Article Text

Abstract
OBJECTIVES To study the dose-response relation between cadmium dose and renal tubular damage in a population of workers and people environmentally or occupationally exposed to low concentrations of cadmium.
METHODS Early kidney damage in 1021 people, occupationally or environmentally exposed to cadmium, was assessed from cadmium in urine to estimate dose, and protein HC (α1-microglobulin) in urine to assess tubular proteinuria.
RESULTS There was an age and sex adjusted correlation between cadmium in urine and urinary protein HC. The prevalence of tubular proteinuria ranged from 5% among unexposed people to 50% in the most exposed group. The corresponding prevalence odds ratio was 6.0 (95% confidence interval (95% CI) 1.6 to 22) for the highest exposure group, adjusted for age and sex. Multiple logistic regression analysis showed an increasing prevalence of tubular proteinuria with urinary cadmium as well as with age. After adjustment to the mean age of the study population (53 years), the results show an increased prevalence of 10% tubular proteinuria (taking into account a background prevalence of 5%) at a urinary cadmium concentration of 1.0 nmol/mmol creatinine.
CONCLUSION Renal tubular damage due to exposure to cadmium develops at lower levels of cadmium body burden than previously anticipated.
- cadmium
- environmental
- tubular damage
Statistics from Altmetric.com
Exposure to cadmium may cause kidney damage.1-3 The cumulative exposure to cadmium and its concentration in the kidneys can be assessed by measuring cadmium in urine.4 The initial sign of cadmium induced renal lesions is tubular proteinuria, usually detected as an increased urinary excretion of low molecular weight proteins, such as β2-microglobulin, retinol binding protein (RBP), protein HC (α1-microglobulin), or enzymes such as N-acetyl-β-glucosaminidase (NAG).5-7 If exposure to cadmium continues the tubular dysfunction progresses and glomerular damage with a decrease in the glomerular filtration rate (GFR) may emerge.1 7 Also, secondary effects on the bone and calcium metabolism may occur causing renal stones, and in cases of severe cadmium poisoning osteoporosis and osteomalacia with the infamous itai-itai disease as the final stage.3 7 8 In recent years it has been recognised that signs of early tubular damage can develop at relatively low cumulative doses of environmental cadmium.7 9
In an extensive cross sectional study of more than 1000 people living in two communities (Fliseryd and Oskarshamn) in a region in the south of Sweden, with a range of relatively low exposures to cadmium, we have examined the association between dose of cadmium and the prevalence of early tubular damage and osteoporosis—the osteoporosis, cadmium as a risk factor (OSCAR) study. Nickel-cadmium batteries have been produced in the region since 1910. The plant in Fliseryd was closed in 1974, whereas the factory in Oskarshamn is still operating. Occupational exposure to cadmium was high during the 5 five decades of operation at the plant, but has gradually decreased since the 1960s.10 11 Environmental cadmium pollution from these plants was substantial in the past, in particular in the vicinity of the Fliseryd plant. Here we present data on cadmium and early tubular effects whereas results from measurements of bone density are reported elsewhere.11a
Methods
The study population included all people between 16 and 80 years of age, who had lived for at least 5 years and were still living in the area close to a nickel cadmium battery plant in southern Sweden between 1910 and 1992 (n=1259). A group of separately selected battery workers (n=242), was also included in the study population. A further group (n=206), matched by age and sex to the population who had lived close to the plant, was randomly selected from a general practice register in a nearby area. This group was initially intended as a reference population, but it was later discovered that there was great overlap in exposure between the two non-occupational groups, and thus these groups were merged into one environmentally exposed group (n=1465). All subjects in the study population were asked to participate. Of the environmentally exposed people 904 (62%) and of the battery workers 117 (48%), agreed to take part in the examinations. Thus, a total of 1021 people (60%) agreed to participate in the OSCAR study and gave their informed consent to the investigation. A telephone survey of a random sample of 5% of the non-participants indicated that they did not differ from the participants in a systematic way for age, sex, or morbidity.
Each study subject received a questionnaire requesting information about employment, residences, smoking, and food as well as medical history, especially kidney diseases and diseases related to osteoporosis. Morning urine was voided in acid washed polyethylene bottles and stored frozen (-20°C) until transfer to the analytical laboratory at the Department of Occupational and Environmental Medicine at Lund University Hospital. At the laboratory, the sample was thawed and 10 ml urine was poured into a polypropylene tube. After addition of 0.2 ml nitric acid, the tube was freeze stored until the measurement of cadmium. Subsamples for the measurement of protein HC were pipetted from the sampling bottle into separate tubes and freeze stored until analysis. The subsample for protein HC measurement was mixed with a preservative solution as described by Tencer et al.12
Cadmium in urine was measured by inductively coupled plasma mass spectrometry (ICP-MS). A quadropole spectrometer (VG PQ2+, Fisons Elemental, Winsford, Cheshire, UK) equipped with an autosampler (Gilson 222, Gilson, Villiers, France) was used. The samples (0.50 ml urine) were diluted 10 fold with a solution containing EDTA (0.5 g/l), Triton-X100 (0.5 g/l), and ammonia (5 ml/l) in Millipore water, and 100 μl of an internal standard solution containing 50 ng of indium (In) was added. All samples were prepared in duplicate. Spiked urine samples, at three concentrations, were used for method calibration. The isotopes 114Cd (and 118Sn for correction of interference from 114Sn) and 115In were monitored in pulse counting, peak jumping mode (three points per peak). The detection limits (calculated as 3SD for reagent blanks) varied between 0.01–0.04 μg/l from day to day. The precision of the method, calculated as the coefficient of variation for the duplicate measurements, was 8%. The method accuracy was checked by including commercial reference urine samples (Seronorm, Nycomed, Oslo, Norway) in each analytical series. The results agreed well with the recommended values in both low and high ranges of urinary cadmium concentrations and there were no time trends in the recoveries. Adjustments for variation in urinary concentrations between people were made by dividing the urinary cadmium values by the creatinine concentrations.4
Urinary protein HC (α1-microgloubulin) was used to detect early renal damage with single radial immunodiffusion for the measurements. The sensitivity of the method was 1.7 mg/l and its total analytical imprecision (within + between assay variation) 6%. The analyses were made at the Department of Clinical Chemistry at Lund University Hospital. The cut off points used for tubular proteinuria were 0.8 mg protein HC/mmol creatinine for men and 0.6 for women, which reflects the upper 95% limit in a Swedish reference population.13
STATISTICAL METHODS
Data were analysed with standard statistical methods, with STATISTICA software. Odds ratios (ORs) and 95 percent confidence intervals (95% CIs) were computed with stratified analyses and multiple logistic regression by EGRET software.
UNITS
For cadmium in urine 1 nmol/mmol creatinine=1 μg/g creatinine.
Results
Age and sex as well as urinary excretion of cadmium and protein HC in the study population are shown in table 1.
Characteristics of the population examined
A positive, highly significant, linear relation was found between dose (cadmium in urine) and effect (urinary protein HC) after adjustment for age for both sexes (table 2). The table shows the regression coefficients for the independent variables age and urinary cadmium, with protein HC as the dependent variable.
Dose-effect relation between urinary cadmium and urinary protein HC for men (n=469) and women (n=532), adjusted for age2-150
A total of 171 people had increased protein HC concentrations in urine with a clear dose-response relation between urinary cadmium and the prevalence of increased protein HC in urine as shown in table 3. During the course of investigation it was discovered thatseveral (n=105) environmentally exposed people also had worked in the battery plant. These people were therefore transferred to the occupationally exposed group, which thus increased to 222 people.
Tubular proteinuria (defined as excreting protein HC >0.8 and 0.6 mg/mmol creatinine, for men and women, respectively) in people exposed to cadmium
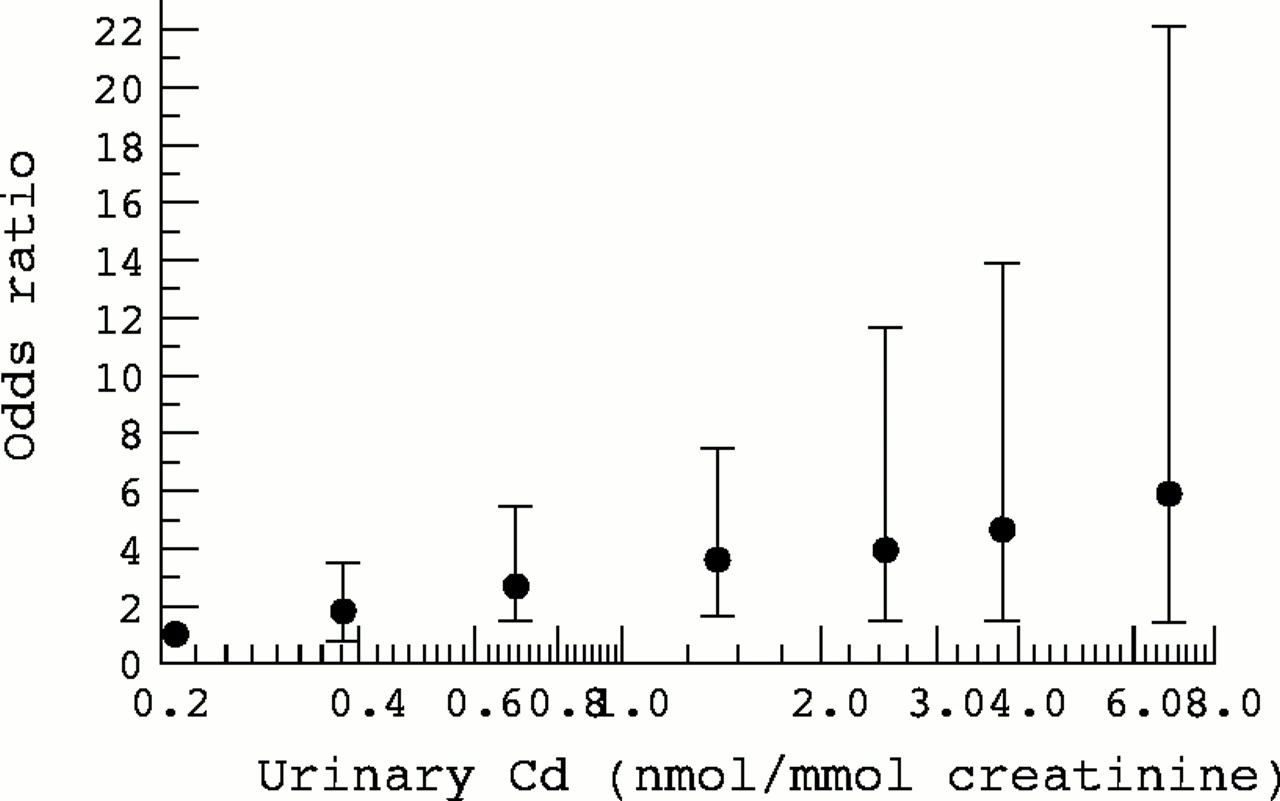
The dose-response relation remained even when the occupationally exposed people were excluded. The figure shows the ORs for increased urinary protein HC relative to increasing urinary cadmium after adjustment for age and sex.

{kind=link}
Odds ratios (95% CIs) for prevalence of tubular proteinuria related to urinary cadmium in Swedish people exposed to low concentrations of cadmium.
Multiple logistic regression analysis, including age and urinary cadmium as independent variables and normal or increased urinary protein HC as the dependent variable was used to establish dose response relations at different ages. Given the mean age of the study population (53 years) an increased prevalence of tubular proteinuria of 10% was calculated to occur at a urinary cadmium concentration of 1.0 nmol/mmol creatinine. Here we have accounted for a normal background prevalence of increased urinary HC of around 5%, and thus the total measured prevalence of tubular proteinuria at a urinary cadmium concentration of 1.0 nmol/mmol creatinine would be 15%.
Discussion
The present study shows that tubular proteinuria occurs in environmentally exposed people at lower concentrations of cumulative cadmium doses than was previously realised. People with cadmium in urine of around 1 nmol/mmol creatinine (which is in the upper part of the normal range) had a threefold increase in risk of having increased urinary protein HC (figure). The OR for increased urine HC is increased more than fivefold at urinary cadmium concentrations above 5 nmol Cd/mmol creatinine, which has been recommended as a health based limit by an expert group within the World Health Organisation (WHO).
Both age and urinary cadmium affect urinary protein HC excretion (table2) and therefore age should be considered when dose-effect and dose-response relations are being analysed. Based on our data, a 10% increase in urinary protein HC would be expected in a population, with a mean age of 53, at a cadmium concentration in urine of 1.6 nmol/mmol creatinine.
One strength of our study is that we have been able to collect and analyse urine samples, with sensitive methods, from a large population with exposures to cadmium close to the normal range. In most countries the normal urinary excretion of cadmium is in the range 0.1–0.6 nmol/mmol creatinine.1 7 When more sensitive methods for detecting tubular damage are used, early and subtle effects from the accumulation of cadmium are shown.14 When a very sensitive biomarker of effect (such as protein HC) is used, the clinical implication of increased urinary excretion is limited. However, as will be discussed later, subtle tubular damage is the beginning of a pathological process, which may end up in renal failure and secondary manifestations on the bone and mineral metabolism.7
Most previous studies have used β2-microglobulin as the marker of tubular dysfunction. A major problem with β2-microglobulin as a biomarker in large epidemiological studies is the instability of the protein in acidic urine. More sensitive markers have, however, been found. In particular, protein HC has been shown to be a sensitive and reliable marker of early tubular damage.15-17 In a recent European collaborative study aimed at identifying early indicators of cadmium toxicity, the most sensitive indicators of nephrotoxicity were found to be protein HC, NAG, thromboxane B2, and RBP.18 The cut off points for tubular dysfunction were taken from a rather limited reference material, based on a population living in a region not far from the study area.13 It should be noted that the cut off points correspond to the 95th percentile in the reference population, and thus 5% of the study population should be expected to have values exceeding the cut off point. This has been taken into consideration in the interpretation of the results.
To obtain a wide range of cadmium exposures (facilitating the dose-response analyses) we included environmentally as well as occupationally exposed people. However, as shown in table 3, exclusion of all people with previous occupational exposure did neither affect the overall results nor their interpretation. The lower response rate among the battery plant workers might have introduced a bias, if the non-participants had different characteristics than the participants. However, as noted in the methods section, a survey of a random sample of the non-participants gave no indication that they differed from the participants in a systematic way for age, sex, or morbidity. Furthermore, the ORs for the environmentally exposed group were similar to those obtained when the occupationally exposed workers were included in the analysis (table 3).
In other parts of the world, where cadmium has contaminated the environment, increased concentrations of cadmium in urine and renal tubular effects have been recorded among residents.1-3 7During the past decade, several studies of both occupationally and environmentally exposed populations have shown that tubular proteinuria occurs at doses of urinary cadmium of 2–4 nmol/mmol creatinine.9 11 19 20 In a large study on environmentally exposed people in Belgium a 10% prevalence of tubular proteinuria was found at 2 nmol Cd/mmol creatinine, not adjusting for age.9 The present study is in agreement with these findings with a 10% prevalence of tubular proteinuria at 1.6 nmol Cd/mmol creatinine adjusted to the mean age of the study population.
Kidney function, at least glomerular filtration, normally deteriorates with age21 and pathological changes of the renal vessels, nephron, and the interstitium become more prevalent with increasing age.22 Cadmium accumulates in the kidney with increasing age, and age may thus constitute an important effect modifier when examining long term health effects of cadmium exposure. The effect of aging itself on normal urinary excretion of β2-microglobulin, however, seems to be limited.23 The covariance between age and urinary cadmium in protein HC excretion (table 2) nevertheless suggests an increased vulnerability to cadmium in elderly people. Probably, normal degenerative changes of the renal tubuli in elderly people cause an increased sensitivity to cadmium.
Most studies of exposure to cadmium and renal tubular function have been performed on male workers. The present study showed only minor differences in tubular dysfunction between men and women, in accordance with a previous Japanese study of environmentally exposed people.24
All studies of exposure to cadmium and tubular dysfunction have been cross sectional. The tubular damage may have occurred a long time before the study was performed. If the concentration of urinary cadmium at the time of onset of tubular damage was higher, the dose-response curve would shift to the left in subsequent studies.17This problem, with a variable shape of the dose-response curve, is probably less relevant for environmentally exposed people, who have a continuous relatively low level of exposure compared with workers who have experienced high exposure to airborne cadmium in the past.17
It is, therefore, particularly noteworthy that tubular proteinuria occurs at relatively low concentrations of cadmium in urine and in the environmentally exposed group, in which the tubular damage appears at even lower concentrations than in the occupationally exposed group. It may well be that the occupationally exposed group comprises a selection of relatively healthy people, whereas the general population also includes more susceptible people. Furthermore, the group of environmentally exposed people also includes some who were very young when the exposure started and therefore are perhaps more susceptible to cadmium. In view of the relatively stable and low exposure to cadmium in the population examined, we think that the dose-response data presented here are valid and may be used to develop risk estimates in other environmentally exposed populations.
Research on health effects from cadmium has focused on the tubular damage, which from a health point of view may have limited importance, as the tubular proteinuria in itself does not give rise to any subjective symptoms or manifestations of disease.1 6 14It has recently been argued that the subclinical renal effects found in people with an increased cadmium body burden are not associated with progressive renal dysfunction, and that these early renal effects may even be reversible.25 It has been shown, however, that the cadmium induced tubular damage is irreversible in most cases even if exposure ends.7 Instead the tubular damage may become worse and glomerular damage with a drop in the GFR occurs. This has been seen among occupationally exposed workers as well as in people environmentally exposed to cadmium.7
Uraemia was common among Japanese farmers with itai-itai disease and end stage renal disease has been observed in workers heavily exposed to cadmium.3 An overall increased mortality among residents with cadmium induced tubular damage in areas of Japan polluted with cadmium has been reported, indicating that serious health consequences may eventually result from the tubular damage.3 7
Cadmium accumulation in the kidney is also related to negative health effects on the bone and mineral metabolism.1 3 7 An increased prevalence of kidney stones in workers exposed to cadmium has been noted by several investigators.7 Possibly this is related to the increased urinary excretion of calcium, secondary to tubular damage. A recent follow up of a large population of environmentally exposed people in Belgium suggests that cadmium accumulation increases the risk of development of osteoporosis.26 This is in agreement with the findings of the OSCAR study, in which we found age adjusted negative correlations between urinary cadmium, or urinary protein HC, and bone density.11a
In conclusion, the results from the present study indicate that renal tubular damage due to exposure to cadmium may develop at lower concentrations than previously anticipated. Even if the tubular dysfunction in itself is a benign condition, it is an indicator of a renal effect that eventually may lead to serious health consequences. Therefore, measures should be taken to reduce exposure to cadmium in the general population, including lowering of current standards for intake of cadmium in food.
Acknowledgments
The study was supported by a grant from the Swedish Environmental Protection Agency. Approval was obtained from the relevant research ethics committee. We thank Ann-Christin Palmqvist and Ann-Kristin Thunberg who collected the data and Mariette Blomberg for entering data into computer files.
References
Linked Articles
- Correction