Article Text

Abstract
Objectives This study investigated the effectiveness of the Stay@Work participatory ergonomics programme to reduce workers′ exposure to psychosocial and physical risk factors.
Methods 37 departments (n=3047 workers) from four Dutch companies participated in this cluster randomised controlled trial; 19 (n=1472 workers) were randomised to an intervention group (participatory ergonomics) and 18 (n=1575 workers) to a control group (no participatory ergonomics). During a 6 h meeting guided by an ergonomist, working groups devised ergonomic measures to reduce psychosocial and physical workload and implemented them within 3 months in their departments. Data on psychosocial and physical risk factors for low back pain and neck pain were collected at baseline and after 6 months. Psychosocial risk factors were measured using the Job Content Questionnaire and physical risk factors using the Dutch Musculoskeletal Questionnaire. Intervention effects were studied using multilevel analysis.
Results Intervention group workers significantly increased on decision latitude (0.29 points; 95% CI 0.07 to 0.52) and decision authority (0.16 points; 95% CI 0.04 to 0.28) compared to control workers. However, exposure to awkward trunk working postures significantly increased in the intervention group (OR 1.86; 95% CI 1.15 to 3.01) compared to the control group. No significant differences between the intervention and control group were found for the remaining risk factors. After 6 months, loss to follow-up was 35% in the intervention group and 29% in the control group.
Conclusion Participatory ergonomics was not effective in reducing exposure to psychosocial and physical risk factors for low back pain and neck pain among a large group of workers.
Trial registration ISRCTN27472278.
- Participatory ergonomics
- RCT
- risk factors
- back pain
- neck pain
- ergonomics
- musculoskeletal
- workload
Statistics from Altmetric.com
What this paper adds
Information obtained from randomised controlled trials on the effectiveness of participatory ergonomics to reduce workers' workload is scarce.
After 6 months, participatory ergonomics significantly improved the psychosocial risk factors decision latitude and decision authority but exposure to working in awkward postures was almost doubled among intervention group workers.
No significant intervention effects were found for the remaining psychosocial and physical risk factors.
Despite several statistically significant but not clinically relevant findings, participatory ergonomics was not effective in reducing exposure to psychosocial and physical risk factors for low back pain and neck pain among a large group of workers.
Introduction
Low back pain (LBP) and neck pain are important public health problems in industrialised nations.1 2 In the Netherlands, the 1-year prevalence of LBP is estimated to be 44% and is 28% for neck pain.3 These symptoms have serious consequences for the individual worker (ie, pain and disability) and for society and companies (ie, cost due to medical healthcare use, work absenteeism and loss of productivity).4 5 Prevention is, therefore, very important.
LBP and neck pain have multifactorial origins,6 indicating that various risk factors are associated with the development of LBP and neck pain among workers. Risk factors for LBP and neck pain are classified into individual risk factors (ie, gender, age and history of LBP and neck pain),6 7 psychosocial risk factors (ie, poor social support, job dissatisfaction, high job demands and low job control)8 and physical risk factors (ie, heavy manual lifting, awkward working posture of the trunk, whole body vibration and neck flexion).9–11
It has been postulated that exposures to psychosocial and physical risk factors for LBP and neck pain can be reduced in the workplace, for example by implementing ergonomic measures.12 Participatory ergonomics can be used to prioritise, devise and implement ergonomic measures in order to reduce workers′ exposure to risk factors. In a systematic review of various study designs, participatory ergonomics proved to be a promising approach to reduce psychosocial and physical workload.13 However, findings obtained from randomised controlled trials (RCT) are scarce. A recent cluster RCT on participatory ergonomics conducted among Finnish kitchen workers showed that participatory ergonomics did not result in significant reductions in either perceived physical workload or perceived psychosocial workload.14 15 Due to the lack of high quality evidence in this area, more evidence from RCTs is required.
Using a cluster randomised controlled study design, the Stay@Work study investigated the effectiveness of a participatory ergonomics programme compared to no participatory ergonomics (control group) in reducing exposure to work-related psychosocial and physical risk factors for LBP and neck pain after 6 months.
Methods
Details of the study design, methods and intervention described in the current study have been published elsewhere.16
Study population
All 5798 workers within the 37 participating departments were allowed to take part in the study. Because the primary outcome of the Stay@Work study was to prevent LBP and neck pain, only workers who met the following criteria at baseline were included in the analyses: (1) aged between 18 and 65 years; (2) not pregnant; and (3) with no cumulative sick leave period longer than 4 weeks due to LBP or neck pain in the past 3 months.
Sample size
Annual incidences of LBP and neck pain in a general working population of 12–14% and 6%, respectively, were used. Due to the episodic nature of LBP and neck pain, repeated measurements were conducted every 3 months. Based on the study of IJmker et al, an intra-class correlation coefficient (ICC) of 0.73 was estimated.17 By using this ICC, the power analysis revealed that a sample size of 1662 workers (two groups of 831 workers) was needed to detect a 25% reduction in LBP and neck pain prevalence among the intervention group compared to the control group.18 This difference can be detected with a power of 80% and α of 0.05. Taking into account a predicted dropout rate of 20% during the 12-month follow-up period, an initial study population of 2076 workers was needed.
Randomisation and blinding
An independent research assistant performed the randomisation by using a computer-generated randomisation programme. To avoid contamination of workers in the control group by those allocated to the intervention, randomisation was done at the level of department. Departments, each consisting of approximately 150 workers, from four Dutch companies (a railway transportation company, an airline company, a university including its university medical hospital, and a steel company) were pre-stratified according to their main workload: (1) mental, (2) mixed mental and physical, (3) light physical, or (4) physically demanding.19
Within each company, pairs of departments with comparable workloads were randomly selected and one department was allocated to the participatory ergonomics intervention group and the other to the control group (no participatory ergonomics). Subsequently, department managers were informed about the randomisation outcome.
The participatory ergonomics intervention made it impossible to blind researchers, ergonomists, working group members and department managers. However, workers in the departments were not aware of the study design, and were thereby blinded to the randomisation outcome.
Control
Before filling out the baseline questionnaire, all workers from the intervention and control departments were requested to watch three short (45 s) educational films showing LBP and neck pain risk factors (ie, lifting too heavy loads, frequent twisting of the lower back, and holding the neck in an awkward position) as well as the (ergonomic) solutions on how to avoid these situations. The films were used as a sham intervention and are an ineffective strategy to prevent LBP and neck pain.20
Intervention
All details of the intervention have been described thoroughly elsewhere.16 In short, directly after the randomisation outcome, each intervention department formed a working group consisting of eight workers and one department manager (or his/her representative). The intervention consisted of a 6 h working group meeting which was held between December 2007 and December 2008. Under the guidance of a trained ergonomist, the working group followed the steps of the Stay@Work participatory ergonomics programme. During the meeting working group members discussed a document which contained information on risk factors for LBP and neck pain in the department, which had been identified during a workplace visit by a ergonomist (which was mandatory for each intervention department), pictures made by the working group members, and baseline questionnaire information (step 1). The working group could also add other risk factors for LBP and neck pain and evaluated the risk factors on their frequency and severity. Based on the perceptions of the working group, the most frequent and severe risk factors were prioritised, resulting in three top risk factors (step 2). Subsequently, the working group held a brainstorming session about different types of ergonomic measures targeting the prioritised risk factors and evaluated the ergonomic measures according to an implementation criteria list including relative advantage, costs, compatibility, complexity, visibility and feasibility within a time frame of 3 months. Based on working group consensus, the three most appropriate ergonomic measures were prioritised (step 3). All prioritised risk factors and prioritised ergonomic measures were written down in an implementation plan (step 4). The implementation plan also described which working group member(s) was/were responsible for the implementation of the prioritised ergonomic measure(s); these people were called implementers. Implementers were requested to apply the prioritised ergonomic measures within 3 months in their department (step 5), and reductions in workload were expected shortly after implementation. If necessary, a second (1 h), optional meeting was arranged to evaluate or to adjust the implementation process (step 6).
To improve implementation, two or three implementers from each working group were asked to voluntarily follow a special 4 h implementation training programme to become a Stay@Work ergocoach. Forty implementers attended this training course, during which they were educated in different implementation strategies to inform, motivate and instruct their co-workers about ergonomic measures. They also received a toolkit consisting of flyers and posters to inform their co-workers about both the prioritised risk factors and the ergonomic measures.21
In total, the working groups prioritised 32 individual ergonomic measures (ie, improving awareness regarding ergonomics, worksite visits and physical activity programmes), 27 physical ergonomic measures (ie, ergonomic redesign or modification, new equipment and manual handling aids) and seven organisational ergonomic measures (ie, pause software installation, job rotation and restructuring management style). After the implementation period, the implementers received a short questionnaire assessing whether the prioritised ergonomic measures for which the implementer was responsible had been implemented in the department. This method enabled the investigators to calculate the percentage of perceived implementation. Approximately one third (34%) of the prioritised ergonomic measures were perceived as implemented in the intervention departments.21
Outcome measures and data collection
For practical reasons the baseline measurement took place after randomisation, and approximately 1 month before the start of the participatory ergonomics working group meetings. All workers within the randomised departments were invited to fill out the baseline questionnaire. Responders to the baseline questionnaire were sent the 6-month follow-up questionnaire.
Psychosocial risk factors
Data on exposure to psychosocial risk factors were assessed at baseline and after 6-month follow-up by means of a Dutch version of the Job Content Questionnaire (JCQ),22 which measures all dimensions of the demand–control–support model. Workers rated 25 items on a four-point scale (1=totally disagree, 2=disagree, 3=agree, 4=totally agree). By combining various items, the following dimensions were constructed: skill discretion, decision authority, psychosocial job demands, supervisor support and co-worker support. These dimensions have shown moderate to good reliability.23 The dimension decision latitude was constructed by combining the dimensions skill discretion and decision authority. The dimensions supervisor support and co-workers support were also combined into the dimension overall social support.
Physical risk factors
Data on exposure to physical risk factors were assessed at baseline and after 6-month follow-up by using the standardised Dutch Musculoskeletal Questionnaire (DMQ). By means of 63 items, the DMQ provides a brief overview of musculoskeletal workload and associated hazardous working conditions, which can be categorised into seven indices (forces, dynamic loads, static loads, repetitive loads, climatic factors, vibration and ergonomic environmental factors) and four separate factors (standing, walking, sitting and uncomfortable postures).24 Based on the literature,25–28 a total of 11 items (yes/no) that were considered to be associated with the onset of LBP or neck pain were selected from the DMQ (see table 1).
Baseline characteristics
Confounders
At baseline, data on various potential confounders were assessed.24 Gender, age and level of education were considered as potential confounders for both psychosocial and physical workloads, whereas work hours per week in current function was considered a potential confounder for physical workload only.
Statistical analyses
All analyses were performed according to the intention to treat principle. Baseline characteristics of workers in the two groups were compared using the unpaired Student t test (continuous variables) and Pearson's χ2 test (categorical and dichotomous variables).
Multilevel analysis was used to evaluate the intervention effects for all outcome variables. Multilevel analysis enables adjustment for the clustering of observations within matched randomisation pairs and departments. In this study four levels were identified: time (pre/post), workers, department and matched randomisation pairs. Almost 30% of the baseline responders did not respond to the follow-up questionnaire after 6 months. Under the assumption that data were missing at random,29 the method of maximum likelihood (ML) yields unbiased estimates. A nice feature of the ML procedure is that all gathered data on the outcomes can be used.
For each outcome variable, two analyses were performed: (1) a crude analysis (ie, the differences between the intervention and control group at 6-month follow-up adjusted for (minus) the corresponding baseline differences on the outcome variable), and (2) an adjusted analysis, encompassing an analysis as above but adjusted for potential confounders. For all analyses the intervention effect of interest was the interaction between group and measurement time.30 Adding potential confounders to the model did not change the intervention effect by more than 10%, and therefore, the results of the crude analysis are presented. All analyses were checked for effect modification by the main workload performed at the department. No significant interactions of p<0.05 were found with workload, indicating that effect modification did not occur. For this reason no stratified analyses on workload were performed.
Linear mixed models were used to evaluate the effects on psychosocial workload and logistic mixed models to evaluate the effects on physical workload. Logistic mixed models were not possible with all levels included, and the level ‘randomisation pairs’ was removed from the model. Intervention effects on four physical risk factors (lift and carry heavy loads, drive machines, and bend neck backwards) could not be determined. By deleting the level ‘department’ from the model, the analyses of these four risk factors were performed by including the ‘workers’ level only.
For all analyses a two-tailed significance level of p<0.05 was considered statistically significant. Linear mixed models were performed with SPSS v 15.0, and logistic mixed models with Stata v 10.0.
Results
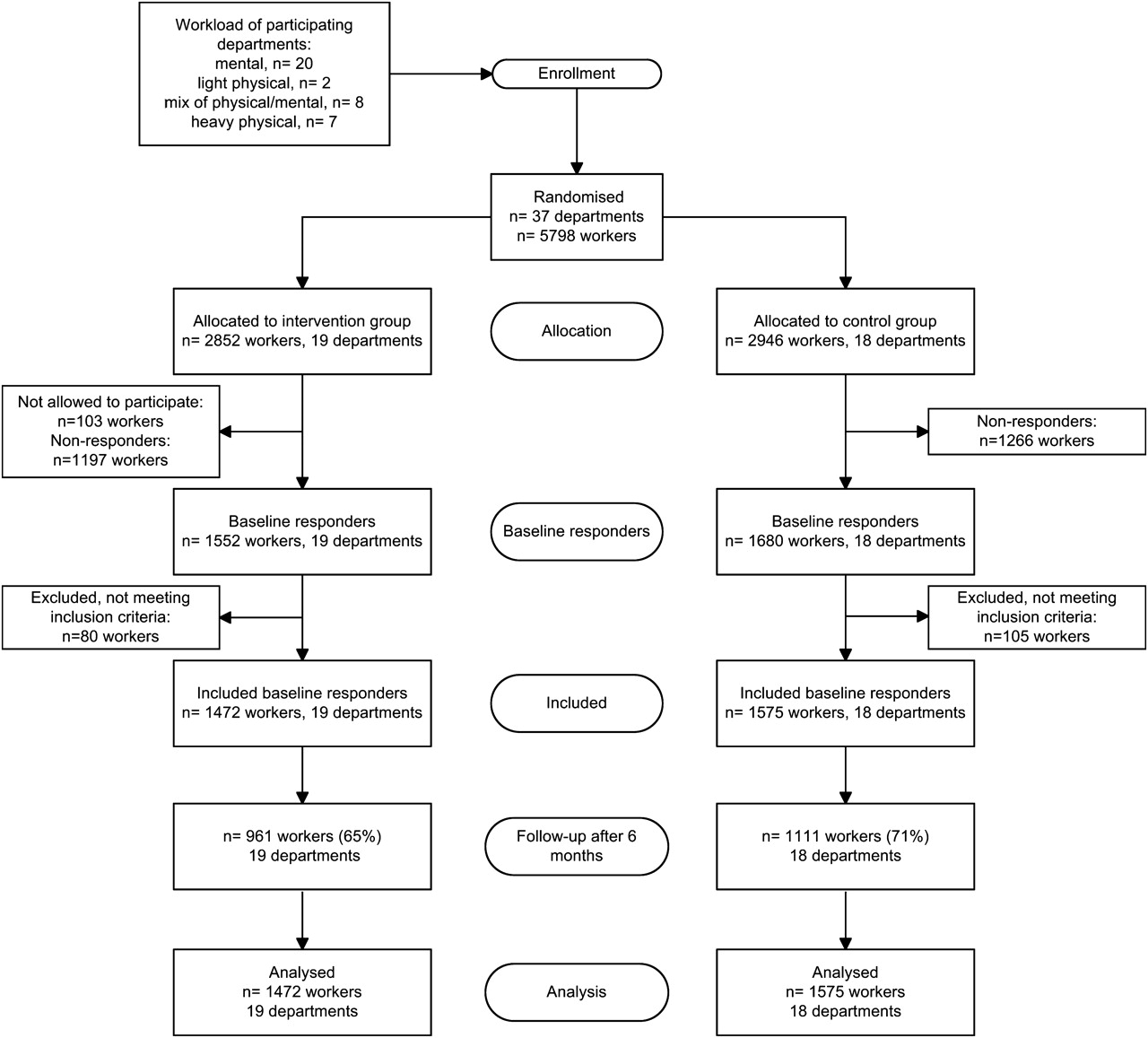
Figure 1 shows that 19 randomisation pairs were formed and the randomisation procedure allocated 19 departments to the intervention group and 18 departments to the control group. Most departments were characterised by a mental workload (n=10 in each group). Due to a sudden reorganisation, the manager of an intervention department consisting of 128 workers decided that a section of the department (n=103 workers) was not allowed to participate in the study or to receive the baseline questionnaire. Therefore, the baseline questionnaire was sent to 5695 workers, of whom 3232 (57%) responded. Among the 3232 baseline responders, 185 did not meet the inclusion criteria and were excluded from the analyses. Therefore, 3047 workers (n=1472 in the intervention group and n=1575 in the control group) met the inclusion criteria at baseline and were approached for follow-up measurements. The loss to follow-up after 6 months was 35% in the intervention group and 29% in the control group. Reasons for loss to follow-up were not collected systematically and, therefore, were largely unknown.

{kind=link}
Flow of departments and participants throughout the phases of the trial
Table 1 presents the baseline characteristics of workers in the intervention and control groups. Groups differed significantly on educational level and gender (57% men in the control group and 59% men in the intervention group). Regarding the outcome variables, various significant, but not clinically relevant differences were found between the intervention and control group.
Effects of the intervention on exposure to psychosocial risk factors
Table 2 shows the intervention effect on exposure to psychosocial risk factors after 6 months of follow-up. A statistically significant difference was found for the risk factors decision latitude (0.29 points; 95% CI 0.07 to 0.52) and decision authority (0.16 points; 95% CI 0.04 to 0.28), indicating that decision latitude and decision authority among workers in the intervention group improved significantly compared to workers in the control group. On all other psychosocial risk factors, except for supervisor support, the observed differences suggested that exposure to psychosocial risk factors among workers in the intervention group was slightly reduced. However, none of the differences were statistically significant.
Intervention effect* on exposure to psychosocial risk factors between the intervention group and control group after 6 months of follow-up
Effects of the intervention on exposure to physical risk factors
Table 3 presents the intervention effect on exposure to physical risk factors after 6 months of follow-up. A statistically significant different OR was found for the LBP risk factor awkward posture (OR 1.86; 95% CI 1.15 to 3.01), indicating that exposure to an awkward working posture of the trunk almost doubled among workers in the intervention group. With regard to the risk factor carry heavy loads, workers' exposure to this LBP risk factor was reduced among workers in the intervention group (OR 0.52; 95% CI 0.27 to 1.01). However, the difference was not significant (p=0.05). Although not statistically significant, the remaining physical risk factors tended to increase somewhat among workers in the intervention group.
Intervention effect* on exposure to physical risk factors between the intervention group and control group after 6 months of follow-up
Discussion
The results of this study showed that after 6 months the Stay@Work participatory ergonomics programme compared to no participatory ergonomics (the control group) resulted in statistically significant but small improvements in exposure to the psychosocial risk factors decision latitude and decision authority among workers in the intervention group. Because the dimension decision latitude was formed by combining the dimensions decision authority and skill discretion, it is possible that the increased decision latitude was the result of improvement found on decision authority. A statistically significant result was found on the physical risk factor for LBP awkward posture; surprisingly, exposure to an awkward working posture of the trunk almost doubled in the intervention group. Nevertheless, the sizes of the intervention effects were small and can be considered as not clinically relevant.31 No statistically significant differences were found for the remaining psychosocial and physical risk factors.
There are several possible explanations why our trial generally failed to demonstrate that the participatory ergonomics programme was effective. The process evaluation of this study showed that 6 months after the participatory ergonomics meeting, the implementers perceived approximately one third of the 66 prioritised ergonomic measures as implemented, while 26% of the workers in the intervention departments perceived the prioritised ergonomic measures as implemented.21 The implementation rate was probably too low to successfully reduce exposure to risk factors among workers. We found that implementation of the prioritised ergonomic measures was hampered by factors such as a shortage of financial/personnel resources, lack of time to implement ergonomic changes and insufficient stakeholder involvement.32
High implementation rates in participatory ergonomics programmes are, however, no guarantee of risk factor reduction. For example, the study by Haukka et al reported that almost 80% of prioritised ergonomic measures were implemented but found no significant reductions in workload.14 15 In this context, the efficacy (can an ergonomic measure change the outcome?) of the prioritised ergonomic measures can be questioned. For example, in our study 32 of the 66 prioritised ergonomic measures consisted of individual ergonomic measures (ie, improving awareness regarding ergonomics using brochures, worksite visits and physical activity programmes),21 whereas such measures may not be able to reduce workers′ psychosocial and physical workloads.33
Another explanation may be the general lack of exposure to psychosocial and physical risk factors between the two trial arms. At the start of this study, the mean sum scores of the JCQ dimensions and the prevalence rates of physical risk factors in both groups were low, indicating that workers perceived low levels of psychosocial and physical workloads. Consequently, the effects of the participatory ergonomics programme on the reduction in risk factor exposure may be masked because little room was left for improvements. It is not thought that confounding played a role in this study because adding the most important potential confounders (age, gender, education and work hours per week) to the mixed models did not change the intervention effects of the crude models by more than 10%. It is therefore unlikely that variables such as lifestyle factors (eg, smoking, alcohol consumption and obesity/overweight) would have led to different results.
In this study, workers′ exposure to the risk factors was assessed using self-reports. Self-reports are commonly used for physical workload but may result in imprecise estimates of workers′ tasks and activities.34 Direct measurements (ie, EMG) on each individual worker may have been more precise and accurate for measuring exposure to posture, movement and exerted forces in order to present valid estimates of physical workload.35 However, practical aspects meant direct measurements on every individual worker were not feasible. Furthermore, this study focused on a selection of 11 physical risk factors, whereas other possible physical risk factors (ie, repetitive movements, maximal force extensions and lifting loads above chest height) or risk factors outside the workplace were not taken into account. Assessing the psychosocial workload was only possible by using self-reports and so the valid and reliable JCQ was used. Moreover, instead of using repeated measurements, this study used one follow-up moment, which may have not been sufficient to detect changes in workers′ exposure.
In addition to the use of self-reports and lack of exposure, another limitation of this study was the loss to follow-up after 6 months, which was considerable (>20%).36 Non-responders were younger (mean 40.7 years, SD 11.3) compared to responders, and were predominantly men performing heavy physical work. However, we do not believe that this has influenced our study results, because the non-responders′ characteristics did not significantly differ between the intervention and control group. Moreover, during all analyses the well-recognised ML procedure was applied to take into account the incompleteness in the data.29 However, there are several distinctive features to our work. This cluster RCT is the first study to investigate the effectiveness of participatory ergonomics in reducing workers′ exposure to psychosocial and physical workload in such a large working population with various task groups. Therefore, the generalisability of the results obtained from this study is high. Furthermore, workers were kept blind to the study design and the randomisation outcome, and so the possibility that workers would undertake actions that could interfere with the experimental design was minimised. By performing the randomisation procedure at departmental level, contamination between workers in the intervention and control group was prevented. Co-interventions can be present in pragmatic trials, but we do not believe that co-interventions have threatened the validity of our study results. During the follow-up period, the number of ergonomic measures implemented in the intervention and control departments beyond the participatory ergonomics programme were equally distributed between the two groups (intervention group n=442 and control group n=483). Moreover, no departmental reorganisations occurred during follow-up.
Comparison with other studies
Our findings most often contradict the conclusion drawn in the review of Rivilis et al. However, making comparisons with this review is hard. The authors concluded that participatory ergonomics was effective for reducing workers′ exposure to both psychosocial and physical risk factors,13 but did not specifically mention the exact risk factors for which participatory ergonomics was effective. Comparing our results with some of the individual studies included in the Rivilis review was difficult, because the included studies differed largely from our study regarding study design (controlled trial, before–after study), study populations (ie, cleaners, hospital orderlies, industry workers), the content of the participatory ergonomics intervention (ie, working group not allowed to make decisions), outcome assessments and follow-up duration. The results of more recently conducted studies on participatory ergonomics (which were not included in the systematic review by Rivilis and colleagues) were more in line with our findings. For example, the studies of Laing et al showed that participatory ergonomics led to statistically significant reductions in mechanical exposures among automotive industry workers,37 but did not lead to statistically significant reductions in psychosocial workload.38 Despite an implementation rate of 80% (n=402 ergonomic measures), the findings of a large cluster RCT among Finnish kitchen workers concluded that participatory ergonomics was not more effective in reducing physical and psychosocial workload than no participatory ergonomics in the control group.14 15 Next to the efficacy of prioritised ergonomic measures, compliance with the measures is also important in order to reduce workers′ exposure to occupational risk factors. The use of implementation strategies to inform workers about the health risks and advantages of ergonomic measures, educate workers how to use the ergonomic measures and reduce workers′ barriers to using the ergonomic measures can improve compliance, and thereby improve the effectiveness of ergonomic measures.39 The current study made a first attempt by introducing the Stay@Work ergocoach as implementation strategy, and provided special training to 40 implementers to become ergocoaches.21 Probably because of the low implementation rate of the prioritised ergonomic measures, the ergocoaches played a less effective role than expected. However, Jensen and Friche showed that a participatory ergonomics programme in combination with an implementation strategy (ie, information about ergonomics and training in ergonomic skills) resulted in sustainable reductions in severe knee problems among Danish floor layers.40 Based on the findings of our process evaluation in which participatory ergonomics appeared to be a successful method to prioritise risk factors and develop and prioritise ergonomic measures,21 and the promising findings of Jensen and Friche, we still believe that participatory ergonomics has the potential to reduce workers′ exposure to occupational risk factors. Therefore, researchers on future participatory ergonomics studies are not only encouraged to improve the implementation of ergonomic measures, but are also challenged to develop and incorporate adequate and intensive implementation strategies (ie, use of informative materials, training in ergonomic skills, education of workers, and ergocoaches) into their participatory ergonomics programmes.
Conclusions
The results of this cluster RCT showed that after 6 months, exposure to the psychosocial risk factors decision latitude and decision authority significantly improved among workers in the intervention group. However, after 6 months workers in the intervention group were significantly more exposed to an awkward working posture of the trunk. Nevertheless, the effect sizes were small and were considered not clinically relevant. For the remaining psychosocial and physical risk factors for LBP and neck pain, we could not detect a significant effect. The results should be interpreted with care as the implementation rate of the prioritised ergonomic measures was low. It is recommended that future participatory ergonomics research projects targeted at reducing workers′ exposure to the psychosocial and physical risk factors for LBP and neck pain use participatory ergonomics programmes in combination with effective implementation strategies.
References
Footnotes
Funding This study was funded by The Netherlands Organisation for Health Research and Development (ZonMw).
Competing interests None.
Ethics approval This study was conducted with the approval of the Medical Ethics Committee of the VU University Medical Center.
Provenance and peer review Not commissioned; externally peer reviewed.