Article Text

Abstract
Objectives: The aim of this intervention study was to determine the effects of an alternative mouse and/or a forearm support board on the change in upper body discomfort scores and the development of incident musculoskeletal disorders.
Methods: This randomised controlled intervention trial followed 206 engineers for one year. Participants were randomised to receive (1) a conventional mouse only, (2) an alternative mouse only, (3) a forearm support board, or (4) an alternative mouse plus forearm support board. Outcome measures included weekly upper body discomfort scores and incident musculoskeletal disorders.
Results: During the study, 42 participants were diagnosed with an incident musculoskeletal disorder. The group that received the forearm support board experienced a reduction in their right upper extremity discomfort (beta-coefficient −0.35, 95% CI −0.67 to −0.03) in comparison to those who did not receive a forearm board. The group that received the alternative mouse had a protective, but non-significant (p = 0.20), effect on incident cases of right upper extremity musculoskeletal disorders (HR 0.57, 95% CI 0.24 to 1.34) and a non-significant reduction in neck/shoulder discomfort (beta-coefficient −0.23, 95% CI −0.056 to 0.10) in comparison to those who received a conventional mouse.
Conclusions: In engineers who use a computer for more than 20 h per week, a forearm support board may reduce right upper extremity discomfort attributed to computer use.
Statistics from Altmetric.com
Musculoskeletal disorders of the upper extremities and neck are the most common occupational health problem associated with computer users and account for the majority of work-related lost time from work.1 2 The most consistently observed risk factors are increasing hours of computer use and sustained awkward postures, such as the keyboard above elbow height.3–6 The hours of computer use, the use of the keyboard and mouse, and break patterns will vary by occupation and by the applications software used. Occupational use of computers has been studied in customer service operators,2 7 technical workers,8 9 newspaper reporters,10 11 clerical workers,12 13 and medical transcriptionists.12 Engineers represent an occupation with high daily use of computers and related musculoskeletal symptoms that may begin in college or during employment.14 15
Computer use by engineers can vary considerably from project to project; however, most engineering applications require a high percentage of time using a pointing device, such as a mouse or puck.15 The risk of upper extremity disorders, such as carpal tunnel syndrome, may be greater with mouse use than keyboard use.8 Cail et al demonstrated higher finger force exertion in computer-aided design activities in comparison to data entry tasks.16 Therefore, the management of musculoskeletal disorders among engineers may require more attention to the mouse design, mouse use patterns, and arm support during mouse use.
The forearm posture during use of a conventional mouse and keyboard requires working at the full range of forearm pronation; a posture that may cause increased forearm muscle loads and elevated tissue pressures.17 It has been postulated that this posture may increase the risk for forearm and wrist disorders. A prospective study by Aaras et al, of moderately symptomatic computer users at a telecommunications company, evaluated a mouse design which places the forearm in a more neutral posture.18 19 The alternative mouse (a 3M neutral forearm posture mouse) was associated with a long-lasting reduction in pain severity for the wrist/hand, forearm, shoulder and neck, and a reduction in lost time from work.20
A recent one-year randomised controlled trial found that a padded horizontal forearm support board reduced neck/shoulder and right distal upper extremity pain and musculoskeletal disorders among customer service operators.21 Customer service operators handle telephone calls and have mixed keyboard and mouse usage. Interestingly, a prospective study by Marcus et al found that the presence of a wrist rest was associated with an increase in hand-arm symptoms.4 But in the same study, the authors found that the placement of the keyboard more than 12 cm back from the edge of the desk, a position of potential forearm support, was associated with a reduced risk of hand-arm symptoms. The same authors conducted a six-month randomised intervention trial to evaluate the effect of adjusting the workstation to achieve some forearm support with the regular desk surface, but found no benefit from these workstation changes.22 Smaller field studies of forearm support have found mixed effects.23–26
The aim of this randomised controlled trial was to evaluate the effects of these same promising interventions among engineers. Specifically, the study was designed to determine whether a forearm support board and/or a neutral forearm posture mouse, when used by engineers with heavy computer usage, would (1) reduce the incidence of upper body musculoskeletal disorders, and (2) reduce discomfort severity.
METHODS
Study design and subjects
We report a one-year, randomised intervention trial with four treatment arms. The study was carried out from 2002–3 at a large aerospace engineering firm in California. The study design was reviewed and approved by the University of California San Francisco Committee on Human Research.
Employees were eligible for participation if they estimated that they worked at a computer for at least 20 h per week and were employed as a member of the engineering staff (93%) or a professional position supporting engineering (7%). The engineers included electrical, mechanical, design, industrial hygiene and quality engineering. The study also included other professional categories that support the engineering projects, such as computer programming, graphic design, financial planning, and project developers. Non-professional occupations, such as administrative assistants (secretaries) and production technicians (welders, machinists, test mechanics, plumbers, inspectors, carpenters, and facilities personnel) were excluded.
Potential participants were recruited at small departmental meetings where the study and eligibility criteria were described. All eligible employees were asked to complete a brief anonymous survey which collected baseline demographic information, self-reported hours of computer use at work, and discomfort ratings for the neck and upper extremities. Subjects were asked to estimate the number of days during the prior week they had difficulty working due to musculoskeletal discomfort and the number of days they took medications because of discomfort. This information was used to compare participants with non-participants.
Employees who met the eligibility criteria and agreed to participate in the study were asked to complete a health questionnaire and a weekly discomfort survey. Employees who completed the health questionnaire and at least four weekly surveys were eligible for participation in this study. Participants were randomised into one of four intervention groups. The randomisation was done by means of a computer-generated permuted-block sequence.
Interventions
The four workstation interventions were (1) a conventional mouse, (2) an alternative mouse with a neutral forearm posture, (3) the conventional mouse plus a forearm support board, and (4) the alternative mouse plus the forearm support board. The forearm support board is a large butterfly-shaped board (36 by 21 inches) that is attached to a desk and provides padded forearm support (ButterflyBoard, Metamorphosis Design and Development, Atlanta, GA, USA). The board is inclined upwards at approximately 5° and the surface can accommodate a keyboard and mouse (see online fig 1). The conventional mouse uses an optical LED for tracking the mouse movement and requires the hand to be in an almost fully pronated posture during operation (IntelliMouse Optical, Microsoft Corporation, Redmond, WA, USA). The alternative mouse is a 3M product that has a vertical handle for grasping and a flat base to support the ulnar side of the hand and uses a roller ball for tracking. The forearm is in approximately 15° of pronation during use (Renaissance Mouse, 3M Corporation, St Paul, MN, USA).

All subjects had a workstation with separate adjustable height surfaces for the keyboard and monitor. For all participants, the chair and workstation were adjusted so that the feet were flat on the floor, keyboard and monitor were directly in front of the subject, and the top of the monitor was at eye level. For those who did not receive the board, the desk height was adjusted so that the keyboard was approximately at elbow height. For those who received a board, the height was adjusted so that the forearms were supported by the board while the keyboard and mouse were used. Minor adjustments were encouraged to improve comfort. One month after the intervention an unannounced visit to the participant confirmed compliance.
OUTCOME MEASURES
Baseline health questionnaire
Upon entry into the study, each subject completed a baseline health questionnaire. The health questionnaire also collected information on possible confounders including age, marital status, gender, ethnicity, highest level of schooling, medical history, medications, smoking history, years at this job, hobbies, exercise habits, work schedule flexibility, psychosomatic complaints, exhaustion, physical functioning, emotional functioning, role functioning, job strain, social support at work, job security, job dissatisfaction, and effort/reward imbalance.27–30
Weekly discomfort survey
Each week participants were sent an email message with a link to the online weekly discomfort questionnaire. Those who did not respond to the initial email message were sent one reminder email. The questionnaire assessed work schedule, hours of computer use, upper body discomfort, medication use for discomfort, and acute injury events during the previous week. Three body regions, the neck/shoulders, right elbow/forearm/wrist/hand and left elbow/forearm/wrist/hand, were assessed for the worst discomfort during the preceding seven days using a 0–10 point scale (0 = no discomfort; 10 = unbearable discomfort).13
Subjects were asked whether they thought the discomfort was the result of (1) working on a computer, (2) an acute injury at work, or (3) activities or an injury away from work. Only discomfort reported by the subject as a result of working on their computer was included in the data analysis. In addition to rating their discomfort level, the subjects noted how many days they took medications because of discomfort. If the weekly survey indicated that the employee had new computer equipment, a new computer workstation or a new job assignment, a visit was made to their worksite to see if adjustments were needed.
Physical examination
Beginning four weeks after the intervention, subjects were assessed each week for the potential presence of a musculoskeletal disorder related to computer use. If the subject reported a discomfort intensity level of more than 5 on the weekly survey, or if they used a pain medication for two days or more per week for upper body discomfort that they thought was related to computer work, then the subject was referred for an examination. The examination protocol focused on the body region with discomfort and was performed by one physician who was blinded to the intervention status. The examination protocol assessed for the presence of 40 upper extremity and neck musculoskeletal disorders (for example, de Quervain’s tendinitis, carpal tunnel syndrome, epicondylitis, supraspinatus tendonitis, etc).13 21 A suspected case of carpal tunnel syndrome or ulnar neuritis at the wrist was confirmed with nerve conduction testing. This nerve conduction testing was performed using an automated electrophysiological neurodiagnostic device (NC Stat, Neurometrix, Waltham, MA, USA). Details regarding the device and method of measurement have been reported.15 The results are adjusted for age and height.31
An incident musculoskeletal disorder was defined as a disorder diagnosed on the physical examination, but only if the participant did not, prior to the intervention, report discomfort >5 in the same body region (neck/shoulder, right upper extremity, or left upper extremity).
Exit protocol and data
When the subjects left the study, either as dropout or because the study ended, they completed an exit questionnaire. The questionnaire collected information on why they exited the study and on whether the intervention was easy or difficult to use and any problems with the intervention.
Data analysis
The analysis followed an intention-to-treat approach. The objective of the study was to compare those who received an intervention with those who did not. Thus, those who received the alternative mouse were compared with those who received the conventional mouse. In a separate analysis, those who received the forearm support board were compared with those who did not receive the board. The study design allowed for evaluation of interaction, but the interaction terms were not significant. The incidence of neck/shoulder disorders was expected to be 35%.13 Based on this expected incidence, the study has an 80% power to show a 26% change in disorder risk at the two-sided 5% level for those who received the interventions and the reference group.
The Cox proportional hazards model was used to calculate hazard ratios for the interventions with respect to incident cases for each of the three body regions. The Cox proportional hazard model considers the time to an event in the calculation of the hazard ratio. A hazard ratio of less than 1 indicates that the risk of developing a musculoskeletal disorder was smaller in those who received the intervention compared with those who did not receive the intervention. The covariates of age, gender and one psychosocial variable measuring job stress (effort/reward imbalance) were forced into all models to control for these potentially strong confounders. Of the 23 covariates that were considered, covariates that did not appear to be evenly distributed among the intervention groups were individually examined for additional confounding in multivariate models that included the forced covariates. Covariates that did change the hazard ratio by 10% or greater were added into a final model.
A “pre-intervention mean discomfort” score was obtained from the weekly surveys before intervention by averaging all the pre-intervention scores for each subject to a single value. A series of “post-intervention mean discomfort scores” was obtained from the weekly surveys after the intervention. These scores were collapsed into a single post-intervention score by body region. The maximum duration for the post-intervention surveys was limited to 52 weeks and observations were right-censored after the 52nd weekly survey. If the subject failed to fill out a weekly survey, missing data were replaced with an average score from the scores that preceded and followed the missing data. The first eight weeks of post-intervention scores were left-censored in order to eliminate symptoms secondary to adapting to the intervention. An outcome variable that represented the change in the mean discomfort score was formed by subtracting the mean pre-intervention score for each body region from the respective mean post-intervention score. This measure was used for the analysis of the effect of the intervention on discomfort severity in the three body regions. General linear models were used to calculate the beta-coefficient and 95% confidence intervals for the interventions for each of the three body regions. A negative coefficient indicated that the discomfort declined more in those who received the intervention compared with those who did not receive the intervention. A positive coefficient indicated that the discomfort decreased less in those who received the intervention compared with those who did not. As with the Cox proportional hazard models, the covariates of age, gender and effort/reward imbalance were forced into all models. The approach to the inspection of covariates was similar to that used in the Cox proportional hazards model. Covariates that did change the β-coefficient by 0.05 or greater were added into a final model. The list of covariates included in the final model is presented in the footnotes of the respective tables.
RESULTS
During the recruitment seminars, all eligible employees (n = 437) filled out the initial questionnaire that provided baseline characteristics for all attendees regardless of whether they chose to participate in the study. Of the 437 eligible employees, 206 (47%) consented to participate in the study. The 206 study participants differed from the 231 non-participants in several characteristics (see online table 1). Females were more likely to volunteer for the study than males (p<0.01). Participants had higher levels of right arm and neck/shoulder discomfort (p<0.01). Participants were also more likely to take medications for discomfort related to work and had higher estimates of the number of days at work that were affected by discomfort (p = 0.05). Study participants did not differ from non-participants on hours worked per week, hours per week on a computer at work or total hours per week on a computer.
Most baseline demographic and psychosocial characteristics of the participants did not differ substantially by intervention group (table 1). However, oophorectomy, birth control pill use, hours of aerobic exercise per week and mean pre-intervention discomfort scores differed substantially between groups. Based on whether these variables had a significant effect on the respective model, these variables were added to the final multivariate models to adjust for this apparently unsuccessful randomisation.
During this 52-week study, 114 of 206 subjects completed an entire year while 92 subjects contributed a partial year, dropping out before the 52nd week. During the first two months of the study, more subjects dropped out of the alternative mouse intervention groups than the conventional mouse intervention groups (see online tables 2 and 3). Common complaints during the first month about the alternative mouse among subjects who left the study early included pain and difficulty adapting to the alternative mouse. A common early complaint about the forearm support board was an inability to accommodate the board to their workstation because of insufficient space.
Incident musculoskeletal disorders
Over the 52 weeks of the study, 56 of the 206 participants reported either the presence of upper body discomfort levels greater than 5 or the use of pain medication for upper body discomfort. These 56 subjects received a physical examination and 51 were diagnosed with a musculoskeletal disorder. Forty two of these subjects qualified as incident musculoskeletal disorder cases. Subjects could receive more than one incident diagnosis; 18 received at least one diagnosis in the neck/shoulder region, 25 received a diagnosis in the right upper extremity and nine received a diagnosis in the left upper extremity. The frequencies of incident disorders by intervention group are presented in table 2. All 206 subjects had at least one body region that was asymptomatic (for example, discomfort ⩽5) at the start of the study; therefore, all participants were eligible to become an incident case.
Crude and adjusted effects of the interventions, in comparison to the respective reference group, on incident regional disorders were examined using the Cox-proportional hazard model for the three body regions (table 3). The adjusted model for the alternative mouse intervention demonstrated a strong protective effect on incident cases of right upper extremity musculoskeletal disorders with a hazard ratio of 0.57, although this effect was of borderline statistical significance (p = 0.20). None of the other crude or adjusted effects was significant or of borderline significance.
Discomfort scores
The mean change in discomfort score for each intervention group by body region is presented in table 2. For the change in discomfort score, the crude and adjusted effects of the interventions were examined by body region using linear regression analysis (table 4). For the neck/shoulder region, the crude models showed a protective effect in both the alternative mouse and forearm support board intervention groups. After adjusting for covariates, the beta-coefficient for the alternative mouse intervention remained protective at −0.23 for reducing neck/shoulder discomfort with borderline statistical significance (p = 0.17). However, for the forearm support board intervention, after adjustment, the beta-coefficient declined to a neutral effect at −0.02 (p = 0.89). For the right upper extremity, the alternative mouse intervention showed a weakly protective effect that was not statistically significant. The forearm support board intervention, however, was protective for right upper extremity discomfort in both the crude and adjusted models with a beta-coefficient of −0.35 (p = 0.035) for the adjusted model. This indicates that the forearm support board intervention was associated with a 0.35 point greater mean reduction in discomfort on the 0–10 point discomfort scale, in comparison to the reference group. Both the alternative mouse and forearm support board interventions were associated with relatively neutral effects on discomfort scores for the left upper extremity.
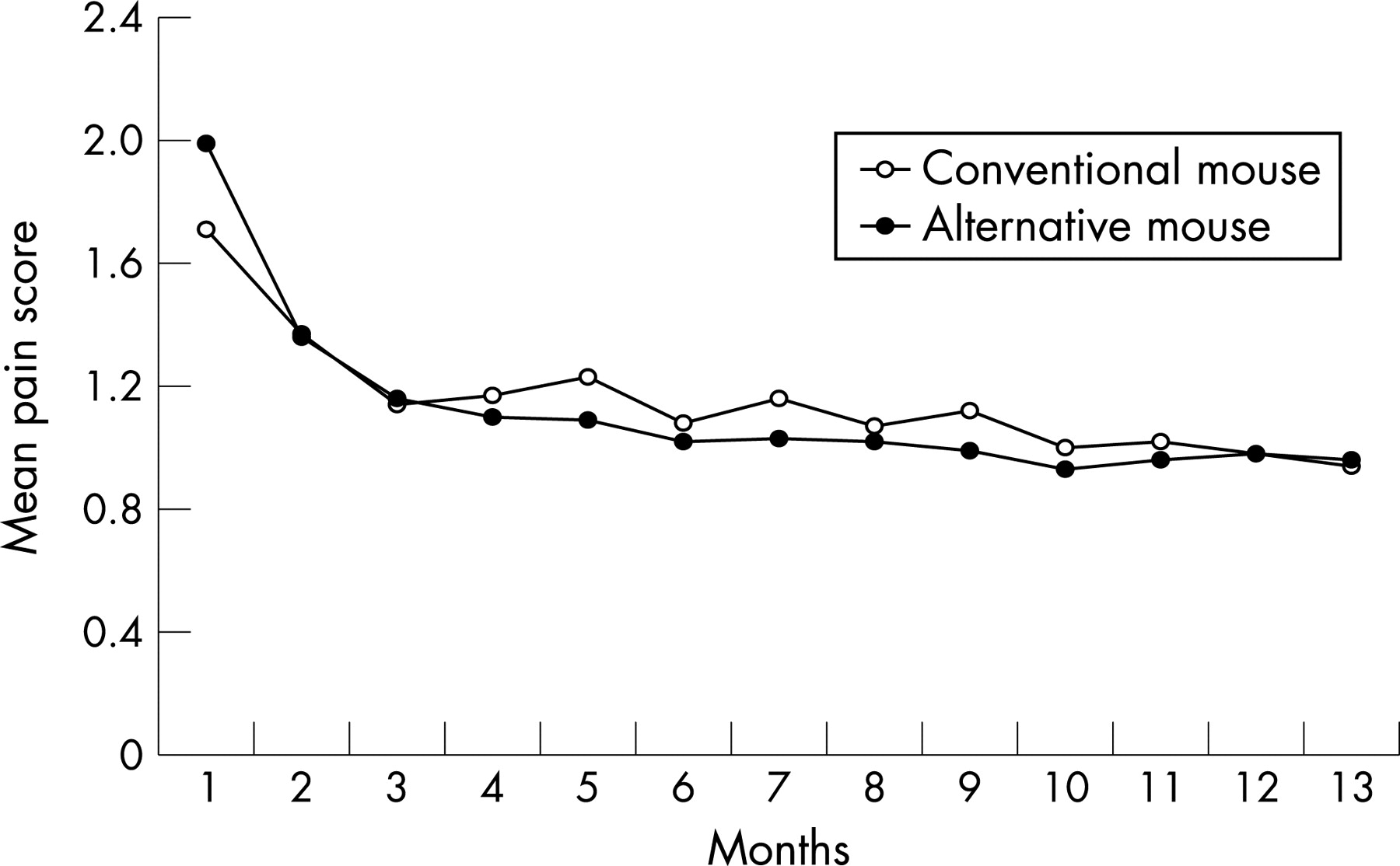
Figures 1 and 2 show the crude mean discomfort scores by month for right upper extremity discomfort by those who did and did not receive the forearm support board intervention and for neck/shoulder discomfort for those who did and did not receive the alternative mouse.
{kind=link}
{kind=link}
In a post hoc analysis, several covariates, including age, body mass index (BMI), computer hours at work and baseline discomfort levels, were dichotomised into high and low groups to evaluate whether the effect of the interventions on mean discomfort scores was modified by these variables. For example, dichotomised age was used to determine whether the effect of interventions on discomfort differed for older versus younger engineers. The association between these predictors and the change in mean discomfort scores by region was examined by linear regression. From these analyses there were interesting effects for the alternative mouse intervention with greater discomfort reduction effects on right upper extremity for the older age group (over 44 years of age) and for those with higher initial discomfort levels (right upper extremity discomfort levels greater than 2.0). There was also greater discomfort reduction effects for the neck/shoulder region for higher BMI (>30) and for higher baseline computer hours at work (>30 h/week computer use). For the forearm support board intervention there was greater discomfort reduction for both the right upper extremity and the neck/shoulder region for those with higher initial discomfort levels (discomfort levels >2.0) and for the right upper extremity with higher computer hours at work.
DISCUSSION
The findings of this randomised controlled trial suggest that providing a forearm support board may reduce right upper extremity discomfort attributed to computer use. There was no significant effect of either the alternative mouse or the forearm support board on upper body musculoskeletal disorders. On average, the forearm support board reduced right upper extremity discomfort by 0.35 points and the alternative mouse reduced neck/shoulder discomfort by 0.23 points in comparison to the reference group on a 0–10 point scale. The standardised effect size of the board was 0.21 for right upper extremity discomfort and the standardised effect size of the alternative mouse was 0.13 for neck/shoulder discomfort (standardised effect size = effect size/standard deviation; for example, −0.35/1.66 = −0.28). Some subjects reported difficulty using the alternative mouse and the forearm support board and increased discomfort with use of the alternative mouse was common during the first month of the study.
A previous prospective study by Aaras et al of moderately symptomatic computer users at a telecommunications company found that the alternative 3M mouse led to a large significant reduction in pain severity for the wrist/hand, forearm, shoulder and neck, but no significant change in the control group.18–20 The average pain level at baseline in these studies averaged about 50 mm on a 100 mm visual pain scale, which is much higher than our average pre-intervention discomfort level scores. Our study found a much smaller, non-significant effect, which may have been due to the lower baseline discomfort levels of our participants.
The effects of forearm support on upper body discomfort or musculoskeletal disorders have been mixed. In a one-year randomised controlled trial of 184 customer service operators, Rempel et al found beneficial effects of a forearm support board on incident neck/shoulder disorders as well as neck and right upper extremity pain scores.21 The forearm support board was different from the one used in our study, in that it was smaller, padded, and provided a level support surface about 2.5 cm above the keyboard support surface. Two other studies adjusted the workstation and chair of computer users so that the work surface or the chair arm supports would provide forearm support. Neither study found a significant benefit of forearm support on upper body pain or disorders.22 24 It appears that providing a separate support board confers a benefit that is not provided by just adjusting the workstation. It is difficult to not use an attached forearm support board, whereas an adjusted workstation can be adjusted back to provide no forearm support. The boards also elevated the forearms above the level of the bottom of the keyboard and may have led to less wrist extension.
The beneficial effect of forearm support on the neck and shoulder appears to be through the reduction of shoulder muscle loads. In two laboratory studies, forearm supports reduced trapezius muscle loading as recorded by electromyography.23 25 However, Tepper et al found that a device that provided an inclined working area was not associated with a decrease in trapezius muscle activity by surface electromyography.26
A potential limitation of our study was the small number of observed incident cases per body region and treatment group. These small numbers reduced the precision of our estimates for the Cox analysis and the power of the study, and introduced unstable hazard ratios for some of our outcome measures. For example, the highest incidence of disorders by region was 18% for right upper extremity musculoskeletal disorders (for example, conventional mouse intervention group). Based on this incidence and 103 subjects in each comparison group, the study had an 80% power to identify a 15% decline in incidence (for example, a decline from an incidence of 18% to 3%). In addition, the relatively low baseline discomfort scores may have reduced the ability of the study to identify beneficial effects of the interventions. Indeed, in the post hoc analysis, greater beneficial effects were observed among subjects with higher initial discomfort scores. Finally, while residual confounding may have occurred, the prospective format of the study and relative success of randomisation should have minimised this bias. Important known potential confounders were controlled for in multivariate analyses, including age, sex and psychosocial job factors. Strengths of this study included the length of the study, the frequent repeated sampling, the time sensitive Cox analysis, and adjustment for psychosocial job factors.
As noted above, participants had higher baseline discomfort scores and differences in other factors possibly related to musculoskeletal disorders (pain medication use and days off work for work-related discomfort) compared with non-participants. Therefore, readers should be cautious when generalising the study findings to asymptomatic computer users.
The findings of this randomised controlled trial suggest that a large forearm support board may reduce right upper extremity discomfort attributed to computer use among engineers who use a computer for more than 20 h/week. There was a trend for the alternative mouse to reduce neck/shoulder discomfort and right upper extremity musculoskeletal disorders, but the effects were not statistically significant. Some subjects had difficulty using the alternative mouse for their tasks and many rejected the alternative mouse during the first month. Some subjects found that the forearm support board took up too much of their work surface. The findings of this study may be relevant for other computer users, to the extent that the keyboard and mouse use patterns are similar. Engineers differ from other computer users, such as customer service workers, in that they generally have greater decision latitude and control of their work. They also use different application software. However, the keyboard and mouse use patterns may be similar to other occupations.
Main messages
Incident musculoskeletal disorders are common in computer users.
Forearm support at a computer workstation is associated with a reduction in right upper extremity discomfort.
In this population, there was no significant effect of the alternative mouse or the wide forearm support board on right upper extremity and neck musculoskeletal disorders.
Policy implication
Forearm support for computer users appears to be a reasonable intervention for the treatment of right upper extremity discomfort.
Acknowledgments
The authors thank Chris Shaw for subject recruitment and data collection, Gary Urbiel Goldner for his assistance in data analysis, Mark Hudes for his advice on biostatistics and Y C Hsia for his programming work on the intranet questionnaire.
REFERENCES
Footnotes
▸ Additional figure and tables are published online only at http://oem.bmj.com/content/vol65/issue5
Competing interests: None declared.