in TTP between the two pregnancies was used as the outcome variable, and male lead levels at the beginning of the TTP and ICL of the later pregnancy were used as exposure variables for constructing linear regression models.
RESULTS
Table 1 shows no significantly different distribution of various pregnancy outcomes stratified by blood lead levels in men at the beginning of the calendar year when time to pregnancy started. The distributions of TTPs by PbB categories in men revealed that wives of men with higher blood lead levels generally took more cycles to become pregnant (table 2). The trend can further be visualised in fig 2, in which the cumulative distribution of TTP showed a shift-to-right phenomenon as blood lead levels increased.
Frequency distribution of various pregnancy outcomes stratified by blood lead levels in men at the beginning of the calendar year when time to pregnancy started
Distribution of time to pregnancies in menstrual cycle and potential confounding factors by blood lead level in men at the beginning of the calendar year when time to pregnancy started
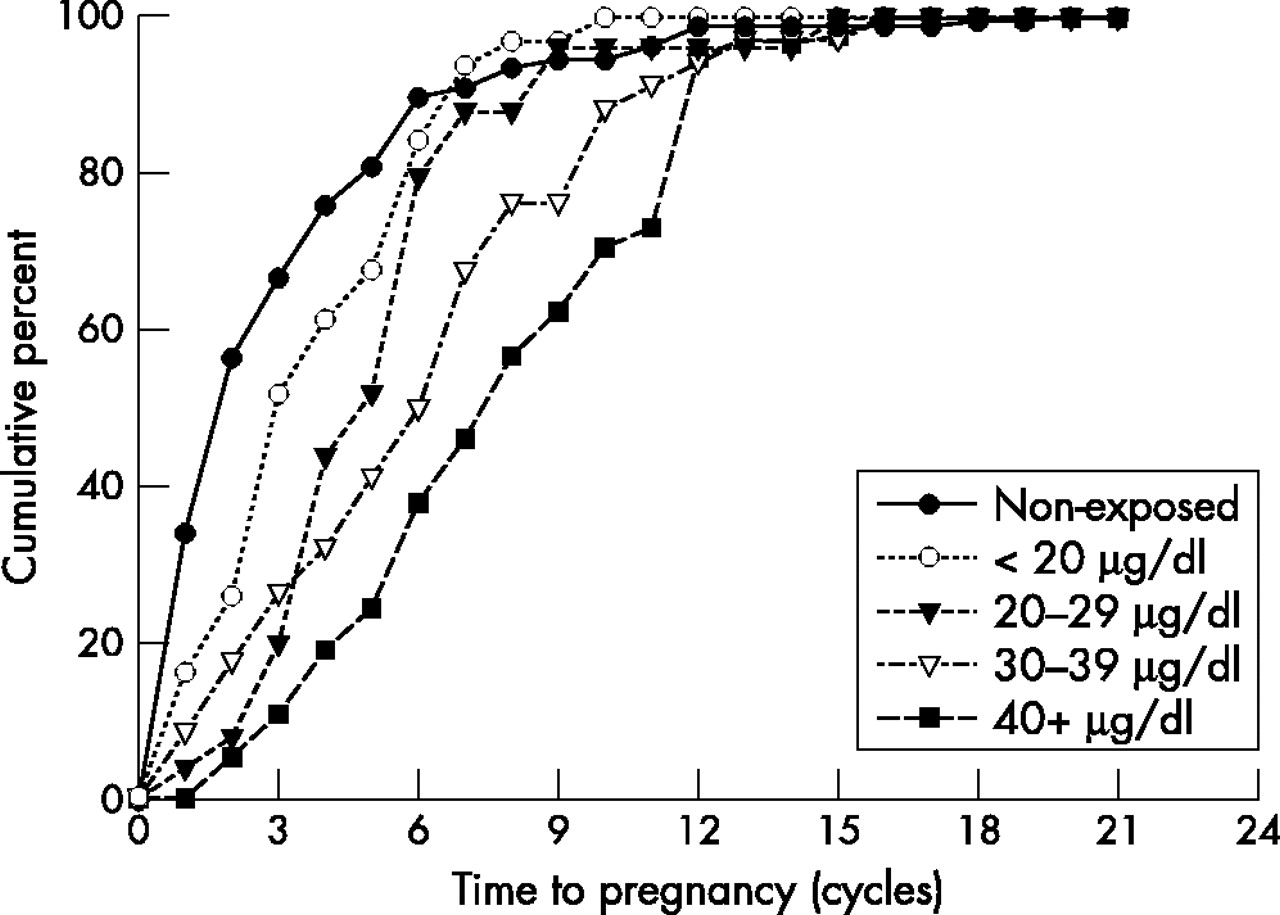
Cumulative distribution of time to pregnancy by blood lead categories in men at the time when time to pregnancy started.
Table 2 also shows the distribution of potential confounding factors by blood lead level in men at the beginning of the calendar year when time to pregnancy started. Table 3 lists the distribution and crude FRs for all variables being potentially associated with the pregnancy outcomes. Lead exposure in both men and women was significantly associated with decreased fecundability, while none of the other factors showed a statistically significant association with TTP.
Crude fecundability ratios according to lead exposure and potential confounding factors; univariate Cox discrete proportional hazard models
The FR decreased with successively higher male blood lead levels, significant at 30 μg/dl (FR = 0.50, 95% CI 0.34 to 0.74) and ⩾40 μg/dl (FR = 0.38, 95% CI 0.26 to 0.56) for all valid pregnancies (table 4). Furthermore, maternal exposure to lead showed decreased FR although it was not statistically significant (FR = 0.61, 95% CI 0.37 to 1.01; p = 0.06). When algorithms restricted the analysis to the first TTP or a randomly selected pregnancy in each couple, the effect of lead exposure still showed consistent results with minor changes. Interaction in terms of lead exposure in men and women was also attempted but no significant interaction effect was found. Moreover, we also found similar results using ICL in multivariable models (data not shown).
Adjusted fecundity ratio according to lead exposure and confounding factors; multivariable Cox discrete proportional hazard models
For the 41 couples with at least one pregnancy before exposure to lead content in an occupational environment in men and another pregnancy after working at a lead plant, there was a prolonged TTP difference due to lead exposure. The TTP difference was prolonged for 0.15 cycles when PbB in men increased by 1.0 μg/dl (R2 = 0.62, p < 0.0001) (fig 3). However, no significant result was found using ICL in the models (data not shown).

{kind=link}
{kind=link}
{kind=link}
The relation between blood lead levels in men and difference between time to pregnancies (TTPs). Solid line represents the linear regression and dotted lines represent the 95% confidence intervals.
DISCUSSION
Although male blood lead levels below 40 μg/dl may impair fecundity in animal experiments,17–19 no human epidemiological study has supported this.13,14 To our knowledge, this study is the first to show that decreased fecundity or prolonged TTP is significantly associated with PbB less than 40 μg/dl in men regardless of the lead level representing the exposure when TTP starts. ICL also shows a statistically significant determinant in the likelihood ratio test but does not illustrate a linear association on its plot against difference between TTPs. We believe that the concurrent blood lead level in men, instead of cumulative lead (ICL) exposure, is the major factor associated with reduced fecundity.
We note the following reasons, however, to argue for the probable causal relation and the need for consideration to lower the occupational standard for blood lead levels. First, we have put all the major potential confounders reported into our multivariable modelling strategy, including cigarette smoking,30,31 alcohol consumption,32 use of coffee or tea,33 age at the beginning of TTP,34 pregnancy sequence,35 and maternal lead exposure.36 As the typical Taiwanese culture is not conducive for women who smoke or drink, both were not prevalent among the women in this study. Thus, none of these factors can explain the association.
Second, the assumption of statistical independence may be violated because of an underestimation of the variance when the study included more than one TTP estimate per couple. To evaluate this potential bias, we restricted the analysis to the first pregnancy or one randomly selected pregnancy from each couple in the models. Although the sample sizes are thus decreased in each exposure group, the effect is still consistent.
Third, we have deliberately eliminated all TTP related biases through a careful study design.23 Women in this study were unaware of their husbands’ PbB, and we have verified each question of the interview data as conducted by the same interviewer, resulting in minimal bias. To prevent possible planning bias, we have excluded 18 unprotected pregnancies, 5.5% (7/127) for the exposed group and 7.2% (11/153) for the non-exposed group. Bias due to medical intervention or unhealthy worker effects was eliminated by excluding four couples undergoing infertility treatment. Pregnancy recognition bias was avoided after the exclusion of one couple with extreme irregular menses and three couples with a previous history of habitual abortion. Because the accessibility of medical services has been well documented for workers and their families in Taiwan since 1995,37 the pregnancies of our subjects were all verified by an obstetrician instead of by home pregnancy test available at local pharmacies. Moreover, we have excluded 19 pregnancies with no accurate TTP, to minimise recall bias of TTP.
Fourth, while most European retrospective TTP studies might suffer from time trend bias38 (that is, blood lead levels consistently decreased during the observation period), our series did not exhibit such a trend. The annual average blood lead (mean (SD)) levels for men in this study from 1987 to 1999 were 36 (12), 33 (10), 38 (13), 38 (18), 38 (15), 35 (13), 41 (17), 33 (15), 35 (17), 32 (15), 39 (14), 35 (14), and 32 (12).
Finally, we have conducted a self comparison for 41 couples that experienced at least one pregnancy prior to lead exposure and another pregnancy with male exposure at the lead plant. However, PbB in men was the only significant factor associated with prolonged TTP in the models. This effect remained even after eliminating pregnancies wherein couples were both exposed. Lead toxicity has been associated with impaired semen quality and endocrine function in both human and animal studies;19 it is biologically plausible that human exposure may prolong TTP. Based on this study, the magnitude of prolongation is 0.15 cycles per 1 μg/dl increase in blood lead concentration, beginning at the level of 10 μg/dl.
The most frequently addressed disadvantage in this study is that the baseline blood lead levels for non-exposed subjects have not been measured. Underestimation of the effect from lead is of concern. Concurrent exposure to other agents, for example, cadmium or other heavy metals is unlikely in a battery factory. Furthermore, the gradual increase in endocrine disrupters from other environmental pollution39 may also constitute some kind of superimposed damage to the human reproductive system and push effect measurement towards null values. If the misclassification in exposure status is dismissed, the measured FR would be strengthened.
Joffe and colleagues22 reported that the TTP collected using a brief questionnaire is valid at a group level with a median recall time of 14 years in England. We used the same collection methods with our semiconductor study,26 which included a face-to-face interview with women and our interviewer team, blinded to occupational exposure. Moreover, the exclusion of spouses with irregular menses or endometriosis, couples diagnosed with infertility or previous habitual spontaneous abortion, and unplanned pregnancies can avoid inaccurate measurement of TTPs, and although it may underestimate the effects of lead exposure, these exclusions can reduce recall bias to a minimum.
Our results showed lower figures of couples with a diagnosis of infertility, spontaneous abortion, and unplanned pregnancy (fig 1). The couples usually seek a doctor for fertility problems with no childbirth after at least two years of preparation for pregnancy in Taiwan. We excluded the couples with a diagnosis of infertility only, to take account of medical intervention for infertility. Another consideration might be a healthy worker effect. That is, married couples usually attempt conception after marriage according to Chinese custom; thus those with infertility problems will not work in lead exposed plants. Our estimate should be lower than the suspected primary infertility rate (6.0%) in Taiwan.40 The healthy worker effect may give a lower rate of spontaneous abortion; furthermore, the Chinese culture for childbirth may explain a lower rate of unplanned pregnancies.
Although the frequency of intercourse is associated with probability of conception, it has been suggested that it is not essential to collect such information for studies of fecundability.41 If intercourse information is not available, this may obscure reproductive effects of an agent that affects the libido. Although we attempted to collect this information, we are concerned that the quality may be poor. Taiwan is a traditional Chinese culture in which the measurement of sexual life is difficult. Imprecision using this data will tend to produce non-differential misclassification.
Our findings are inconsistent with three previous TTP studies in men exposed to lead at similar exposure levels. Apostoli et al found that a statistically significant longer TTP was associated with an exposure level of at least 40 μg/dl.13 Sallmén et al found that men with blood lead concentrations above 30 μg/dl had relatively lower fertility, but no clear dose-response relation existed.14 On the other hand, Joffe et al found no detectable effect on male fertility in European worksites.15 The effect found in this study appears to be a dose-response relation between blood lead and decreased fecundity. Although the reasons for the discrepancies among the findings in the different studies are unclear, face-to-face interviews with workers and their wives to collect data on TTP and other related factors are worth mentioning in this study.
We also found that the workers exposed to lead with delayed pregnancies caught up after 12 months (fig 2). Although we excluded the couples with a diagnosis of infertility, this would imply that the prevalence of infertility did not increase in men exposed to lead at these levels. The findings do not conform with the recent study by Bonde and colleagues,4 indicating that there was no linear trend of lower sperm concentration with increasing blood lead, and sperm count does not reduce at exposure levels below 45 μg/dl. However, the latter study focused on sperm count and sperm chromatin structure other than seminal characteristics such as morphology or motility or male mediated reproductive effects as early fetal losses, which might also be adversely effected by lead exposure and have an impact on the fecundability.
Our data also support the contention that concurrent blood lead level is a more adequate indicator for reducing male fecundity than cumulative lead exposure. One of the possible reasons could be that the ICL could not differentiate between short term high exposure and long term low exposure. Since the half-life of lead in blood is about 28–30 days,42 if there were any cumulative effect of lead on reproduction, relying on blood concentrations alone would be insufficient.
The present study corroborates the hypothesis that decreased fecundity is significantly associated with male exposure to lead when the concurrent blood lead level is less than 40 μg/dl. The current occupational standard, 40 μg/dl, for blood lead does not provide adequate protection for male workers. The appropriate blood lead level for men requires exploration in the light of reproductive health considerations.
Acknowledgments
We are grateful to Mrs Lih-Jane Huang and Ms Lih-Huey Chen for their help with data collection and are indebted to Fung-Chang Sung, PhD, Institute of Environmental Health, National Taiwan University College of Public Health, for his welcome comments during drafting.
REFERENCES
Footnotes
-
Funding: This study was supported by grants from National Health Research Institute (DOH88-HR-504 and NHRI-GT-EX89P504P) and National Science Council (NSC91-2320-B-002-168), Taiwan.
Linked Articles
- Work in brief