Article Text

Abstract
Objective: To estimate the occurrence of hand eczema in hairdressers in Sweden.
Methods: The occurrence of hand eczema was estimated in a Swedish longitudinal retrospective cohort study including all female graduates from vocational schools for hairdressers from 1970 to 1995. A stratified sample from the general population acted as controls. A self-administered questionnaire including questions on the occurrence of hand eczema, skin atopy, working periods and number of hair treatments performed per week was sent to the participants. Incidence rate ratios (IRRs) of hand eczema were estimated.
Results: The incidence rate of hand eczema in hairdressers was 23.8 cases/1000 person-years, whereas in hairdressers who were aged <25 years it was 37.1/1000 person-years. The corresponding IRR for hairdressers compared with controls was 2.5 (95% confidence interval (CI) 2.2 to 2.8), and that for younger hairdressers was 3.1 (95% CI 2.6 to 3.5). The mean age at onset of hand eczema was 21.6 years for hairdressers and 21.2 years for controls. The 1-year prevalence of hand eczema was 18.0% for hairdressers and 12.1% for controls. A large number of hair treatments involving exposure to skin irritants and sensitisers were reported. The incidence rate of hand eczema was higher among individuals with a history of childhood eczema, both for hairdressers and for controls, giving an (age-adjusted) IRR of 1.9 and 2.2, respectively. The attributable fraction of hand eczema from skin atopy was 9.6%. A synergistic effect of skin atopy and hairdressing was found on the occurrence of hand eczema. The relative excess risk due to interaction was 1.21 (95% CI 0.21 to 2.21; p = 0.01).
Conclusion: Hairdressers are highly exposed to skin-damaging substances. The self-reported incidence of hand eczema was substantially higher in female hairdressers than in controls from the general population and than that found previously in register-based studies. For many individuals, onset of hand eczema occurs early in life. Only about 10% of the hand eczema cases among hairdressers would be prevented if no one with skin atopy entered the trade.
- IRR, incidence rate ratio
- RERI, relative excess risk due to interaction
Statistics from Altmetric.com
There are about 19 000 hairdressers in Sweden, of whom 80–90% are women and most are self-employed, working in small salons. Hand eczema is a well-known problem in occupations that involve largely manual work, particularly in combination with long periods of wet exposure and skin contact with chemicals. Hairdressing includes extensive wet work, which can cause irritant contact dermatitis. Many hair cosmetics such as hair colourings, permanent wave solutions and bleaches can also cause contact allergy. Previous studies on the occurrence of hand eczema in hairdressers give a cumulative prevalence of 17–42%.1,2 A high prevalence (24–70%) and incidence rate (152–328 cases/1000 person-years) of hand eczema have been found among apprentice hairdressers.3–5 The only studies presenting incident rates of hand eczema in active hairdressers are based on registers of industrial injuries, which report incidences of 5.6–9.7/1 000 person-years.6,7 Registers of occupational skin diseases probably underestimate the actual occurrence of disease owing to under-reporting.8 The objective of this study was to estimate the incidence of hand eczema and occupational skin exposure in female hairdressers using a self-administered questionnaire.
METHODS
The design was a longitudinal retrospective cohort study with a self-administered postal questionnaire. The study was approved by the Ethics Committee at Lund University, Lund, Sweden.
Subjects
Study population
The study population consisted of women born after 1945 who had graduated from vocational schools for hairdressers in Sweden during 1970–95. The hairdressing programme in Sweden comprises 3 years. Altogether, 7203 trained hairdressers were identified. A questionnaire was mailed to them in December 1996. After two reminders, answers were obtained from 4061 (56%) hairdressers. Of these, 396 (10%) reported having never worked as hairdressers after their initial training, leaving 3665 for the analysis. Table 1 shows their age distribution. In the latest period of employment, most hairdressers (80%) had worked for>30 h week.
Descriptive and self-reported data for the female hairdressers and the population controls
Controls
A total of 7355 women, stratified by age and randomly selected from the Swedish population register, constituted a population-based control group referred to as “population controls”. After two reminders, 5034 (68%) returned the questionnaire. Table 1 shows their age distribution.
Questionnaire
Hairdressers and controls were administered a questionnaire containing questions about hand eczema and atopy history (see appendix). The questionnaire also contained items on respiratory symptoms, information that has been published elsewhere.9,10 The hairdressers were asked to state the calendar year of all periods of employment as a hairdresser from the time they had graduated. They were also asked to state whether there had been periods of >1 year during which they had not worked as hairdressers. For each employment period, the hairdressers were asked about the number of hair treatments they performed per week. The different treatments asked for were permanent waving, different hair colourings, hair bleaching, shampoos and use of hair spray. A question on glove use during hair treatments was also asked.
Non-responders
Altogether, 584 of the hairdressers and 217 of the controls (about one fifth and one tenth, respectively) who had not returned the questionnaire were randomly selected for a telephone interview by a nurse. Interviews were performed with 392 (67%) hairdressers and 134 (62%) controls. Altogether, 368 (94%) hairdressers had been professionally active after vocational school. All interviewees answered questions about hand eczema, asthma, childhood eczema and any change of job. The wording of the questions was the same as in the postal questionnaire. Lack of time was the most common reason given for not returning the postal questionnaire.
Statistics
For statistical analysis, SAS V.8.2 was used. Age was stratified into categories of <25, 25–34 and >34 years. For the hairdressers, only periods of working as active hairdressers were included in the calculations. The incidence rates were calculated as the number of new cases of hand eczema per person-year of observation. Hairdressers without previous hand eczema were followed up from the year of certification, usually at the age of 18 years, and during years of working as hairdressers. The population controls were followed-up from the age of 18 years. Onset of hand eczema or 1996 (end of follow-up) were regarded as individual end points. Incidence rate ratios (IRRs) of hand eczema, with 95% confidence intervals (CIs), were estimated by Poisson regression using EGRET software. For comparison of proportions and that of means, the χ2 test and Student’s t test were used, respectively.
To establish whether a biological interaction (synergism) between childhood eczema and hairdressing exists, the relative excess risk due to interaction (RERI) was calculated. A model with two dichotomous risk factors was used, giving four possible combinations (exposure categories), the fourth serving as a reference category.11 Accordingly, if i = 1 the first risk factor is present and 0 otherwise, and if j = 1 the second risk factor is present and 0 otherwise; furthermore, if RRij is the age-adjusted relative risk in exposure category i,j, and thus RR11, RR10, RR01 and RR00 are the age-adjusted relative risks for each of the four categories (ie, RR11 = hairdressers with childhood eczema; RR10 = hairdressers without childhood eczema; RR01 = controls with childhood eczema; and RR00 = the reference category – (ie, population controls without childhood eczema = 1), then RERI = RR11−RR10−RR01 + 1.12 The CI was calculated according to Hosmer and Lemeshow.13
The attributable fraction (AF) of hand eczema from skin atopy—that is, the proportion of hand eczema cases attributable to childhood eczema, was calculated as follows:
AF = pc×(IRR−1)/IRR
where pc is the prevalence of childhood eczema among the cases of hand eczema and IRR is the age-adjusted IRR of hand eczema for hairdressers with childhood eczema compared with those without. The CI was established for ln(1−AF), where ln is the natural logarithm.14
RESULTS
Occurrence of hand eczema
Table 2 shows the incidence rate of self-reported hand eczema. The incidence rate observed for the hairdressers was 23.8 cases/1000 person-years compared with 9.6 for the controls. For hairdressers who at the time of the study were aged <25 years, the incidence rate of hand eczema was even higher. Table 2 shows the IRRs. A comparison between hairdressers and controls gives an IRR of 2.5 (95% CI 2.2 to 2.8). The IRR for hairdressers aged <25 years was significantly higher than that for older hairdressers.
Incidence rates (cases/1000 person-years) of hand eczema in hairdressers and controls in relation to age
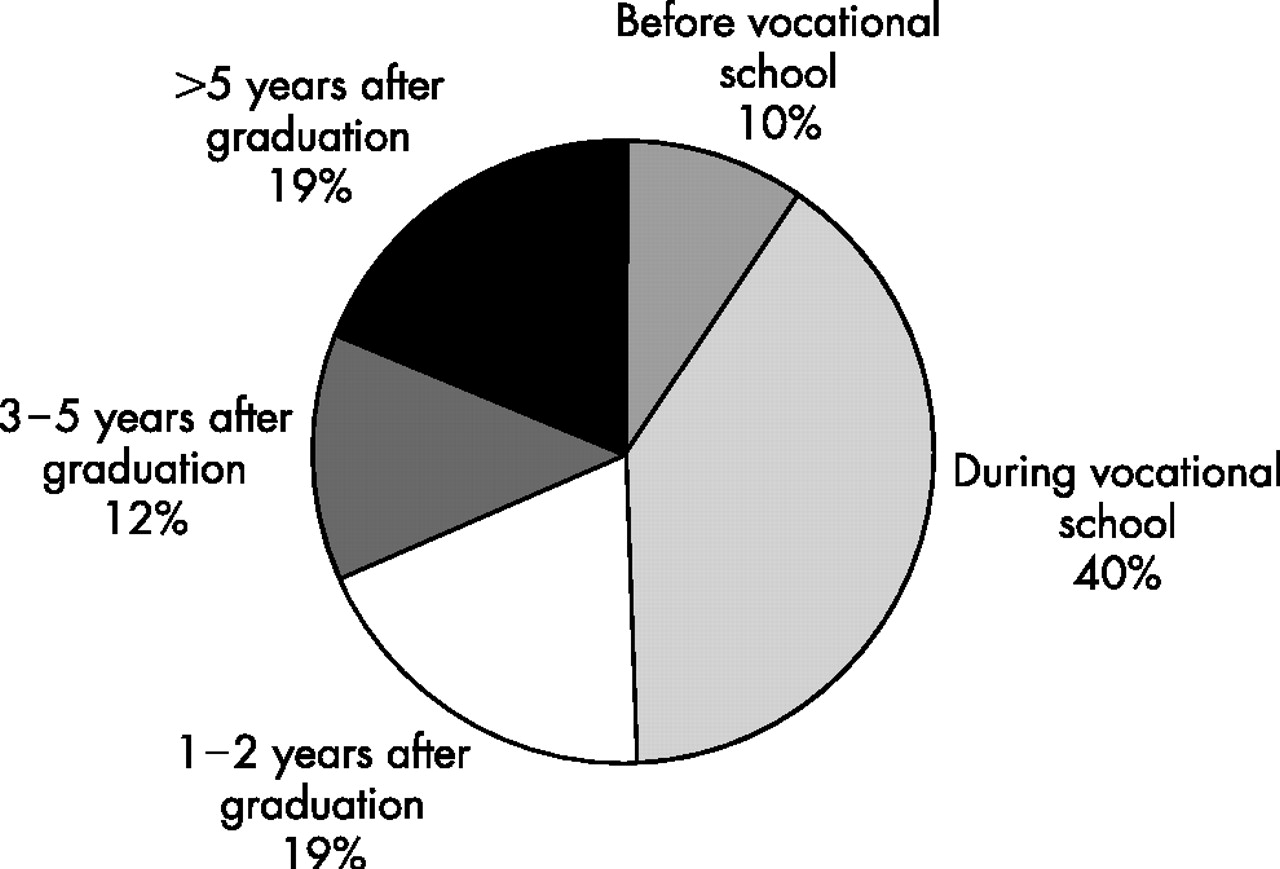
The mean age at onset of hand eczema was 21.6 (median = 20) years for hairdressers, and 21.2 (median = 21) years for the population controls. Figure 1 shows the onset of hand eczema among the hairdressers. In all, 40% of the hairdressers reported that their hand eczema had started during the period at vocational school.

{kind=link}
The proportion of hairdressers who reported onset of hand eczema during different time periods.
Table 1 shows the cumulative lifetime prevalence and 1-year prevalence of self-reported hand eczema among hairdressers and controls. Prevalences were significantly higher among the hairdressers. The 1-year prevalence in hairdressers was 18%. Among both hairdressers and controls with hand eczema during the previous 12 months, 54% stated that a physician had diagnosed the disease. Of the hairdressers who were or had been smokers, 31% had ever had hand eczema, compared with 27% of those who had never smoked (p = 0.017). Among the controls, the corresponding figures were 20% v 18% (p = 0.054).
History of atopy
Table 1 shows the anamnestic data on childhood eczema. A significantly lower proportion of hairdressers reported childhood eczema than controls. Both for hairdressers and controls, the incidence rate of hand eczema was higher among individuals with a history of childhood eczema, giving an (age-adjusted) IRR of 1.9 and 2.2, respectively (table 3). The RERI was calculated as 1.21 (95% CI 0.21 to 2.21; p = 0.01). The AF of hand eczema from skin atopy was 9.6% (95% CI 5.7 to 13.4).
Incidence rates (cases/1000 person-years) of hand eczema in hairdressers and controls in relation to history of childhood eczema
For hairdressers reporting childhood eczema, the mean age at onset of hand eczema was 18.8 years, whereas for controls who had had eczema during childhood it was 15.8 years (p<0.001). For 66% of the hairdressers reporting childhood eczema, the hand eczema had started before 21 years of age, compared with 46% among those without childhood eczema (p<0.001). For the controls, the corresponding figures were 67% v 29% (p<0.001). Among those with onset of hand eczema during the period at vocational school, a total of 28% reported childhood eczema.
Exposure and skin protection
Table 4 shows the self-reported number of hair treatments per week and use of protective gloves during current employment. For alkaline permanent waving, hair colouring and bleaching, between two and seven treatments per week was most common. A total of 58% of hairdressers stated that they performed shampooing >30 times a week. During colouring and bleaching glove use was most frequent, but during permanent waving and shampooing, gloves were used rarely. Of the glove users, 64% reported using polyvinyl chloride gloves, 50% used natural rubber latex gloves and 4% did not know the glove material (more than one answer possible). As many as 65% reported discolouration of the hands as a reason for using gloves, whereas 72% gave prevention and 19% gave alleviation of skin problems as the reason (more than one answer possible). Whereas 64% reported use of hand cream one to three times a day, 18% used cream more than four times a day and 18% never used hand cream. In all, 73% stated that they wore rings or bracelets while working.
Self-reported number of hair treatments per week and glove use during current employment
Change of job
Change of job due to hand eczema was reported almost three times more often by the hairdressers than by the controls (table 1). Of the hairdressers who reported ever having had hand eczema, 20% stated that they had changed jobs due to hand eczema (not shown in table 1). Among the 396 hairdressers who had never worked in the occupation after completing their training, 74 (19%) reported hand eczema as the reason. Therefore, 2% of all 4061 individuals never started working as hairdressers after school because of skin problems (74/4061). Of these, 27% (20/73) had a history of childhood eczema.
Non-responders
No statistically significant differences were found between responders to the mail questionnaire and participants in the telephone interview with regard to prevalence of hand eczema, childhood eczema and change of job for hairdressers and population controls.
DISCUSSION
A remarkably high incidence rate of hand eczema among hairdressers was found in this retrospective cohort study, in which about every fifth hairdresser in Sweden participated. The results confirm that hairdressing is a high-risk occupation for hand eczema, with extensive exposure to skin irritants and sensitisers.
An interesting observation is that the age of onset of hand eczema was ⩽20 years for about half of the hairdressers, and also for the controls. For 40% of the hairdressers, onset of hand eczema occurred during vocational training (fig 1). In other studies, a high prevalence and a high incidence rate of hand eczema were found among apprentice hairdressers.3–5 In two German studies, the risk was highest in the youngest age group.15,16 The explanation for early onset of hand eczema is probably that individuals with increased susceptibility, with as well as without skin atopy, develop hand eczema at an early stage when exposed to skin irritants and contact allergens.17
Many cases of occupational skin disease are probably not reported to the register of industrial injuries. In Sweden, only 5–10% of the hand eczema cases in hairdressers are reported. There is probably also some under-reporting to the registers in Germany and Denmark, as the reported incidence in these countries is considerably lower than what we found in this study.6,7
The high risk for hand eczema in hairdressers is in accordance with clinical experience. There are several studies showing that hairdressers have a high risk of developing occupational allergic contact dermatitis.18–21 In our study, we have no data on the occurrence of contact allergy among hairdressers. It was not feasible to perform patch testing because the hairdressers were scattered all over Sweden.
Childhood eczema results in a highly increased risk of developing hand eczema in adulthood.17,22–26 Brisman et al27 found that skin atopy increased the incidence of hand eczema among bakers by about threefold, and a synergistic effect of atopy and exposure was indicated. In our study, we found a twofold risk for hand eczema among hairdressers and controls with skin atopy. A statistically significant RERI was found, indicating a biological interaction between hairdressing and childhood eczema. Consequently, the sensitive skin among those with skin atopy in combination with the extensive exposure in hairdressing seems to have a synergistic effect on the occurrence of hand eczema.
The attributable fraction of hand eczema cases from skin atopy was 9.6%, indicating that only 1 in 10 hand eczema cases in hairdressers could be ascribed to atopy, and that the majority of cases are due to other factors. In a German study, 19% of occupational skin diseases among hairdressers could be ascribed to atopy.26 In our study, the prevalence of childhood eczema in hairdressers was lower than that in the general population. This implies a selection away from the hairdressing profession for those with skin atopy in agreement with another German study reporting lower prevalence of childhood eczema among hairdressers.16 The relative risk of developing hand eczema for hairdressers would therefore have been even higher if the incidence rates had been adjusted for atopy.
Change of jobs due to hand eczema was reported almost three times as often by the hairdressers as by the controls. One in five hairdressers who had ever had hand eczema had left the occupation because of the eczema. Half of the hairdressers and controls with hand eczema stated that a doctor had diagnosed the disease. This implies that the burden to society in terms of medical costs and possible compensation for income losses to the individual is of considerable proportion. In a Finnish self-administered questionnaire-based study, the risk of hairdressers having to leave their profession because of asthma or hand eczema was 3.5 times greater than found among the control group.28
Our results show that hairdressers perform a large number of different hair treatments, and that most of them are performed several times a week. To use protective gloves can be difficult during certain work tasks—for example during hair cutting. Glove use was reported to be low during permanent waving and shampooing, but higher during hair colouring and bleaching. Several studies show that dermatitis on the hands correlates with extensive daily exposure to occupational skin irritant factors.29 In one study on apprentice hairdressers, unprotected wet work in combination with <2 h/day of glove use gave a high risk for developing skin disorders.15
Smokers had a slightly higher prevalence of hand eczema, both among the hairdressers and among controls. There is little previous knowledge about whether there exists an association between smoking and hand eczema. Few studies have been published, with contradictory results.30–32
In this study, the postal questionnaire was sent to about one fifth of all active hairdressers in Sweden. Results from the analysis of non-responders showed that there was no difference between responders and non-responders regarding occurrence of hand eczema and childhood eczema, and that the results can therefore be considered representative. The questioning for the 1-year prevalence of hand eczema has been validated previously, and has shown to lead to some underestimation.33 However, using incidence rates gives a better understanding of the risk of developing hand eczema, considering the long duration of the disease.34 The question about childhood eczema has been validated previously.35
In conclusion, hairdressers are highly exposed to skin-damaging substances. The self-reported incidence of hand eczema in female hairdressers was substantially higher than that found previously in register-based studies, and also higher than that in controls from the general population. Onset of hand eczema often occurs early in life. Although the risk for hand eczema is increased in relation to history of childhood eczema, the attributable fraction from atopy is only about 10%. Measures to prevent the development of hand eczema among hairdressers should be given high priority.
Main messages
-
Female hairdressers are at high risk for hand eczema.
-
The number of hair treatments involving skin-damaging chemical exposure is high.
-
Skin atopy and hairdressing have a synergistic effect on the development of hand eczema.
-
In this study, the attributable risk of hand eczema from skin atopy in hairdressers was 9.6%.
-
For about half of the females with hand eczema, onset occurs before the age of 20 years.
Policy implications
-
Hairdressing is a high-risk occupation for hand eczema.
-
To prevent hand eczema in hairdressers, reduction of skin-damaging exposure is essential.
-
A history of childhood eczema increases the individual risk of hand eczema, but is not a major risk factor for hand eczema among hairdressers.
APPENDIX
QUESTIONNAIRE ITEMS REGARDING HAND ECZEMA AND SKIN ATOPY
Hand eczema:
Have you ever had hand eczema?*
Yes No
If yes:
What year did the hand eczema start?
19…….
Have you had hand eczema on any occasion during
the past 12 months?†
Yes No
Was your hand eczema diagnosed by a physician?
Yes No
Have you ever changed job because of hand eczema?
Yes No
Skin atopy:
Have you had childhood eczema?
Yes No
If yes:
Was this eczema sometimes on your hands?
Yes No
*Gives cumulative lifetime prevalence of hand eczema.
†Gives 1-year prevalence of hand eczema.
Acknowledgments
This study was funded by the Swedish Council for Work Life Research, the Vardal Foundation for Health Care Sciences and Allergy Research (2000–0074), the Swedish Council for Working Life and Social Research (2001–2399) and the Medical Faculty of Lund University. We thank Gunborg Lindahl, who assisted with collection of the cohort data and the data analysis, Karin Amilon and Ingrid Lindqvist, who interviewed the nonparticipants and Anders Holmén, who assisted in editing the questionnaire for scanning. We also thank Gudrun Persson, Gunnel Nilsson, Monica Hansi, Helena Brönmark and Ulrika Wallin, who handled the questionnaires, and Jonas Björk, who assisted in the calculations of the relative excess risk due to interaction and attributable fraction.
REFERENCES
Footnotes
-
Published Online First 19 October 2006
-
Competing interests: None declared.