Article Text

Abstract
Objectives: To study the effectiveness of using a computer mouse with a feedback signal for upper extremity musculoskeletal symptoms in office workers.
Methods: A randomised controlled trial with 8 months of follow-up was carried out. The intervention consisted of a computer mouse with a feedback signal. In total, 354 subjects were allocated to the intervention group or the control group. Measurements were performed with electronic questionnaires at baseline, after 4 months and after 8 months. Outcome variables were the prevalence and incidence of upper extremity musculoskeletal symptoms and disability in the upper extremities. The intervention process was evaluated by software registration.
Results: The use of the mouse with a feedback signal resulted in a significant decrease in duration of mouse usage over time. No differences were found in the number of mouse usage rest breaks. No differences were found in the prevalence (p = 0.29) or incidence (p = 0.832) of upper extremity musculoskeletal symptoms between the groups 8 months after baseline. The prevalence decreased from 49% at baseline to 44% after 8 months in the control group, while it remained at 36% in the intervention group. The incidence was 21% in the control group and 22% in the intervention group. Among the population with upper extremity musculoskeletal symptoms at baseline, the risk of experiencing symptoms after 8 months did not differ between the groups (p = 0.49). Minor disability was found in both groups. In the intervention group, a lower level of physical disability over time was reported than in the control group (p = 0.02).
Conclusions: A feedback signal computer mouse does not affect the prevalence and incidence of upper extremity musculoskeletal symptoms, but it does lower disability scores. Given the high prevalence, studying preventive interventions for upper extremity musculoskeletal symptoms is of high importance.
Trial registration number: ISRCTN13222474.
Statistics from Altmetric.com
High prevalence and incidence rates of work-related upper extremity musculoskeletal symptoms have been reported in office workers.1–3 A lot of attention has been paid to identify risk factors for upper extremity musculoskeletal symptoms among office workers: Ijmker et al4 reviewed the scientific evidence available for the association between the duration of computer usage and upper extremity musculoskeletal symptoms. The duration of computer work appeared to be a risk factor for developing complaints during office work, and, in particular, mouse usage seemed to be more predictive of symptoms than computer usage in general.4 Continuous static muscle contraction with insufficient breaks could result in reduced local blood circulation and muscle fatigue,5 6 which may be seen as a possible pathophysiological mechanism for the development of upper extremity musculoskeletal symptoms.
Because duration of computer usage is a risk factor, preventive interventions that reduce this duration in office workers would have high potential. The implementation of rest breaks may be a possible preventive intervention. Studies that focus on the effectiveness of the implementation of rest-break interventions have shown positive effects on discomfort.7–10 Furthermore, among office workers with upper extremity complaints, the use of pause software seems to contribute to the perceived recovery from these complaints,11 although the use of pause software does not decrease the frequency of complaints.11 However, as Brewer et al12 reported in their 2006 systematic review, only one high-quality study has been performed on the effect of rest breaks on musculoskeletal outcomes.11 Therefore, it is presently unclear if the positive effects of rest breaks on discomfort can be generalised to effects on upper extremity musculoskeletal symptoms. Since the association between the duration of mouse usage and upper extremity musculoskeletal symptoms seems stronger than the association of general computer work and symptoms,4 it is hypothesised that the introduction of rest breaks during mouse usage would be of more value in the prevention of upper extremity musculoskeletal symptoms or for decreasing the impact of symptoms in the upper extremity on a person’s physical functioning.
In 2005, a laboratory study exploring the effect of the use of a computer mouse with a tactile feedback signal during standardised computer tasks showed that the mouse with a feedback signal significantly increases the dynamic activation pattern of the wrist extensors.13 In addition, using the computer mouse with a feedback signal decreased mouse usage duration.14 Therefore, a mouse with a feedback signal seems to be a promising preventative measure for upper extremity musculoskeletal symptoms among office workers. However, the effect of this computer mouse on musculoskeletal symptoms has yet to be determined. Thus, to study the effect of a feedback signal mouse on upper extremity musculoskeletal symptoms among office workers, a randomised controlled trial was performed in the present study. It was hypothesised that, because of the expected increase in dynamic activation wrist patterns and the decrease in mouse usage duration, office workers will develop fewer new complaints and the prevalence of upper extremity musculoskeletal symptoms will decrease. Furthermore, it was expected that the use of a mouse with a feedback signal will decrease current physical disabilities due to upper extremity musculoskeletal symptoms.
The objective of this present study is to study the effect of a computer mouse with a feedback signal on upper extremity musculoskeletal symptoms. The formulated research questions are:
Is a computer mouse with a feedback signal effective in lowering the incidence and prevalence of upper extremity musculoskeletal symptoms in office workers compared with a regular mouse?
Is a computer mouse with a feedback signal effective in reducing physical disability due to upper extremity musculoskeletal symptoms in office workers compared with a regular mouse?
METHODS
Design
A randomised controlled trial was performed with one baseline measurement before randomisation and two post-measurements at 4 and 8 months after the start of the intervention.
Study population
Participants were recruited from a population of 800 office workers at a Dutch regional governmental institute. All employees were informed of the study’s goals and protocols and instructed to initiate participation by sending in a signed informed consent form. Office workers were eligible to participate if their working tasks consisted of mainly computer usage (for over 4 h a day) for at least 2 days per week. Furthermore, eligible office workers were required to work on a desktop computer, while those working exclusively on laptops were excluded. A total of 400 office workers each were randomly assigned to the intervention group and the control group. Figure 1 shows the flow chart of the study population.
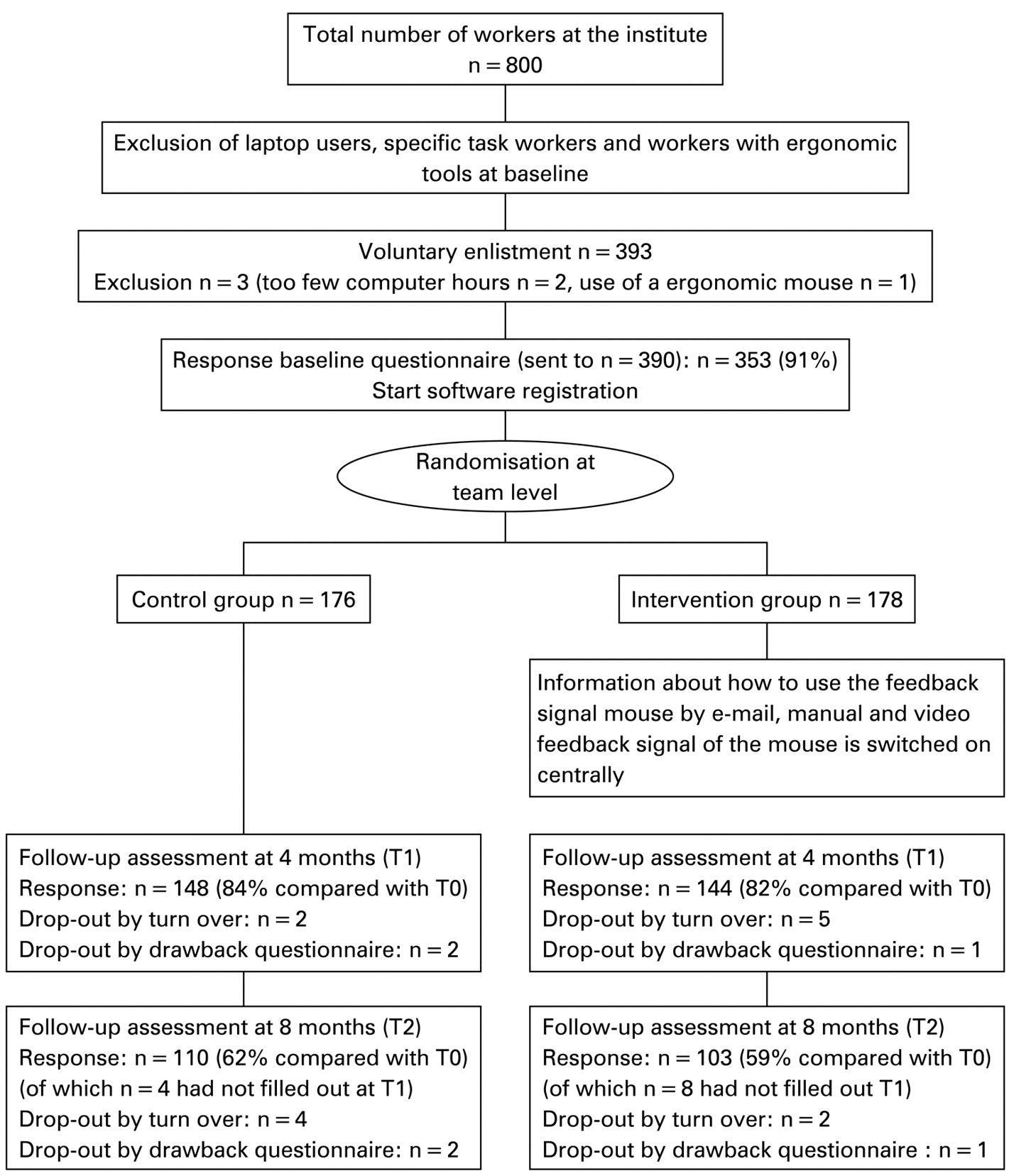
{kind=link}
Flowchart, protocol and design.
Intervention
The intervention consisted of a computer mouse with a sensor that detected the presence of a hand on or just above the mouse. The sensor monitored if the mouse was actually used (clicking, scrolling) or if the mouse was held passively and not being used. If the mouse was held for over 12 seconds without active usage, the mouse provided a feedback signal by means of a vibration signal to remind the user to take his or her hand from the mouse and to relax his or her hand and forearm by laying it down on the table.
The mouse feedback signal was switched on centrally by the information and communications technology (ICT) department of the governmental institute for only the intervention group. The used computer mice were identical in appearance. When receiving their randomisation assignment from the researchers, the intervention group was informed on how to use the mouse properly in a way that conformed to the manufacturer’s instructions. Participants were notified by e-mail, which included a link to an instructional video on the internet.
Outcomes
The outcome variables of this study were: prevalence of upper extremity musculoskeletal symptoms, incidence of upper extremity musculoskeletal symptoms, and physical disability due to upper extremity musculoskeletal symptoms. Outcomes were measured using a digital questionnaire three times: at baseline (before randomisation) and at two follow-up assessments, 4 and 8 months after baseline.
The incidence of upper extremity musculoskeletal symptoms was defined as having new symptoms in the neck, upper back, shoulder, elbow, forearm, wrist and/or hand, for at least 4 days within 1 week15 during: (1) the 4-month period before the first follow-up assessment and (2) the 8-month period before the second follow-up assessment. Incidence was determined among those participants who reported no upper extremity musculoskeletal symptoms at baseline (i.e., no complaints that encompassed at least 4 days within 1 week during the 12 months prior to the baseline questionnaire).
Prevalence of upper extremity musculoskeletal symptoms was defined as having symptoms in the neck, upper back, shoulder, elbow, forearm, wrist and/or hand for at least 4 days within 1 week,15 during: (1) the 4-month period before the first follow-up assessment and (2) the 8-month period before the second follow-up assessment.
Physical disability was assessed using the Dutch version of the “Quick Disability Arm Shoulder Hand” questionnaire (QDASH).16 The functioning scale of the QDASH consists of 11 activity items.16 Answers were on a numerical scale that ranged from “no difficulty” (1) to “unable to perform” (5). The sum scores was converted to scores ranging from 0 to 100, where 0 indicated no disability and 100 indicated maximum physical disability.
To explore the secondary preventive effects of this intervention, subgroup analyses on the 4- and 8-month prevalence and physical disability due to upper extremity musculoskeletal symptoms were performed for the population who reported symptoms at baseline.
Sample size
From earlier pilot data of the study population, the prevalence of upper extremity musculoskeletal symptoms was 45%.17 Due to the opportunity that arose to perform this field study, a preliminary sample size was not calculated; however, a total population of 800 office workers seemed large enough to detect a clinically relevant effect on the prevalence of upper extremity musculoskeletal symptoms.18
Randomisation
A computer-generated random sequence table was constructed before the baseline assessment. Eligible participants signed a written informed consent form after they were informed about the research goals, assessments, and the randomisation procedure. After written informed consent was received, the baseline measurements were conducted, and then the participants were randomised. Randomisation took place at the team level, where 45 teams were randomised using a series of random numbers. The participants within the teams were informed about the randomisation assignments. Double blinding for the intervention after baseline was not possible. Since all questionnaires were administered over the internet, biases due to researcher influence on the participants were unlikely.
Process evaluation
The registration software was part of the mouse software. The mouse registered the presence of the hand by a sensor. The threshold setting of the time interval of mouse use was 1 millisecond. The sensor also registered the hand as using the mouse when the hand was held just above the mouse. Registration started each morning at the first computer log-in and continued until the last log-out that day. This time period was defined as a working day. Mouse usage duration was defined as the mean percentage of the working day that the hand was clicking, scrolling, and resting on the mouse. The frequency of rest breaks from mouse usage was determined as the mean number of times the hand was removed from the mouse per hour during a working day.
Statistical analyses
Analyses were performed including participants with complete data and were conducted with SPSS 16.0 (SPSS Inc. Chicago (IL), USA). The significance level was set at p<0.05 for all outcome measurements. To analyse the differences between the intervention and control group in the 4- and 8-month incidence and prevalence as of the second follow-up assessment, the risks were compared between the groups using Chi-square tests. To analyse whether the mouse with a feedback signal had a main effect on physical disability over time (intervention x time), a linear mixed-model analysis was performed based on repeated measures with adjustments for cluster randomisation. The residuals were checked for normality. If this assumption was violated, the data were transformed to ranks, and the linear mixed-model analysis was performed on these rank scores as a non-parametric test.
For analysing the two process outcomes (duration of mouse usage and the frequency of mouse breaks), mixed-model analysis based on repeated measurements with adjustments for cluster randomisation were performed. Independent t tests were used to check if there were baseline differences between the analysed study population (the population with complete data) and the dropouts.
The subgroup analyses on prevalence and physical disability due to upper extremity musculoskeletal symptoms among the population who reported symptoms at baseline were performed in accordance with the analysis used to evaluate the main effects of the intervention over time as previously described.
RESULTS
Participants
In total, 354 participants filled out the questionnaire at baseline: 176 office workers (94 males, 82 females) were randomised into the control group, and 178 office workers (94 males, 84 females) were randomised into the intervention group (see fig 1). At baseline, the groups were comparable with respect to age (on average 44 years) and contract working hours per week (on average, 33 h in the control group and 32 h in the intervention group). Table 1 presents prevalence and incidence findings per group. At baseline, no differences were found for age (p = 0.81), workday length (p = 0.75), mouse usage (p = 0.55) and break frequency (p = 0.28) between dropouts and workers with complete data.
Process evaluation
Complete computer data were registered for 152 participants, including 70 (42 males) participants in the control group and 82 (42 males) participants in the intervention group. The average age of 43 years and the average contractual working hours of 33 hours per week were comparable with the total eligible population (n = 354, see paragraph above). The workday length did not differ between the two groups at baseline (7.1 h in both groups, p = 0.901) or over time (p = 0.626).
The duration of mouse usage over time differed significantly between groups (p = 0.03). Mean mouse usage duration in the control group increased from 19.9% of the working day (85 minutes) at baseline to 22.5% (105 minutes) after 4 months, and it then decreased again to 20.6% after 8 months (90 minutes). In contrast, mouse usage duration in the intervention group decreased from 18.6% of the working day at baseline (81 minutes) to 16.7% (76 minutes) 4 months later, and it increased again to 18.5% (82 minutes) after 8 months (table 2).
The frequency of rest breaks from mouse usage did not differ significantly between the two groups (p = 0.27). The number of breaks increased slightly from 33.0 to 36.5 per hour after 8 months in the control group. In the intervention group, the number of rest breaks from mouse usage increased from 33.5 at baseline to 42.2 per hour after 8 months (table 2).
Prevalence and incidence of upper extremity musculoskeletal symptoms
In total, 194 office workers filled out the prevalence and incidence question for all three measurements. At baseline, 49% of the participants in the control group (n = 50) and 36% of the participants in the intervention group (n = 33) reported upper extremity musculoskeletal symptoms (p = 0.084).
Table 3 summarises the 4-month and 8-month prevalence for the intervention and control groups. There was no significant difference in the 4- and 8-month prevalence of upper extremity musculoskeletal symptoms between the groups (p = 0.40 and p = 0.29). The relative risk (RR) of prevalent symptoms (95% CI) for the intervention group compared with the control group was 1.22 (0.77 to 1.95) after 4 months and 0.83 (0.59 to 1.18) after 8 months. Four months after baseline, 30% of the intervention group and 24% of the control group had upper extremity musculoskeletal symptoms. Eight months after baseline, 36% of the intervention group and 44% of the control group had upper extremity musculoskeletal symptoms.
In the determination of the incidence of upper extremity musculoskeletal symptoms, only the participants not reporting symptoms at baseline were included in the analysis (n = 111). Table 4 presents the incidence at 4 and 8 months of upper extremity musculoskeletal symptoms for the intervention and control group. No significant differences in the incidence at 4 and 8 months were found between the groups (p = 0.06 and p = 0.83). Four months after the start of the intervention, the RR (95% CI) of developing symptoms in the intervention group compared with the control group was 3.0 (0.89 to 10.48): 17% of the intervention group and 6% of the control group reported new upper extremity musculoskeletal symptoms that were not experienced at baseline or 12 months before baseline. Eight months after the start of the intervention, the RR (95% CI) in the intervention group compared with the control group was 1.08 (0.53 to 2.20): 22% of the intervention group and 21% of the control group developed upper extremity musculoskeletal symptoms that were not experienced at baseline or 12 months before baseline.
Table 5 summarises the 4-month and 8-month prevalence in the subgroup who reported symptoms at baseline (n = 83), for the intervention and control groups. No differences in prevalence were found after 4 months: 52% of the intervention group and 44% of the control group reported symptoms again (RR = 1.171 (0.743 to 1.846), p = 0.50). A total of 61% (n = 20) of the intervention group and 68% (n = 34) of the control group reported upper extremity musculoskeletal symptoms again 8 months after the baseline measurement. Thus, the relative risk of experiencing upper extremity musculoskeletal symptoms was 0.83 (0.64 to 1.25) for the intervention group compared with the control group. This difference was not statistically significant (p = 0.49).
Physical disability
In total, 183 office workers filled out disability questions (QDASH) for all three measurements. There was a significant main effect of the intervention on disability scores over time (p = 0.016). In the intervention group, the disability score decreased from 8.2 at baseline to 5.0 after 4 months. After 8 months, the disability score in the intervention group was 6.4. In the control group, the disability score decreased from a baseline of 7.1 to 6.8 after 4 months, and it then increased to 8.5 after 8 months (table 1).
Subgroup analysis of intervention effects on physical disability among participants who reported upper extremity musculoskeletal symptoms at baseline (n = 83) revealed differences between the groups at baseline. At baseline, the mean level of disability was 17.7 in the intervention group and 11.6 in the control group. After 8 months, disability increased to 13.6 in the control group, and, in the intervention group, the physical disability score decreased to 13.4. Again, a significant difference between the groups over time was found (p = 0.01).
DISCUSSION
This study evaluated the effects of a computer mouse with a feedback signal on upper extremity musculoskeletal symptoms among office workers. The process evaluation shows that the intervention reduces the duration of mouse usage. However, no significant difference in the number of mouse usage rest breaks was found between the groups over time. The main results show that prevalence as well as incidence of upper extremity musculoskeletal symptoms did not differ between the intervention group and the control group at 4 and 8 months after baseline. Four months after baseline, the relative risk of having symptoms was 1.2 (0.77 to 1.95), with 30% of the intervention group and 24% of the control group experiencing symptoms. Eight months after baseline, the relative risk of having symptoms was 0.83 (0.59 to 1.18), with 36% of the intervention group and 44% of the control group experiencing symptoms. Among participants who did not experience upper extremity musculoskeletal symptoms at or 12 months before baseline, the relative risk of new symptoms was 3.0 (0.89 to 10.45) after 4 months and 1.08 (0.53 to 2.20) after 8 months for the intervention group compared with the control group. In 17% of the participants in the intervention group and 6% of the participants in the control group, upper extremity musculoskeletal symptoms developed 4 months after baseline. Eight months after baseline, symptoms developed in 22% of the participants in the intervention group and 21% of the participants in the control group. Physical disability scores differed significantly (p<0.05) between the groups over time, with the intervention group reporting less disability compared with the control group in both the total group and the subgroup of office workers who reported upper extremity musculoskeletal symptoms at baseline.
In this study, the mouse usage duration significantly decreased, as was expected based on the results of the previous studies.13 14 Based on these same studies, it was also expected that the intervention would increase the frequency of mouse usage breaks, which would contribute to fewer new symptoms and a decrease of the prevalence of upper extremity musculoskeletal symptoms. However, no main preventive effect of the intervention was found. Van der Molen et al19 described three factors that might explain the absence of the expected intervention effect: lack of compliance, the intervention itself, and methodological implications.19 These factors may also be helpful to describe why the intervention did not affect the prevalence and incidence of upper extremity musculoskeletal symptoms in this study.
First, the duration of mouse usage and the frequency of mouse usage rest breaks were evaluated to gain an insight into participant compliance to the intervention. And, although the percentage of mouse usage per working day was significantly less in the intervention group compared with the control group (18.5% versus 20.6%), this difference is small and represents a reduction of 6 minutes of mouse usage during an average working day, at 8 months after the start of the intervention. This result can be explained in two ways: (1) the intervention did not decrease mouse usage or (2) participants’ compliance was low. Because two earlier studies on mouse usage behaviour showed large decreases in mouse usage while using a computer mouse with the feedback signal,13 14 participants’ compliance to the intervention may have been low in our study as well.
Main messages
Using a computer mouse with feedback signals does not prevent or reduce the risk of developing upper extremity musculoskeletal symptoms in office workers.
Using a computer mouse with feedback signals decreases the physical disability level in office workers.
Policy implications
Office workers with physical disability complaints may be offered a computer mouse with feedback signals as an intervention during computer work.
Implementation of ergonomic measures in the office environment, especially newly developed devices, should be based only on sound evidence of their efficacy.
Second, the intervention itself may be the cause of the poor intervention effect. The intervention was, among other things, focused on decreasing the duration of mouse usage. However, based on the duration of mouse usage at baseline, the mouse was held for only 85 minutes per working day in the intervention group and for 80 minutes in the control group. The relatively short exposure to the mouse usage may explain why this intervention was not effective in preventing upper extremity musculoskeletal symptoms in this study. Moreover, recent studies raise doubts about the association between computer use and upper extremity musculoskeletal symptoms.20 21 Although self-reported duration of computer use was positively associated with upper extremity musculoskeletal symptoms, the computer exposure registered by software was not associated with upper extremity musculoskeletal symptoms.21 However, both studies dealt with keyboard use; for mouse use only, there is a known association between self-reported mouse use and upper extremity musculoskeletal symptoms; moreover, the experimental computer mouse was specifically developed for preventing upper extremity symptoms in this population. However, when computer mouse duration registered by software would also be less associated with upper extremity musculoskeletal symptoms then this might be a reason for not finding a positive effect of the mouse on lowering the prevalence and incidence of upper extremity musculoskeletal symptoms.
Furthermore, the lack of intervention effect may be explained by the multifactorial origin of upper extremity musculoskeletal symptoms. It is known that the posture of the workers during computer work is another risk factor.22 23 Postures of the upper extremities and the neck are the same during both active computer usage use and during passive computer use, which includes reading from the screen and thinking about what to write or type. Since the computer mouse with the feedback signal only influences the risks associated with active mouse usage, the isolated preventive effect of the mouse upper extremity musculoskeletal symptoms may be of limited value.
The third factor that could explain the absence of expected intervention effects may be methodological. However, randomised controlled trials are the “gold standard” for determining the effectiveness of interventions. Furthermore, this randomised controlled trial was performed in a real office setting, which should increase the generalisability of the research findings compared with laboratory studies. Therefore, it seems that the lack of expected intervention effects is likely not due to methodological reasons.
It seems that the intervention increases the risk of experiencing symptoms in the short term indicated by a relative risk of 3.0 with a p value of 0.06, at 4 months after the start of the intervention. However, in calculating the long-term prevalence at 8 months after the start of the intervention, cases within the first 4 months were included, and the 8-month prevalence analysis shows that the prevalence did not differ between the groups. Therefore, it can be concluded that the intervention had no effect on the prevalence of upper extremity musculoskeletal symptoms. Additionally we explored the secondary preventive effects of the mouse by performing subgroup analyses among the population who reported symptoms at baseline. No effects were found: the prevalence was not affected but the level of disability decreased in the intervention group compared with the control group. These results indicate that the effect of the mouse was similar for office workers without symptoms as it is for office workers with upper extremity symptoms. It is possible, however, that usage of the intervention in a population of workers with daily active mouse usage of longer duration compared with the current population, may increase the chance of a preventive effect of the mouse with the feedback signal.
The intervention effectively decreased disability over time. However, in the total study population, the mean disability score was low (7.7), which raises some doubts about the clinical importance of this finding. These low disability scores may be expected because many participants did not have symptoms and all were able to work; thus, it is unlikely that they would report disability of the upper extremity. To determine whether changes in the full-length disabilities of the arm, shoulder and hand (DASH) scores are of any clinical importance, Gummesson et al24 suggested that a change exceeding 10 points is the most accurate for discriminating between improved and unimproved patients. Although the QuickDASH was used in this study, this 10-point threshold may be appropriately applied since the discriminating ability of these two questionnaires was found to be similar.25 In the post hoc analysis among participants who reported upper extremity musculoskeletal symptoms at baseline, the QuickDASH scores decreased during the 8-month follow-up in the intervention group (from 18 to 13), while the disability score in the control group increased during the same period (from 12 to 14). This indicates that the intervention was effective to decrease disability scores, but the clinically important difference of 10 points or more was not found. As a result, it may be expected that, among a population with a higher level of physical disability, the mouse with the feedback signal would result in a larger decrease in disability score than was observed in this study population.
In conclusion, no effects of the computer mouse with a feedback signal were found on the prevalence and incidence of upper extremity musculoskeletal symptoms in office workers. The feedback signal mouse resulted in less physical disability. Given the prevalence of upper extremity musculoskeletal symptoms of 40%, this study underscores the importance of studying preventive interventions for upper extremity musculoskeletal symptoms in real occupational settings. To be able to observe maximal effects of this computer mouse, it is recommended that the effect of the intervention be tested in a population of workers with durations of mouse usage that are longer than the duration observed in the present study. Furthermore, implementation of interventions that intervene on multiple risk factors may be potentially more effective in preventing upper extremity musculoskeletal symptoms.
Acknowledgments
We would like to thank all participants and the manufacturer of the computer mouse for its technical support. This trial has been registered at the Dutch national Trial register: ISRCTN13222474 (http://www.trialregister.nl/trialreg/admin/rctview.asp?TC = 44).
REFERENCES
Footnotes
Competing interests: None.
Funding: This project was funded by the Dutch Ministry of Social Affairs and Employment.
Ethics approval: The study was performed according to the Helsinki Declaration and was approved by the Medical Ethics Committee of the Academic Medical Center, Amsterdam, the Netherlands.
Patient consent: Obtained.