Article Text

Abstract
Background Occupational risks for bladder cancer in hairdressers by using hair products have been examined in many epidemiological studies. But owing to small sample sizes of the studies and the resulting lack of statistical power, the results of these studies have been inconsistent and significant associations have rarely been found.
Methods We conducted a meta-analysis to determine summary risk ratios (SRRs) for the risk of bladder cancer among hairdressers. Studies were identified by a MEDLINE, EMBASE, CENTRAL search and by the reference lists of articles/relevant reviews. Statistical tests for publication bias and for heterogeneity as well as sensitivity analysis were applied. In addition, the study quality and the risk of bias were assessed using six criteria.
Results 42 studies were included and statistically significantly increased risks around 1.3–1.7 were found for all but one analysis. The SRR increased with duration of employment from 1.30 (95% CI 1.15 to 1.48) for ‘ever registered as hairdresser’ to 1.70 (95% CI 1.01 to 2.88) for ‘job held ≥10 years’. No difference was found between the risk for smoking-adjusted data (SRR 1.35, 95% CI 1.13 to 1.61) and no adjustment (SRR 1.33, 95% CI 1.18 to 1.50). Studies assessed as being of high quality (n=11) and of moderate quality (n=31) showed similar SRRs. There was no evidence of publication bias or heterogeneity in all analyses.
Conclusion In summary, our results showed an increased and statistically significant risk for bladder cancer among hairdressers, in particular for hairdressers in jobs held ≥10 years. Residual confounding by smoking cannot be totally ruled out. Because of the long latency times of bladder cancer it remains an open question whether hairdressers working prior to 1980 and after 1980, when some aromatic amines were banned as hair dye ingredients, have the same risk for bladder cancer.
- Urinary bladder neoplasms [MeSH]
- occupational exposure
- hairdresser
- hair dyes
- aromatic amines
- epidemiology
- occupational health practice
- public health
- cancer
- urological
This is an open-access article distributed under the terms of the Creative Commons Attribution Non-commercial License, which permits use, distribution, and reproduction in any medium, provided the original work is properly cited, the use is non commercial and is otherwise in compliance with the license. See: http://creativecommons.org/licenses/by-nc/2.0/ and http://creativecommons.org/licenses/by-nc/2.0/legalcode.
Statistics from Altmetric.com
- Urinary bladder neoplasms [MeSH]
- occupational exposure
- hairdresser
- hair dyes
- aromatic amines
- epidemiology
- occupational health practice
- public health
- cancer
- urological
Introduction
Until the end of the 1970s several aromatic amines (eg, 4-aminobiphenyl, benzidine, 2-naphthylamin, 4-chloro-o-toluidine) were used in hair dyes and other hair products, which were identified as carcinogenic for urothelial cancers.1 2 In response, regulatory action was taken in 1978 and some aromatic amines were banned as hair dye ingredients in the European Union, but other aromatic amines have still been used in hair dyes. Therefore today, there seems to be no relevant bladder cancer risk from the use of hair dyes. But human urothelial cancers, chemically induced by aromatic amines, typically have latency times often longer than 30 or 40 years.2–5 As earlier exposures to aromatic amines used in hair dyes could have an impact decades later, this means that the possibility of bladder cancer in hairdressers having worked with hair dyes during earlier decades (prior 1980) should be taken into account. Furthermore, a study conducted by Turesky et al6 demonstrates that aromatic amines with carcinogenic effect (derivatives of 4-aminobiphenyl) are still present in some commercial hair dyes.
The risk for bladder cancer among hairdressers has been examined in many epidemiological studies. But owing to small sample sizes and the resulting lack of statistical power the results of these studies have been inconsistent and significant associations have rarely been found.
Two reviews summarised available evidence on the association between hair dyes and cancer.2 7 But neither were the search strategies or inclusion criteria for the studies explained, nor were extensive meta-analyses carried out. Recently Reulen et al8 conducted a meta-analysis on the association between bladder cancer and occupation, among others in hairdressers. A small but significantly increased risk was determined for hairdressers in the pooled analysis, even for smoking-adjusted data. But due to the fact that Reulen et al8 worked on a total of over 60 occupational groups, a more detailed analysis for hairdressers was not possible and is still missing. None of the three reviews covered duration of exposure.
Therefore we conducted a meta-analysis to determine the risk for bladder cancer among hairdressers in more detail: pooled risk estimators stratified by study design, gender, study quality, duration of employment as hairdresser and adjusted by smoking were calculated.
Materials and methods
Search strategy and screening form
We conducted a MEDLINE, EMBASE, CENTRAL search for articles published after 1970 in October 2008 (update February 2009). The search terms included ‘Urinary Bladder Neoplasms’ [MeSH], ‘occupation’, ‘occupational exposure’ or ‘hairdresser’ and ‘hair dye’ or ‘hair color/colour’ or ‘hair colourant/colorant’. Additional studies were identified from the reference list of articles and relevant reviews. Three authors screened all abstracts and full texts by an initially developed screening form, which included the following inclusion criteria:
Study design: randomised controlled trial (RCT), case-control study or cohort study
Study population: the population included hairdressers
Exposure: job held as a hairdresser is clearly stated
Analysis: occupation is determined as a risk factor
Outcome: clinically confirmed diagnosis of bladder cancer
Languages: English and German
Studies which do not meet the inclusion criteria were excluded and the reasons for exclusion were noted. When the information provided by abstracts was insufficient to decide on inclusion or exclusion, we retrieved and evaluated the full text.
Assessment of study quality and the risk of bias
In concordance with the literature for the assessment of study quality of observational studies9–13 we generated six criteria. Each of these criteria were scored with one, two or three stars as follows:
A clearly stated aim9 10: reported and adequate (***), reported, but inadequate (**), not reported (*).
Response rate/trace rate11 12: ≥70% (***), ≥50% (**), <50% (*).
Comparability of subjects10–12: population-based controls (***), matching (**), no matching (*).
Elevation of exposure12: definition for job held ≥5 years (***), definition for job held <5 years (**), definition for ‘ever registered as a hairdresser’ or not reported (*).
Adequate statistical analysis and confounding10 11 13: adjustment for smoking (***), partially adjusted (**), non-adequate statistics or not adjusted (*).
Discussion of limitations and generalisability9: limitations and generalisability discussed (***), partially discussed (**), not discussed (*).
Two authors individually graded the study quality by a predefined form. In a consensus meeting the results were compared and potential disagreement was resolved following discussion.
We developed the grading system according to the process of the Methodological Index for Non-Randomised Studies (MINORS).10 Overall, 18 stars could be achieved. By summing up the stars, the studies were classified according to their quality:
17–18 stars=high-quality level
≤16 stars=moderate-quality level
Evaluation of heterogeneity
Heterogeneity is a consequence of methodological diversity between the studies and manifests itself in the observed effects being more different from each other than one would expect by random error (chance) alone. The absence of heterogeneity among studies indicates between-study comparability. We used the χ2 test to test for heterogeneity. Because the χ2 has lower power in the situation of a meta-analysis when studies have small sample size, we used a p value of 0.10 to determine statistical significance for heterogeneity. This means a non-significant result indicates absence of heterogeneity.11
Statistical pooling
The data for the statistical analysis were extracted by a predefined data extraction form. For the overall meta-analysis we extracted the sample size, the sizes of the case group and control group, the effect estimate, given as the OR or the standardised incidence ratio, or standardised mortality ratio (both abbreviated as SMR), respectively, with a 95% CI. When necessary, we contacted the authors of some studies for further clarification. Data extraction was individually carried out by two reviewers.
A summary risk ratio (SRR) was calculated using the generic inverse variance approach. The weight given to each study in the inverse variance approach is chosen to be the inverse of the variance of the effect estimate (ie, one over the square of its standard error (1/
If SE was not given by the individual study, an approximate standard error of the logarithm of the risk estimate was calculated as follows11:
In case of homogeneity we used a variation of the inverse variance approach with a fixed effect model and in case of heterogeneity we used the random effect model.11 14
For the overall meta-analysis we used unadjusted data. If unadjusted data were not published by the individual studies, smoking-adjusted effect estimates were used for the overall meta-analysis. For studies where only stratified data on sex were given, we summarised the data and calculated the effect estimate among both sexes combined to calculate the overall SRR. All analyses were carried out using Review Manager 5 and Microsoft Excel 2007.
Stratification
For the stratified analysis we additionally extracted, where given, smoking-adjusted and stratified data for various factors. We calculated the SRR stratified for study design, gender, study period (defined as the mean year of ascertainment of the bladder cancer cases), study area, adjustment for smoking and study quality. If no adjustment or stratification were given, the studies were excluded from the stratified analysis. In addition, we analysed whether the SRR varies by duration of job held as a hairdresser, because demonstration of this association would lend additional weight to a suspected cause–effect relationship. Therefore three mutually non-exclusive categories were defined: ever registered as hairdresser, job held ≥5 years and job held ≥10 years. If no definition for job held was given or if the categorisation used in the study did not fit neatly in this categories, the studies were excluded from this analysis.
Sensitivity analysis
Sensitivity analysis was carried out by recalculation of SRR after exclusion of each individual study in turn. This method of sensitivity analysis indicates the importance of each individual study in the combined meta-analysis and allows determination of whether any of these had a disproportionate influence.11
Publication bias
Following Egger et al57 we explored publication bias due to study size. First, we plotted the effect estimator versus the precision of the estimate (defined as the inverse of the standard error (1/SEi)) to explore publication bias due to study size. An asymmetry of this funnel plot indicates publication bias.57 Second, we tested the funnel plot asymmetry by a linear regression approach on the natural logarithm scale of the effect estimator. In this method the standard normal deviate (SND), defined as the effect estimate divided by its standard error, is regressed against the precision. The intercept provides a measure of asymmetry—the larger its deviation from zero, the more pronounced the asymmetry.57
Results
Studies identified and assessment of study quality
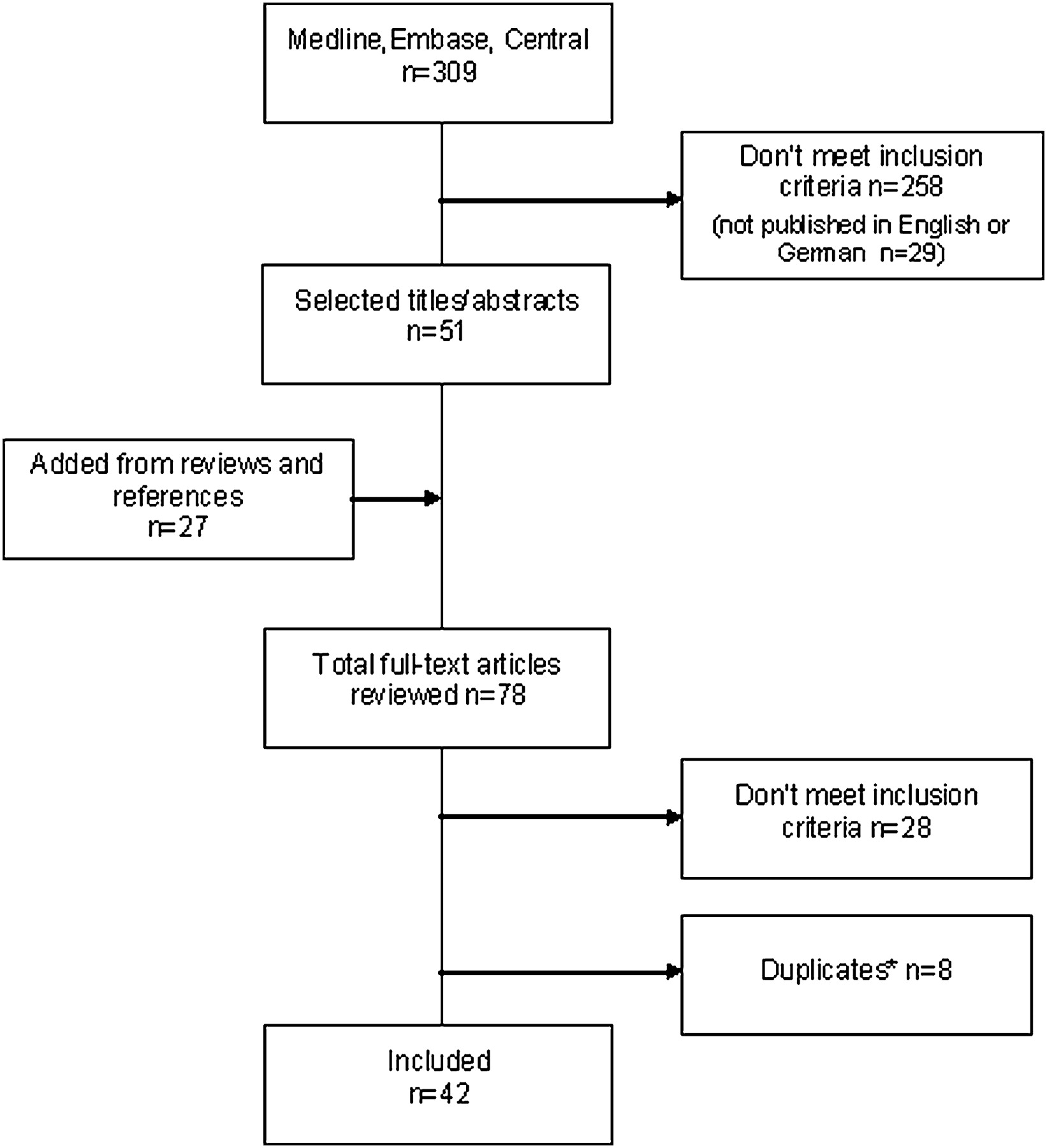
We identified 309 abstracts from the database search and 27 were added from references (n=336). Two hundred and fifty-eight were excluded, because they did not meet the inclusion criteria. Of these excluded studies, 29 were published in other languages than English or German, but 26 provided an English abstract. These abstracts were screened and 24 of them were excluded because they did not meet the inclusion criteria. The information of two abstracts was insufficient to decide on inclusion or exclusion. This means that we excluded five studies because of language issues alone. Finally, 78 studies needed to be reviewed as full-text articles and 42 articles met the inclusion criteria (figure 1).

Flow diagram of the process of identifying and including studies. *When the study population was described in more than one study, only the study with the greatest number of cases was included. All others were excluded as duplicates.
Of the included studies, 28 used a case-control design and 14 studies used a retrospective cohort design. RCTs or prospective cohort studies were not identified. The effect estimate for bladder cancer among hairdressers varied between 0.40 and 17.84, and the studies included from one up to 138 cases in hairdressers. Eleven studies were assessed as being high-quality studies; all of these studies had been case-control studies. Thirty-one studies were assessed as being of moderate quality, with 17 of these studies having a case-control design and 14 having a retrospective cohort design (table 1).
Abstracted study information and risk estimates for bladder cancer from the individual studies and assessment of study quality
Results of the overall meta-analysis
The meta-analysis of all included studies (n=42) showed a significantly increased SRR of 1.34 (95% CI 1.21 to 1.48) and the χ2 showed no evidence of heterogeneity (χ2 39.88, p=0.52) (table 2). Visual examination of the funnel plot to assess publication bias reveals no systematic relation between study size and magnitude of the estimator (OR/SMR) (funnel plot not shown). The statistical test applied did not show significant funnel plot asymmetry either (intercept 0.37; 95% CI −0.14 to 0.88).
Pooled estimates of bladder cancer among hairdressers: stratified analysis
Sensitivity analysis
Sensitivity analysis by exclusion of each study in turn did not modify the results of the meta-analysis and showed robust results. The SRR ranged from 1.33 to 1.37 and all SRRs were statistically significant (figure 2).

Forest plot showing the influence of excluding each individual study on the summary risk ratio (SRR) obtained using all studies for bladder cancer among hairdressers. Vertical dashed line=SRR obtained using all studies, vertical solid lines=95% CI of the SRR using all studies, block with line=SRR with 95% CI obtained by omitting the mentioned study. †For convenience reasons only the first author is given.
Stratified analysis
Figure 3 illustrates the forest plot of case-control studies and cohort studies. The SRR calculated for case-control studies was 1.41 (95% CI 1.51 to 1.74) and for cohort studies 1.32 (95% CI 1.17 to 1.48). Both plots showed a good overlap of the confidence interval and no evidence of heterogeneity (case-control studies: χ2 29.86, p=0.32; cohort studies: χ2 9.73, p=0.72). Drawing the funnel plot of case-control studies (intercept 0.66; 95% CI −0.46 to 1.78) and cohort studies (intercept 0.37; 95% CI −0.52 to 1.27) separately did not reveal asymmetry (funnel plot not shown).

Forest plot of studies by study design. Block=risk estimates (size displays weight), line=95% CI. †For convenience reasons only the first author is given.
Significantly increased risks and no evidence of heterogeneity were also found for stratified analysis shown in table 2. Small differences were found between studies stratified by gender: the risk for male hairdressers (SRR 1.52, 95% CI 1.34 to 1.72) was slightly higher than the risk for female hairdressers (SRR 1.25, 95% CI 1.05 to 1.50). Significant increased risks, but no trend with time, were found for the set of studies stratified by study period. The SRR for studies with ascertainment of cases ≤1979 was 1.37 (95% CI 1.19 to 1.58), the SRR for studies with ascertainment of cases between 1980 and 1989 was 1.24 (95% CI 1.00 to 1.53) and the SRR for studies with ascertainment of cases ≥1990 was 1.42 (95% CI 1.16 to 1.75). Nearly no difference in risk was found between studies from the USA/Canada and Europe/Nordic countries as well as between studies with smoking-adjusted data and studies with no adjustment. Also, no difference in the risk was shown between studies assessed as being high-quality studies or as being moderate-quality studies (table 2).
Duration of job held
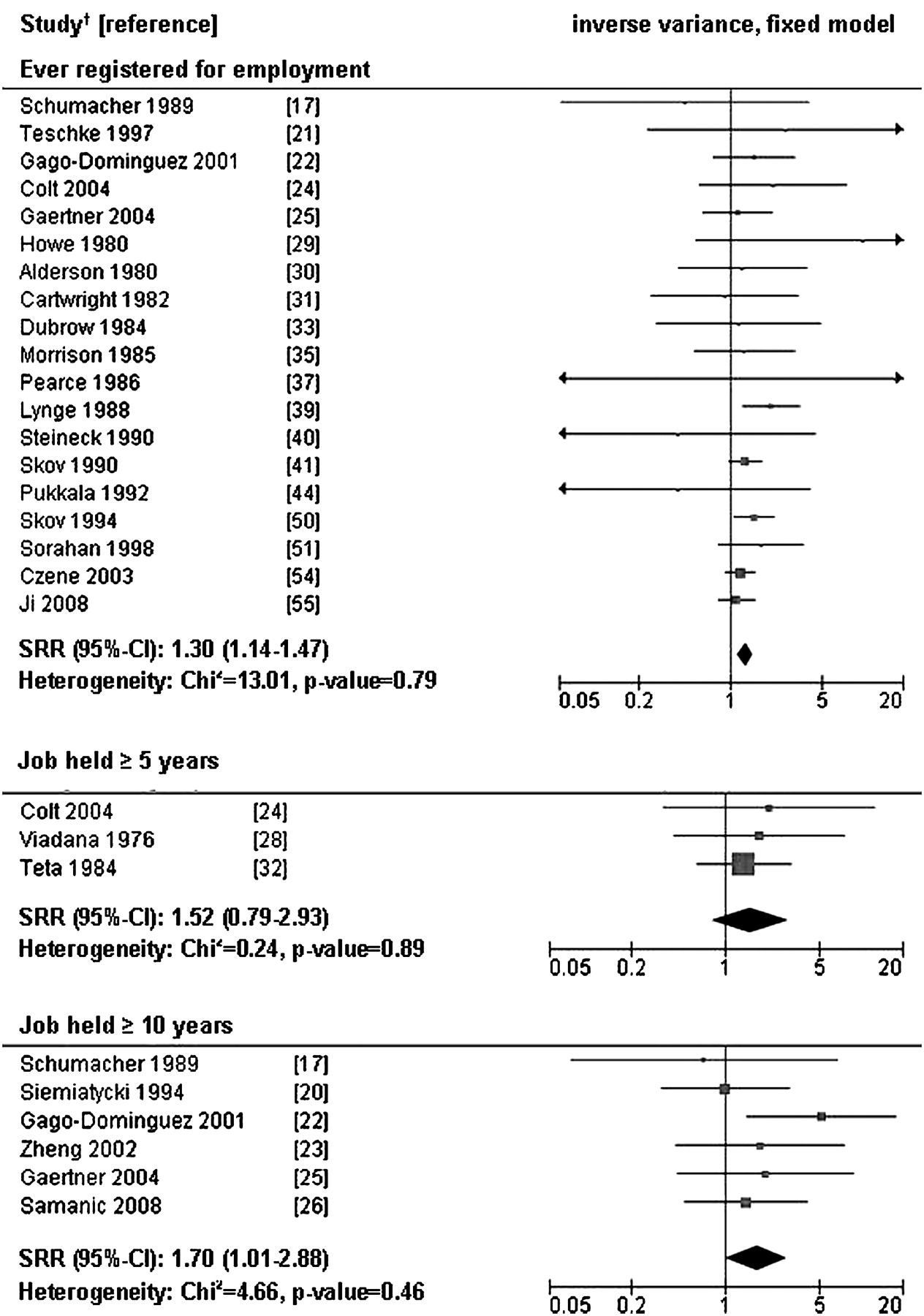
The risk of bladder cancer increased with the duration of employment as a hairdresser and all analyses showed no evidence of heterogeneity in all three strata. The SRR calculated for studies with data for hairdressers who were ever registered for employment (n=19) showed a risk of 1.30 (95% CI 1.15 to 1.48). The SRR calculated for studies with stratified data for job as a hairdresser held for ≥5 years (n=3) showed an increased, but not significant risk of 1.52 (95% CI 0.79 to 2.93) and the SRR calculated for studies with stratified data for job held ≥10 years (n=6) showed an increased and significant risk of 1.70 (95% CI 1.01 to 2.88) (figure 4).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Forest plot of studies by duration of job held as a hairdresser. Block=risk estimates (size displays weight), line=95% CI. †For convenience reasons only the first author is given. Studies 17 18 26 33 35 37 41 42 44–48 51 52 55 56 with no definition or unsuitable definition for job held were excluded form this analysis.
Discussion
We found significantly increased risks for bladder cancer among hairdressers in all but one analyses. To our knowledge this is the first meta-analysis approach covering bladder cancer in hairdressers that tested between-study comparability by evaluation of heterogeneity and that tested for publication bias. Furthermore the duration of employment as a hairdresser was considered for the first time and a predefined quality assessment tool was used.
Relevant literature and publication bias
We found 42 studies which met the inclusion criteria. Reulen et al8 found 29 studies which analysed this association. Even though the risk of bladder cancer among hairdressers is methodologically best observed in RCTs or prospective studies, our meta-analysis had to rely on observational studies, because RCTs or prospective studies were not found.
Another point is that the results of a meta-analysis might be affected by publication bias. Publication biases result from the probability that studies with a significant effect are more likely to be published in journals indexed in databases such as MEDLINE than studies which found no effect. In order to avoid such publication bias, we included also studies which were published in German and studies which were not published in indexed journals (eg, results of dissertations44 and reports from federal institutes).45 In addition, publication biases can also result from language bias, because studies published in other languages than English or German were not included in our meta-analysis. In order to assess potential language bias in our meta-analysis we checked the amount of studies published in other languages found by our search strategy and, if provided, the English abstract for inclusion criteria. Finally, if we had not applied our language restriction, five additional studies would have been included in our meta-analysis. Furthermore we formally tested for publication bias but did not find an indication for asymmetry of the funnel plot and consequently for publication bias.
Results of the meta-analysis and study quality
The SRR for all studies included in our meta-analysis was 1.34. Furthermore, we conducted a sensitivity analysis to evaluate the importance of each study in the overall meta-analysis and we found no evidence for a disproportionate influence of individual studies. In their meta-analysis, Reulen et al8 also found a significant but slightly lower risk of 1.24 (no test for heterogeneity or publication bias). In addition, in the review of La Vecchia7 the observed (O) and expected (E) cases of seven cohort studies were summarised and a risk of 1.4 was calculated by dividing O/E (no test of significance).
We pooled the data separately for case-control and cohort studies, because the study design has an impact on the methodological quality of studies. We found nearly the same risk for case-control and cohort studies with a statistically significant SRR of 1.3 and 1.4, respectively, and no evidence of heterogeneity as well as no indication of publication bias. Reulen et al8 also found nearly no difference between case-control and cohort studies, but with significant SRRs around 1.2, the risk was slightly lower (no test for heterogeneity or publication bias).
In addition, we assessed the quality and the risk of bias of the included studies, because irrespective of the study design there might be other issues of interest in terms of study quality. A number of checklists and indexes have been proposed, but none of these seemed to be suitable for our study question.10 13 Therefore in concordance with the literature and on the basis of recommendations for systems to rate the quality of observational studies9–13 we developed a quality assessment tool adapted for our study question. This tool has not been validated but it turned out to be suitable for our purposes.
However, following our assessment tool we found only case-control studies and no retrospective cohort studies for the high-quality level. This is not surprising because registry data have a number of limitations; these were also mostly the reasons for downgrading the study quality. First, information on occupation is not fully registered.47 Second, registry data contain no additional information on occupation, for example, about duration of job held.47 51 52 And third, information on potential confounders such as smoking is often missing. But well-designed studies based on registry data might also have benefits. They are routinely collected, provide a big amount of data with very little data missing and the data can be determined for several causes of death or diseases.47 Therefore registry data can provide important information to some potential health problems, especially for occupational health problems. This is also shown by a comparison study.47 The ability of death certificate data was compared with the ability of data of a population-based case-control study to identify high-risk occupations for bladder cancer. In this comparison the rate of agreement was 62%.
Case-control studies might also have limitations and were therefore assessed as being of moderate quality. Reasons were mostly a relatively low response rate and missing stratification for the duration of employment. In addition, the control group of some case-control studies was hospital-based and sometimes the control group was not chosen with matching.
Nevertheless, we found nearly the same risks with a significant SRR around 1.35 for high-quality and moderate-quality studies. In summary, irrespective of the study design and the level of quality we found consistent risks with a significant SRR around 1.3–1.4. This corroborates the interpretation that there is a causal association between bladder cancer and job held as a hairdresser.
Stratified data
We found significantly elevated risks and no evidence of heterogeneity in all sets of studies. The pooled risk estimator for female and male hairdressers differed slightly with statistically significant SRRs of 1.25 for females and 1.52 for males. More or less the same results were found by Reulen et al.8 They also established a slightly higher risk in males than in females. Some authors who found higher risks for male than for female hairdressers conclude that the risk for bladder cancer is mainly caused by exposure with brilliantine, which was used in the past for hair grooming in men.24 53 But in contrast, other studies found a higher risk for female than for male hairdressers.26 51 55 Nearly no difference in risk was found between studies from the USA/Canada and studies from Europe/Nordic countries. To our knowledge this comparison was not performed in other meta-analyses on bladder cancer among hairdressers.
Tobacco consumption is a well-established risk factor for bladder cancer.26 28 30 34 53 The pooled risk estimator for smoking-adjusted data in our meta-analysis showed with 1.35 nearly the same risk as the pooled risk estimator for no adjustment for smoking (both statistically significant). Reulen et al8 found a significant risk of 1.29 for smoking-adjusted data among hairdressers and an elevated but not significant risk of 1.20 for no adjustment for smoking. This makes it likely that confounding by smoking is of minor importance even though its influence cannot be completely ruled out because quite a few studies (n=19) did not control for confounding.
Risk by duration of job held
To our knowledge, the association between the duration of job held as a hairdresser and the risk of bladder cancer was not tested before by meta-analysis. The risk of bladder cancer increased with the duration of job held, in particular for hairdressers with a duration of job held for ≥10 years. The pooled data for the duration of job held ≥5 years were also elevated, but the effect was not statistically significant. The lack of a significant effect may be due to limited study power as only three studies provided data for job held ≥5 years.
Duration of working as a hairdresser was used as exposure surrogate. Because of the different ways duration was assessed in the studies, it was not possible to create mutually exclusive exposure categories, for example, the lowest category ‘ever registered as hairdresser’ might also contain hairdressers who worked for more than 10 years. However, our results suggest that there is an association between the duration of job held, especially for hairdressers with job held for ≥10 years, and this lends additional weight to a suspected causal relationship.
Time aspects and the risk of bladder cancer
It remains an open question whether current occupational exposure to modern hair dyes and other hair products is still related to some excess bladder cancer risk among hairdressers. The data of none but one53 study included in our meta-analysis are not eligible to analyse this association because the studies did not specify the calendar year during which exposure occurred.
In this respect, the year of case finding is of limited value when trying to distinguish different exposure periods. Because of the long latency times (30 or 40 years) even recently conducted analyses with bladder cancer cases ascertained after 199523–25 or after 200055 may observe risks caused by the exposure to aromatic amines included in hair products before 1980.
The analysis stratified for study period showed significant elevated risks, but no trend with time while Reulen et al8 found increasing risks with time in their meta-analysis. Risks of 1.18, 1.27 and 1.48 were found for ascertained bladder cancer cases in hairdressers before 1980, between 1980 and 1989, and after 1989, respectively.
In order to determine whether occupational exposure to modern hair products is still related to a risk for bladder cancer, it would be useful to determine whether hairdressers working before 1980 and hairdressers working after 1980 have the same risk. A Swedish retrospective cohort study conducted by Czene et al53 is the only study that distinguishes different exposure periods. Registry data with data of four exposure periods yielded declining SMRs: the risk for males registered as hairdressers between 1960 and 1969 was 2.56 (significant). The risk decreased to 1.35 for the period 1970–1979, to 1.25 for the period 1980–1989 and to 0.92 for the period 1990–1998 (all not significant). No increased risk estimate was found for female hairdressers, so the data were not presented.53 It remains unsettled to which extent this decline is explained by different latency periods or by a real decline in risk.
Conclusion
All our results taken into account, we conclude that there is good evidence for an increased risk of bladder cancer among hairdressers, in particular for hairdressers in jobs held ≥10 years.
We included 42 studies in our meta-analysis: no indication of publication bias or heterogeneity was found. We found SRRs in the range from 1.25 to 1.70 which were positively associated with duration of employment, rendering a causal association between bladder cancer and job held as a hairdresser likely. The risks for smoking-adjusted data were more or less the same than for data with no adjustment. Potential for residual confounding cannot be ruled out but this risk seems small. It remains an open question whether hairdressers working after 1980 only, when aromatic amines with known mutagenic or carcinogenic effects were banned from hair dye ingredients in the European Union, still present an increased risk for bladder cancer.
What this paper adds
Aromatic amines which were identified as carcinogenic for urothelial cancers were used in hair dyes and other hair products until the end of the 1970s.
In response, many epidemiological studies have been conducted to examine occupational risk factors for bladder cancer among hairdressers, but the results of these studies have been inconsistent.
The results of the present meta-analysis on 42 studies suggest that there is robust evidence for an increased risk of bladder cancer among hairdressers, in particular for hairdressers in a job held ≥10 years.
The data available from the individual studies do not provide adequate information to draw a conclusion regarding the question whether current occupational exposure to modern hair products is still related to some excess bladder cancer risk among hairdressers and therefore further research is needed.
Acknowledgments
We wish to thank Dana Wendeler for her great support with the management of the literature.
References
Footnotes
Competing interests None.
Provenance and peer review Not commissioned; externally peer reviewed.