Article Text

Abstract
Objectives To investigate whether prior symptoms of allergic disease influence first job undertaken on leaving school.
Methods The study included 5020 members of the 1958 British birth cohort who provided a job history (including start dates) at age 33 and for whom information on allergic disease in childhood and adolescence was reported by parents at ages 7, 11 and 16. Occupational group (high risk, low risk, reference) was based on first job and its probable asthma risk.
Results With occupational group defined using only job title, the RR of taking a high risk over a reference level job was an estimated 30% (RR ratio (RRR) 0.70; 95% CI 0.56 to 0.88) lower among those with than without prior reported symptoms of hay fever/allergic rhinitis but an estimated 60% (RRR 1.60; 1.17 to 2.19) higher among those with symptoms of asthma/wheezy bronchitis in adolescence compared to those with no history of asthma/wheezy bronchitis. With occupational group defined using an asthma specific job exposure matrix, a similar association was observed for prior hay fever/allergic rhinitis (RRR 0.77; 0.62 to 0.96) but not for asthma/wheezy bronchitis (RRR 1.18; 0.85 to 1.64). There was no evidence of an association between prior eczema and occupational group of first job.
Conclusion Whether our findings indicate avoidance or residual confounding, it would be prudent for future studies of occupation and the incidence or recurrence of asthma in adult life to adjust for any previous history of hay fever/allergic rhinitis.
- Asthma
- hay fever
- occupation
- allergy
- asthma
Statistics from Altmetric.com
What this paper adds
Estimates of associations of occupation with adult onset asthma will be biased if those with hay fever in childhood and/or adolescence (a risk factor for the development of asthma) avoid particular jobs on entering the work force in an effort to minimise their exposure to certain allergens.
Among a British cohort born in 1958, a history of hay fever/allergic rhinitis between 0 and 16 years of age appeared to be associated with a lower probability of entering an occupation classed as high risk for asthma.
It would be prudent for future studies of occupation and asthma to adjust for any previous history of hay fever and/or allergic rhinitis.
Introduction
The burden of occupational asthma is felt not only by the individual but also by employers and tax payers in terms of its drain on healthcare services and the number of working days lost due to ill health.1 2 The estimated proportion of adult onset asthma associated with occupational exposure varies between studies, ranging from as low as 2% to as high as 21%.3 The validity of such figures relies on estimates of the association between occupational exposures and adult onset asthma arising from population- and workplace-based studies. These associations are argued to be consistently under-estimated.3–5
One difficulty in assessing occupational risk is that many studies have inadequate information on age at onset of disease.4 5 This to a large extent can be overcome in longitudinal studies that collect information on disease occurrence throughout life. Another difficulty is that those with symptoms of asthma or other allergic disease may avoid certain jobs.4 6 One possible reason for inaccurate results in cross-sectional studies is that people with asthma are avoiding occupations through job selection. Bias results due to there being (1) fewer people with asthma in high risk occupations and (2) more people with asthma in the reference category.4 6 Allergic diseases such as eczema, hay fever and allergic rhinitis are associated with the development of asthma, so if people with allergic disease are avoiding high risk occupations and entering low risk/reference jobs, there will appear to be a reduced risk in high risk occupations. This form of ‘healthy worker hire effect’ was highlighted in a paper by Le Moual et al,4 who suggested that studies based on child to adult cohorts may provide important information on the magnitude of this potential bias.
Using data from such a birth cohort study, the National Child Development Study (NCDS), we aim to investigate whether individuals with asthma or allergic disease before entry to the workforce are more or less likely to be employed in jobs considered to be at high risk for the development of asthma.
Methods
Study population
This study is based on a cohort of 18 558 British children born in 1 week in 1958, including immigrants with the same birthday who entered the country before age 17 years. The cohort was followed up at intervals including at ages 7, 11, 16, 23 and 33 years.7–9 Response rates although declining over successive follow-ups, have remained relatively high and at age 33, the target sample was 16 229 of whom 11 468 (71%) participated.10 11 Nevertheless, cohort data collected in adult life are known to under-represent Britain's non-white ethnic groups. In addition, previous comparisons between those interviewed and those targeted at age 33 have identified small biases in response in favour of females and more privileged individuals (eg, those from middle class backgrounds),10 11 and modelling of non-response by Hawkes and Plewis found that responders at age 33 tended to have a more stable employment history recorded at the 23-year follow-up.12
Information on prior allergic disease
At age 7, a doctor noted the presence or absence of eczema and parents were asked if the study child had a history of ‘eczema in the first year’, a history of ‘eczema after the first year’, ever had ‘hay fever or sneezing attacks’, ever had ‘attacks of asthma’ and ever had ‘bronchitis with wheezing’.
At age 11, parents were asked if the study child had ever had ‘attacks of asthma, or asthma and wheezy bronchitis, or wheezy bronchitis only’, ‘hay fever or allergic rhinitis in the past 12 months’ and ‘eczematous rashes in the past 12 months’.
At age 16 they were asked if the study child had ‘ever had an attack of asthma or wheezy bronchitis’ and if yes, when the most recent attack occurred, suffered from ‘hay fever or allergic rhinitis in the past 12 months’ and suffered from ‘eczematous rashes in the past 12 months’.7
Using the above, we constructed three variables representing prior allergic disease: hay fever/allergic rhinitis ages 0–16 (coded yes or no); eczema ages 0–16 (coded yes or no); and asthma/wheezy bronchitis ages 0–16 coded ‘symptoms in adolescence’ (ie, most recent attack at ages 11–16 years according to parental report at the 16-year follow-up), ‘symptoms only in childhood’ (ie, asthma/wheezy bronchitis ever, reported at ages 7 and/or 11 but no report at the 16-year follow-up of any attacks since 11th birthday) or ‘no’ (ie, no reported history at ages 7, 11 or 16).
Confounding factors and job history
Information on father's social class was collected at birth and supplemented where missing with information on father's social class as reported at the 7-year follow-up.7 The date of leaving school was reported by the cohort member themselves at age 23 years.8 At age 33, cohort members were asked to provide a complete job history, including up to 12 jobs (each lasting 1 month or more) since leaving school and up to 12 periods (each lasting 1 month or more) when out of a job (eg, when ‘unemployed and seeking work’, in ‘full-time education’, in ‘government training or work scheme’, ‘full-time housework or childcare’ or ‘unable to do work because of sickness or handicap’).9
Coding based on job title
A job history including starting dates was provided by 10 185 cohort members at age 33, of whom 10 131 had a record of at least one job (figure 1). Jobs were coded according to the Standard Classification of Occupations 1990 and then re-coded, blind to asthma status, according to the International Standard Classification of Occupations 1988 (ISCO88). ISCO88 codes were then mapped onto 27 job titles, and based on a categorisation used by the European Community Respiratory Health Survey of adult onset asthma,13 the first job recorded for each individual (i.e. the job with the earliest starting date, or in the case of a tie, the job mentioned first in the questionnaire) was placed in one of three occupational groups: (1) a reference group of mainly professional, clerical and administrative jobs; (2) a high risk group including cleaners, caretakers, hairdressers, barbers, beauticians, nurses, agriculture and forestry workers, bakery workers, plastics and rubber workers, chemical processors, welders and flame cutters, workers involved in metal making and metal treating, other metal workers, electrical processors, painters, spray painters and printing workers; and (3) an ‘other occupations’ or ‘low risk’ group including all job titles not otherwise assigned.
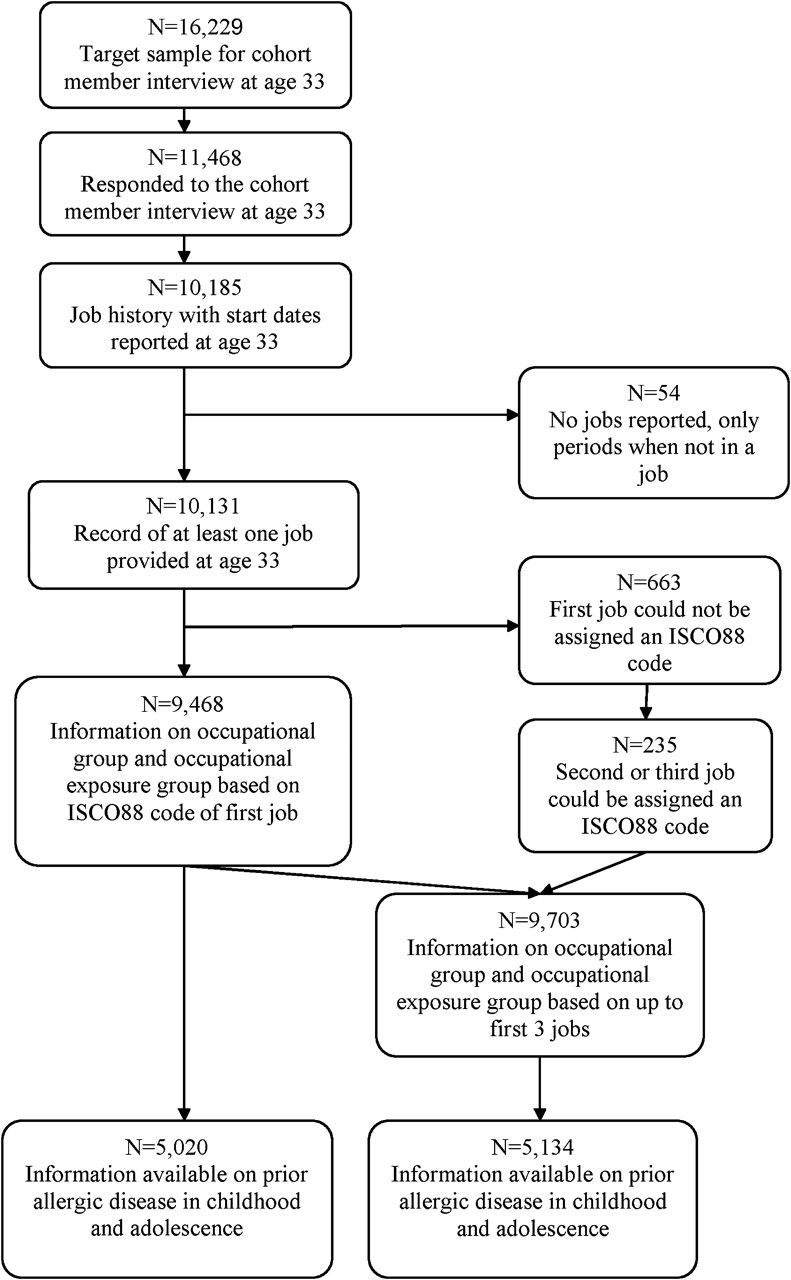
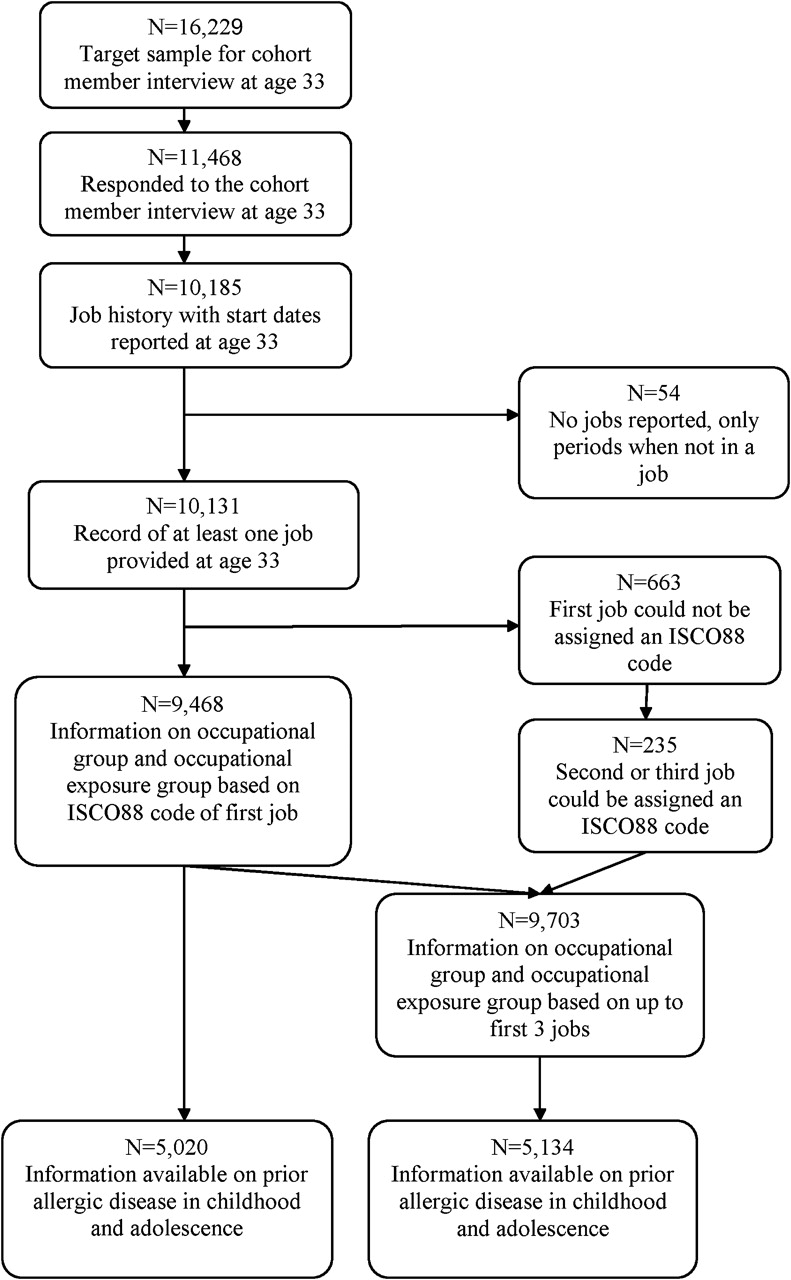{kind=link}
Diagram illustrating response and sample attrition.11
Coding based on the job exposure matrix
Another occupational variable, ‘occupational exposure group’, was constructed by linking ISCO88 codes to 22 potential occupational exposures using an asthma specific job exposure matrix (ASJEM) with the inclusion of an expert judgement step.14 Consistent with the categorisation used in a report on job choices in German teenagers,15 and using information from the ASJEM, we allocated first jobs into three occupational exposure groups14: (1) a reference group of unexposed jobs; (2) a high risk group of jobs associated with exposure to high or low molecular weight agents, mixed environments or peak exposures; and (3) a low risk group of jobs not otherwise assigned.
Occupational variables based on first three jobs
As the first job for some individuals may represent a period of short term employment rather than a career choice and to increase statistical power, two further occupational variables, one based on job title (ie, occupational group) and the other on the ASJEM (ie, occupational exposure group), were similarly defined using information on the first three jobs reported. If all jobs up to a maximum of the first three were reference level, the cohort member was assigned to the reference group and if any of the first three was high risk, the subject was assigned to the high risk group. For all other job combinations, the subject was allocated to the low risk group.
Data source
The NCDS data were provided in anonymised form by the UK Data Archive.
Statistical methods
In preliminary analysis variables were cross-tabulated and simple χ2 tests used to detect associations.
Treating occupational category (reference, low risk, high risk) as the outcome variable to be predicted by health status in childhood and adolescence, associations were further investigated using multinomial logistic regression as implemented by MLOGIT in Stata 10.16 Essentially this simultaneously models (1) the RR of taking a high asthma risk job over a reference level job (primary contrast) and (2) the RR of taking a low asthma risk job relative to a reference level job, and their respective associations with prior allergic disease. Results are presented as relative risk ratios (RRR) and their 95% CIs both before and after adjustment for potential confounding factors including sex, region of residence at age 16 (11 regions), father's social class at birth, school leaving age, whether continued full-time education on leaving school and other prior allergic disease. An RRR is the ratio of two relative risks, for example the probability (risk) of taking a high risk job over the probability of taking a reference level job among those with prior hay fever, divided by the probability of taking a high risk job over the probability of taking a reference level job among those without prior hay fever.17 For a dichotomous outcome variable, RRRs are the same as ORs but even where the outcome variable has multiple categories (as here—reference, low risk, high risk) RRRs are sometimes treated as if they were ORs for ease of interpretation.
Asthma/wheezy bronchitis at ages 0–16 was treated as a three level factor for adjustment but as a continuous variable taking the values 0, 1 and 2 for significance testing. All other variables were entered into models as categories (table 1). Statistical significance was based on detecting differences across all three occupational or occupational exposure groups (reference, low risk, high risk) and was assessed using the likelihood ratio test.
Potential predictors of job choice based on title of first job (N=5020)
Results
Occupational group and occupational exposure group of first job were successfully calculated for 9468 subjects, of whom 5020 also had complete information on prior allergic disease (figure 1).
Sample attrition
According to the occupational group of the earliest job recorded in the job history, 58.6% of subjects were assigned to the reference group, 20.8% to the other/low risk group and 20.7% to the high risk group. For occupational exposure group, the corresponding percentages were 52.1%, 28.3% and 19.6%, respectively. The median age at first job was 16 years (IQR 16–18) and the median length of first job was 2.41 years (IQR 0.83–5.92; n=9345).
When the data set was restricted to those with information on prior allergic disease, percentages were little changed. For occupational group, they were 60.1% (reference), 19.3% (other/low risk) and 20.6% (high risk) and for occupational exposure group, 53.6%, 27.3% and 19.1%, respectively. Median age at first job was 16 years (IQR 16–18) and median length of first job was 2.58 years (IQR 0.83–6.00; n=4961).
Occupational group based on job title of first job
From table 1, the percentage whose first job was classed as high risk for asthma was higher in men than in women (29.4% vs 12.5%), in those born into a manual rather than a non-manual social class background (22.1% vs 16.9%), in those who left school before age 17 years rather than at or after age 17 (25.1% vs 10.5%) and in those who did not rather than did continue full time education on leaving school (22.3% vs 8.2%). Occupational group of first job also differed significantly by region (p<0.001, df=20) with the percentage entering a high risk occupation being lowest among those living in the South East of England at age 16 years (16.1%) and highest among those living in the Midlands of England (24.5%).
For prior allergic disease, the percentage in the high risk group was slightly higher among those with than without a report of asthma/wheezy bronchitis in childhood or adolescence (22.8% vs 19.9%) but lower among those with than without a parental report of hay fever/allergic rhinitis at ages 7, 11 or 16 years (16.7% vs 21.4%). There was no evidence of an association between prior eczema and occupational group.
When we used multinomial regression to adjust for sex, father's social class at birth, region, school leaving age and whether continued full-time education on leaving school (adjustment 2, table 2), overall associations of occupational group with hay fever/allergic rhinitis and with prior asthma/wheezy bronchitis fell short of statistical significance at the 5% level.
Ratios of relative risks (RRR) and their 95% CIs investigating the association between prior symptoms of allergic disease and job choice based on title of first job (N=5020)
However, in our final model we additionally adjusted for other allergic disease (adjustment 3, table 2). Based on this analysis, the RR of entering a high risk job over a reference level job was estimated as 60% higher (RRR 1.60; 95% CI 1.17 to 2.19) among those with symptoms of asthma/wheezy bronchitis in adolescence than among those with no prior symptoms of asthma/wheezy bronchitis, while for hay fever/allergic rhinitis the RR was an estimated 30% lower (RRR 0.70; 0.56 to 0.88) among those with than without prior symptoms. However, there was no clear trend in RR across the three asthma categories (no, symptoms only in childhood, symptoms in adolescence) and only for hay fever/allergic rhinitis did the overall association with occupational group regain statistical significance at the 5% level.
Sensitivity analyses
Of the 5020 subjects in the analysis, 352 (7.0%) started their first job before the interview at age 16 years and for a further 12 (0.2%) the date of the 16-year interview was not recorded. In theory, this group could have developed asthma in the first months of their first job before they were interviewed at age 16. When we repeated the analysis (adjustment 3) excluding these 364 subjects, the RR of taking a high risk job over a reference level job was 61% higher (RRR 1.61; 1.16 to 2.23) among those with symptoms of asthma/wheezy bronchitis in adolescence than among those with no prior symptoms of asthma/wheezy bronchitis and 31% lower (RRR 0.69; 0.55 to 0.87) among those with than without prior symptoms of hay fever/allergic rhinitis.
Occupational exposure group based on ASJEM applied to first job
A similar association (compare tables 1 and 3) with father's social class was observed for occupational exposure group of first job as for occupational group. In contrast, using occupational exposure group, differences in the percentage categorised as high risk were less marked between males and females (21.1% vs 17.3%), those who left school before age 17 years rather than at or after age 17 (21.3% vs 15.3%) and those who did not rather than did continue full time education on leaving school (19.9% vs 13.4%). Occupational exposure group also differed significantly by region (p<0.001, df=20), with the percentage categorised as high risk still lowest among those living in the South East of England at age 16 years (15.1%), although highest among those living in the North West (23.1%).
Potential predictors of job choice based on first job and using an asthma specific job exposure matrix (N=5020)
As in the previous analyses (compare tables 2 and 4), there was no evidence that eczema was associated with entering a high risk job, and even though the overall association between occupational exposure group and prior hay fever/allergic rhinitis fell short of statistical significance at the 5% level (adjustment 3, table 4), a similar RR ratio for entering a high risk over a reference level job was observed (RRR 0.77; 0.62 to 0.96). There was no evidence of an association with asthma/wheezy bronchitis.
Ratios of relative risks (RRR) and their 95% CIs investigating the association between prior symptoms of allergic disease and job choice based on first job using an asthma specific job exposure matrix (N=5020)
Additional analyses based on up to first three jobs
When based on up to the first three jobs and after adjustment (see table 5 in the online data supplement), prior hay fever/allergic rhinitis was significantly associated with both occupational group and occupational exposure group. The RR of taking a high risk job over a reference level job was estimated as 30% lower (RRR 0.70; 0.57 to 0.84) among those with than without prior hay fever/allergic rhinitis when using occupational groups and 27% lower (RRR 0.73; 0.60 to 0.88) when using occupational exposure groups.
Occupational group was significantly associated with prior symptoms of asthma/wheezy bronchitis, with the RR of taking a high risk job over a reference level job estimated as 58% higher (RRR 1.58; 1.18 to 2.13) among those with symptoms of asthma/wheezy bronchitis in adolescence than among those with no prior symptoms of asthma/wheezy bronchitis. There was no evidence of an association of occupational exposure group with prior asthma/wheezy bronchitis but some evidence of an association with prior eczema.
Discussion
Among a British cohort born in 1958, a history of hay fever/allergic rhinitis in childhood or adolescence appeared to be associated with a lower probability of entering a job with high asthma risk. This observation was consistent when a high risk job was defined by job title or by a job exposure matrix (ASJEM), and was robust to adjustment for other allergic disease.
The association of asthma with first job choice was less clear, and differed with definition of high risk jobs. Our data provide no evidence that adolescents with asthma or wheezy bronchitis are avoiding high risk jobs and when the definition of high risk was based on job title rather than the ASJEM, symptoms at ages 11–16 years appeared to be associated with a higher probability of entering a high risk job.
While job titles are simple to use for exposure assignment, they are imprecise by comparison with job exposure matrices or other such methods in which more detail (eg, from the job or task description) is used to ascribe risk.5 14 In addition, our use of the ASJEM included an expert judgement step from British occupational experts and the combination of these factors might explain the differing results for asthma.
Our unexpected findings for asthma/wheezy bronchitis may have been influenced by early occupational exposure, although this conjecture was not supported by our sensitivity analysis in which we excluded subjects whose first job started before the 16-year interview or for whom the interview date was missing. However, with such a diverse range of jobs in our high risk groups and the inclusion of wheezy bronchitis in our definition of disease, the avoidance of certain occupations or exposures by those with asthma entering the job market for the first time cannot be discounted.
Choice of reference groups may also have affected results. As in other epidemiological studies,15 18 the groups used were made up solely or primarily of professional, clerical and administrative jobs. Thus, observed patterns may have been influenced by lack of job choice among those whose disease may have compromised their level of achievement at school,15 and confounding by social class, especially as in the study sample (n=5020), the proportions with reported hay fever/allergic rhinitis at ages 0–16 and asthma/wheezy bronchitis at ages 11–16 were higher among cohort members born into a non-manual than manual social class background (data not shown). In our analysis we therefore adjusted for father's social class at birth, age at leaving school and whether continued full-time education on leaving school. Further, when we additionally adjusted for father's social class at age 11 and self-reported smoking at age 16 (data not shown), those RRR comparing high risk to reference level jobs for hay fever/allergic rhinitis, eczema and asthma/wheezy bronchitis, were little changed.
Our findings support work from other parts of Europe. Radon et al15 studied German teenagers in vocational training who were asked to specify the type of job they would like in the future. Among those with allergic rhinitis, a lower proportion selected jobs associated with a high asthma risk. In addition, a large study of Swedish conscripts found strong evidence to suggest that those with allergic rhinitis in adolescence were less likely to take up jobs with a high probability of airway-irritating exposure.19 These studies also commented on the apparent lack of job avoidance observed among those with prior asthma compared to those with prior allergic rhinitis.15 19
Why allergic rhinitis rather than asthma should be associated with a lower probability of entering a high risk job is unclear. It may reflect the relative side effects of treatments (eg, sedating antihistamines used in the treatment of allergic rhinitis)20 or the likelihood of being symptomatic at the time of looking for that first job (eg, in the summer months after leaving school).
Nevertheless, a history of hay fever is a strong risk factor for asthma incidence in adults.21 If, as our findings suggest, such high risk individuals are more prevalent in occupations with particularly low exposures, reference groups used in studies of asthma and occupation will tend to contain an excess number of cases. Without adjustment for prior hay fever/allergic rhinitis, such studies may therefore under-estimate the proportion of adult onset asthma attributable to occupation.
Conclusion
Whether our findings for hay fever/allergic rhinitis indicate avoidance, selection by employers4 or residual confounding, it would be prudent for future studies of occupation and the incidence or recurrence of asthma in adult life to adjust for any previous history of hay fever and/or allergic rhinitis.
Acknowledgments
The experts who helped in the evaluation of the asthma specific job exposure matrix were Dr David Fishwick (Centre for Workplace Health, Sheffield), Dr Jennifer Hoyle (North Manchester General Hospital) and Dr Chris Warburton (Aintree Chest Centre, University Hospital Aintree, Liverpool). We also wish to acknowledge the original creators, sponsors, depositors and distributors of the NCDS data. Sweeps 0–3, 1958–1974 were created by the National Birthday Trust Fund and the National Children's Bureau, and sponsored by the Economic and Social Research Council, the National Birthday Trust Fund, the Institute of Child Health (University College London), the National Foundation for Educational Research and the Department of Health. Sweep 4, 1981 and Public Examination Results, 1978 were created by the National Children's Bureau, and sponsored by the Department of Health and Social Security, the Department of Education and Science, the Department of Employment, the Department of the Environment and the Manpower Services Commission. Sweep 5, 1991 was created by the Social Statistics Research Unit, City University, and sponsored by the Economic and Social Research Council, the Department of Health, the Department of Social Security, the Department of Employment, the Department of Education and Science, the Department of the Environment, the Transport and Road Research Laboratory, the Health and Safety Executive and the National Institute for Child Health and Development, United States of America. The principal investigator (depositor and copyright holder) for all three Data Collections is the Centre for Longitudinal Studies, Institute of Education, University of London. The Data Collections (2nd edition, 2008) were distributed by the UK Data Archive, University of Essex, Colchester. The original data creators, depositors or copyright holders, the funders of the Data Collections and the UK Data Archive bear no responsibility for their further analysis or interpretation.
References
Supplementary materials
Web Only Data oem.2010.058065
Files in this Data Supplement:
Web Only Data oem.2010.058065
Files in this Data Supplement:
Footnotes
Funding Asthma UK (project ID 07/32) provided funding for this study.
Competing interests None.
Provenance and peer review Not commissioned; externally peer reviewed.