Article Text

Abstract
Objectives: The French National Mesothelioma Surveillance Program (NMSP) was established in 1998 by the National Institute for Health Surveillance (InVS). Its objectives are to estimate the trends in mesothelioma incidence and the proportion attributable to occupational asbestos exposure, to help improve its pathology diagnosis, to assess its compensation as an occupational disease, and to contribute to research.
Methods: The NMSP records incident pleural tumours in 21 French districts that cover a population of approximately 16 million people (a quarter of the French population). A standardised procedure of pathological and clinical diagnosis ascertainment is used. Lifetime exposure to asbestos and to other factors (man made mineral fibres, ionising radiation, SV40 virus) is reconstructed, and a case-control study was also conducted. The proportion of mesothelioma compensated as an occupational disease was assessed.
Results: Depending on the hypothesis, the estimated number of incident cases in 1998 ranged from 660 to 761 (women: 127 to 146; men: 533 to 615). Among men, the industries with the highest risks of mesothelioma are construction and ship repair, asbestos industry, and manufacture of metal construction materials; the occupations at highest risk are plumbers, pipe-fitters, and sheet-metal workers. The attributable risk fraction for occupational asbestos exposure in men was 83.2% (95% CI 76.8 to 89.6). The initial pathologist’s diagnosis was confirmed in 67% of cases, ruled out in 13%, and left uncertain in the others; for half of the latter, the clinical findings supported a mesothelioma diagnosis. In all, 62% applied for designation of an occupational disease, and 91% of these were receiving workers’ compensation.
Conclusions: The NMSP is a large scale epidemiological surveillance system with several original aspects, providing important information to improve the knowledge of malignant pleural mesothelioma, such as monitoring the evolution of its incidence, of high risk occupations and economic sectors, and improving pathology techniques.
- pleural mesothelioma
- epidemiological surveillance
- occupational disease compensation
- France
Statistics from Altmetric.com
The massive development of asbestos use in industrialised countries was followed since the 1950s by a substantial and regular increase in the incidence of pleural mesothelioma.1 Occupational exposures are currently responsible for the vast majority of asbestos induced cancers in industrialised countries; other sources include environmental exposures of geological origin observed in some regions and the exposure of small populations of immediate neighbours of industrial asbestos manufacturers.2 Despite notable differences between studies, essentially because exposure assessment methods and frequencies of population exposure vary highly, it appears clear that in humans at least 80% of all pleural mesotheliomas in industrialised countries are due to occupational asbestos exposure.3,4
The most highly exposed occupations have changed over time. During the 1960s workers in industries involving asbestos mining, transformation, and use had the highest increases in the incidence of pleural mesothelioma,5 but since the 1980s, incidence of these cancers has increased most among workers involved in interventions to asbestos containing materials. These include construction workers in particular, but also other very diverse occupations.6,7
Some countries took measures long ago to reduce occupational asbestos exposure,8 and the increase in the incidence of and mortality from pleural mesothelioma has begun to slow down; the number of mesotheliomas is even diminishing in some countries.9–11 These trends are not homogeneous in all the industrialised countries, however. In France, for example, the frequency of pleural mesothelioma will probably continue to increase for at least two or three more decades, as shown by projections based on modelling of mesothelioma mortality.12,13
The National Mesothelioma Surveillance Program (NMSP) was established at the beginning of 1998 at the request of the French authorities. Responsibility for putting together qualified teams for each component of the programme and overall coordination were assigned to the occupational health department of the National Institute for Public Health Surveillance (DST-InVS).
The objectives of the NMSP are: to estimate the national incidence of mesothelioma in France and its course over time; to study the proportion of mesotheliomas in France attributable to asbestos exposure, especially of occupational origin; to contribute to research into other possible aetiological factors (man made mineral fibres, ionising radiation, SV40 virus, etc); and to help improve the pathological diagnosis of mesothelioma. As a study covering 1986–93 estimated that only 25% of patients with pleural mesothelioma in France received compensation for an occupational disease, and also showed important geographical disparities in compensation,14 one of the objectives of the NMSP is also to assess the extent of the recognition of pleural mesothelioma as a compensable occupational disease.
METHODS
The NMSP is organised into several components: (i) incidence monitoring; (ii) exposures and aetiology; (iii) pathology and clinical confirmation; and (iv) assessment of recognition as a compensable occupational disease. The DST-InVS coordinates the overall programme. An independent scientific committee was set up when the programme began.
Incidence monitoring
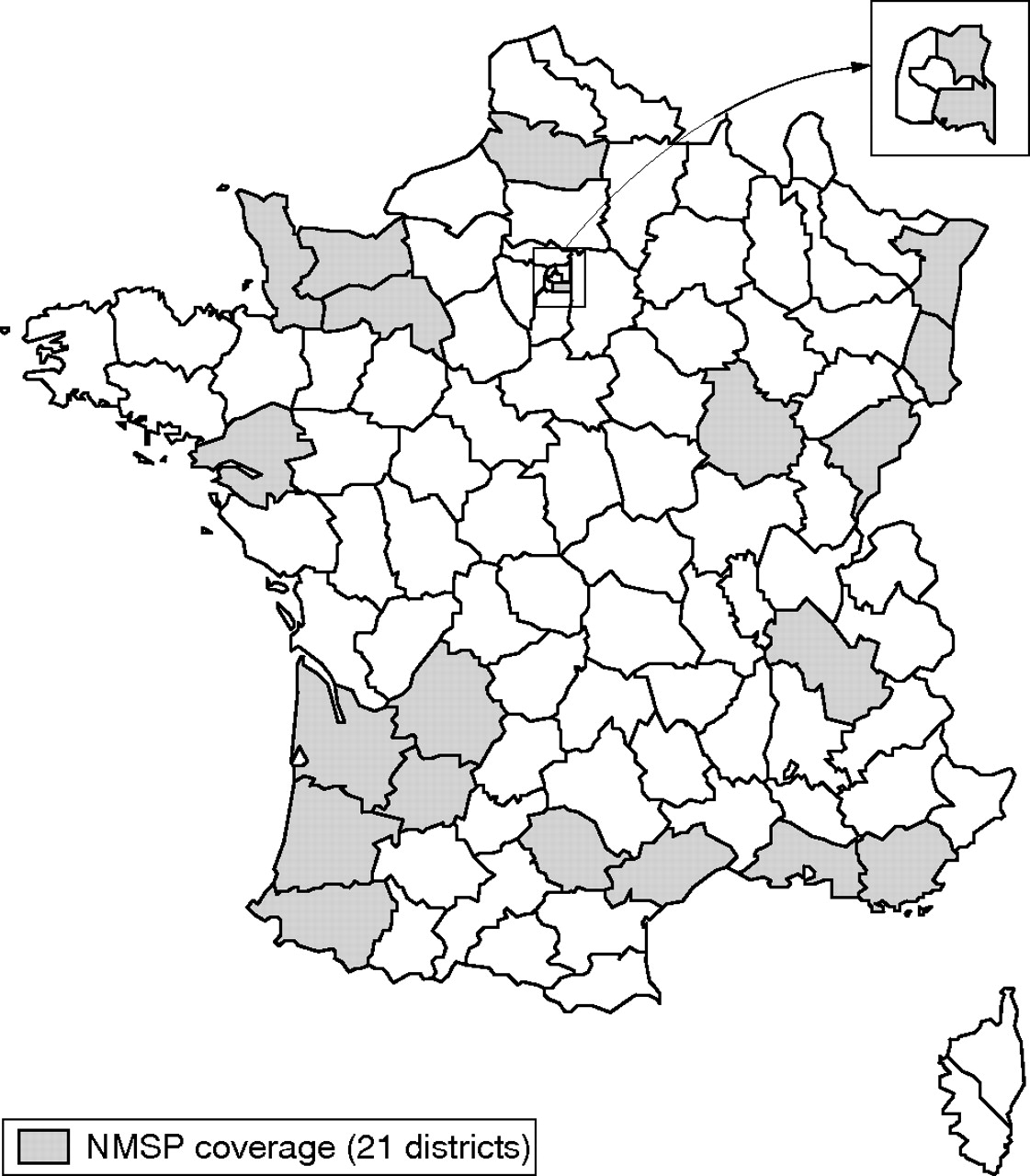
The NMSP relies on the exhaustive recording since 1998 of all incident primary pleural tumours in specified districts (for administration purposes, France is subdivided into 100 “departments” or districts). When the programme began it included 17 districts; coverage has since been extended and the NMSP currently includes 21 districts that cover a population of about 16 million, approximately one quarter of the 60 million inhabitants of France. These districts were chosen to be representative of France regarding the main demographic, employment, and economic activity characteristics. Figure 1 shows the geographical coverage of the NMSP and table 1 shows that the main basic characteristics of the population surveyed by the NMSP are almost similar to their distribution in France according to the 1999 census.15
Comparison between France and NMSP districts

Geographical area covered by the French National Mesothelioma Surveillance Program (21 districts, 16 million inhabitants).
Each district included in the programme has developed a procedure for identifying and reporting primary pleural tumours within a very short period after diagnosis. In 10 of the districts, a cancer register affiliated to the FRANCIM register network already existed and contributed to the NMSP. The procedure covers all of the specialised medical facilities likely to see these cases in order to improve the exhaustiveness of cases; ascertainment of the completeness of reporting in each district relies on the comparison of the numbers of registered cases and of death certificates with a pleural cancer or mesothelioma code. A standardised procedure of pathological and clinical confirmation of the diagnosis (described below) is applied to all cases reported.
Usually, national cancer incidence is estimated using projections based on modelling the evolution of registered cases and of mortality data.16 However, at that stage of the NMSP which began in 1998, it was not possible to use this technique. Thus the method used to estimate the national incidence of pleural mesothelioma was based on the estimated incidence/mortality ratio obtained by comparing the incidence and mortality data from the study districts. During the first two years of the NMSP (1998 and 1999), France still used the ICD-9 to code causes of death; since 2000, deaths are coded according to ICD-10. The incidence/mortality ratios observed for these districts are used to establish a global correction coefficient to the overall mortality figures in order to estimate the national annual incidence of pleural mesothelioma.
We intend to modify the methods we used to estimate the national incidence from the year 2000 onwards for two reasons: (i) it is planned that national incidence of all cancers will regularly be estimated in the future using projections based on modelling the evolution of cases registered by the FRANCIM network of cancer registers,16 using the mesothelioma cases from the NMSP districts which undergo a standardised diagnostic confirmation procedure to adjust the estimates; and (ii) we launched a specific sub-study for studying the impact of shifting from ICD-9 to ICD-10 and the coherence of death certificates with incidence data by matching the cases included in the NMSP to individual death certificates, and conversely by revising cases coded as mesothelioma on the death certificate and who were not registered in the NMSP.
Exposure and aetiology
Trained investigators interview each reported case. Using a standardised questionnaire, they collect information directly from the subjects during a face-to-face interview; when the subject has died, a family member or friend is interviewed according to a shorter questionnaire. The interview makes it possible to reconstruct the subjects’ lives: all the homes they lived in, all the schools they attended, their detailed job history including the tasks performed during each job, as well as their home repairs and do-it-yourself handiwork. The questionnaire also asks about other situations during the subject’s lifetime that may have involved exposure to asbestos or other possible aetiological factors. Each questionnaire is then analysed by industrial and environmental hygiene experts to assess the probability, intensity, frequency, and duration of exposure to each aetiological factor.
From 1998 to 2002, a population based case-control study intended to analyse the risk of pleural mesothelioma associated with exposure to asbestos, man-made mineral fibres, ionising radiation, and the SV40 virus was also conducted. For this study, two controls matched for age, sex, and district were selected from the general population by random drawing from voting rolls and interviewed according to the same questionnaire as the cases. Data analysis of the case-control study is underway.
Pathological and clinical ascertainment of diagnosis
Each case reported in the districts included in the NMSP undergoes a standardised diagnostic confirmation procedure. Samples (histological section or blocks) tested by the pathologist responsible for the initial diagnosis of the pleural tumour are transmitted to a national group of pathologists who specialise in mesothelioma, the national “Mesopath” panel. Three experts, blinded to asbestos exposure, classify each case as certain, uncertain (probable, possible), unclassifiable because of inadequate materials, or ruled out in favour of another diagnosis. When all three experts reach the same diagnosis, it is considered confirmed. Classification as an uncertain diagnosis corresponds either to a tumour definitely malignant, but not classifiable in the current state of pathology knowledge, or a lesion for which it is difficult to judge with the tools currently available whether it is benign or malignant. Otherwise, the case is reviewed collectively in consensus meetings involving at least 10 experts and confirmed, ruled out, or referred for clinical expertise.
The procedure of pathological diagnostic certification includes a supplemental immunohistochemical analysis to maximise the reliability of the diagnosis; this makes it possible to differentiate between pleural adenocarcinoma metastases and epithelioid mesothelioma, which are very similar and thus responsible for diagnostic errors. It can also distinguish sarcomatoid mesotheliomas from the primary sarcomas or metastases of sarcoma from extrapleural sites, which resemble them.
When the case cannot be confirmed pathologically, either because of diagnostic difficulties or because the samples were inadequate or not available, a clinical assessment is organised, based on questions to the attending physician and the patient’s records. If the physician does not respond or the documents are too incomplete, such an assessment is considered impossible. When the record is considered sufficient, two pneumoconiosis specialists independently assess it. The assessment is considered conclusive only when they agree. Cases are classified into three categories: very likely mesothelioma diagnosis, improbable mesothelioma diagnosis, and impossible to determine.
Recognition of pleural mesothelioma as a compensable occupational disease
In 18 of the 21 NMSP districts, we compiled a list of the mesothelioma cases of workers who belonged to the General National Health Insurance fund (organisation that also covers workers’ compensation for more than 80% of the French population) diagnosed between 1 January 1999 and 31 December 2001 and not excluded by the pathology confirmation procedure. The following data were collected: membership in General National Health Insurance fund; declaration of occupational disease, and its date; response by the General National Health Insurance fund and date; and reasons for refusal. The proportion of patients eligible for compensable occupational diseases from the General Fund and the proportion of subjects who did not apply for compensation were compared for the districts with sufficient mesothelioma cases (n ⩾30).
The French National Commission for Information Processing & Civil Liberties approved the procedures used by the NMSP.
RESULTS
Since the NMSP began, numerous analyses were conducted for surveillance purposes and to provide information for the public and for health authorities. Here, we summarise several results from each component of the programme, including some already published,17–21 to illustrate the contribution of the NMSP to epidemiological surveillance and research.
Incidence
By the end of 2003, approximately 1150 cases had been reported, 770 of which had been confirmed by pathological criteria. A first estimate of the national incidence for 1998 and 1999 was based on data from the 17 districts initially included (an 18th district was included in 1999). There was some interdistrict heterogeneity in the incidence/mortality ratio for pleural cancer (ICD-9 163): two of 17 districts in 1998 and three of 18 districts in 1999 showed a ratio equal or lower to 0.33, suggesting under-reporting. We thus considered two different scenarios to estimate the global correction coefficient to be applied to the national pleural cancer mortality figures: (1) using data from all the districts, assuming that recording was exhaustive in all districts; and (2) exclusion of districts for which the incidence/mortality ratio was less than a given threshold in order to exclude the districts where under-recording appeared likely; this threshold was arbitrarily set at 0.33, allowing us to keep as much information as possible while excluding the most extreme districts. Thereafter the calculation of incidence/mortality ratios to be applied to the national mortality data was conducted for each of the districts considered in both scenarios, by sex, age group, and year, and mean global ratios were computed. The first set of calculations considered only the cases classified as confirmed according to the pathology confirmation procedures; a second set also included the cases classified as probable or possible (according to the pathology confirmation) or very likely (according to the clinical confirmation). Finally, we applied the average global incidence/mortality ratios, by age group, and separately for men and women, to the numbers of deaths coded ICD-9 163 in France to obtain an estimate of the national incidence of mesothelioma.
The mean age at diagnosis was 69 years (median 70 years) in women and 70 years (median 72 years) in men. All subjects were older than 45 years at diagnosis except for one woman aged 30 years. According to scenario 1, the estimated number of incident cases in France for 1998 ranges from 127 when considering only the definite cases, to 146 (definite, probable, and possible) in women, and from 533 to 615 in men, that is, overall, from 660 to 761. Using scenario 2 increased the estimated incidence: for 1998, the estimate obtained from all the cases (confirmed, probable, and possible) increased by 2% in men and 24% in women. The crude incidence rate per 100 000 ranges from 1.8 (confirmed cases; all districts) to 2.3 (confirmed, probable, and possible cases; districts where the incidence/mortality ratio was at least 0.33) in men and 0.4–0.54 in women.17
The estimated number of incident cases of pleural mesothelioma in 1999 is close to that for 1998 and ranges between 600 and 808. Overall, these results are close to the estimate (750 cases in 1996) made by the INSERM expert advisory panel,2 and lower than incidence estimates for 2000 based on modelling of the data of the FRANCIM network of cancer registers,16 the difference being mainly due to the fact that more than 10% of the cases regularly registered were excluded by the NMSP diagnosis ascertainment procedure.
Exposures and aetiology
At the end of 2003, 470 living cases (377 men and 93 women) and 820 controls (679 men and 141 women) were interviewed, and 124 interviews conducted of family or friends of cases who could not be personally interviewed. A full analysis of the case-control study is currently underway, but several partial results for the living men for whom we have complete data are already available.
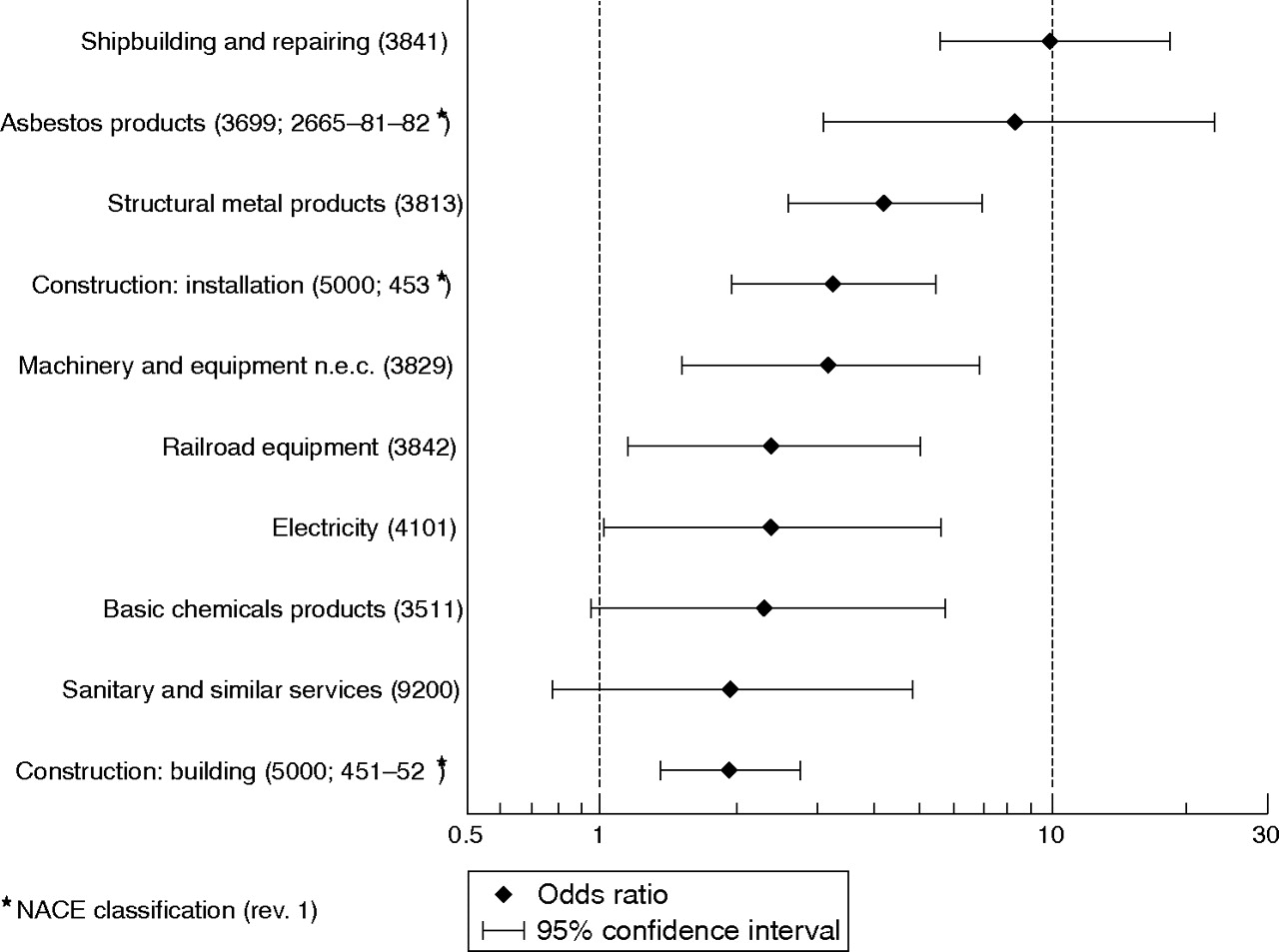
A descriptive analysis examined the industries and occupations at high risk for mesothelioma; it compared subjects who had at least once in their career been employed in a given industry or occupation with those who never had been. An odds ratio (OR) and its 95% confidence interval (95% CI) were thus calculated for each industry and each occupation (with at least 20 cases and controls). The industries where the risks of mesothelioma were highest were construction and ship repair, transformation and manufacture of asbestos products, and the manufacture of metal construction materials (bridges, tanks, pipes, scaffolding, and staircases). The occupations most at risk were plumbers and pipe-fitters, sheet metal workers and boilermakers, and welders and flame-cutters.18Figures 2 and 3 summarise these results.

Pleural mesothelioma among men in France: industry specific odds ratios (ISIC classification, rev. 2) (377 cases and 679 controls).

{kind=link}
{kind=link}
{kind=link}
Pleural mesothelioma among men in France: occupation specific odds ratios (ISCO classification, 1968) (377 cases and 679 controls).
We also calculated the risk fraction attributable to occupational asbestos exposure: it was estimated at 83.2% (95% CI 76.8 to 89.6) in men, and 38.4% (95% CI 26.8 to 50.0) in women.
Diagnostic confirmation
Pathological review confirmed the initial pathologist’s diagnosis in 67% of cases and definitely ruled it out in 13%. The diagnosis remains uncertain (no reliable element allowing a definitive decision either way) in approximately 17% of cases (3% of the files are still in the process of certification). The cases with uncertain diagnoses underwent clinical expert assessment when the medical record was sufficiently complete (75% of the uncertain cases). Among them, 49% concluded by a judgement strongly supporting a mesothelioma diagnosis, 36% that there was little evidence of such a diagnosis, while no conclusion was possible for 15%.
Analysis of the histological variants showed mostly epithelioid mesothelioma (approximately 70%). The mixed form was observed in approximately 15% of the cases and the sarcomatoid form in 11%; the desmoplastic form accounts for less than 2% of the latter.
Since the NMSP began in 1998, numerous markers have been marketed for mesothelioma diagnosis, which has improved the quality of the results. For example, the number of epithelioid mesotheliomas increased in 2000 (after the introduction of calretinin, a positive marker for mesothelial cells) and in 2002 (after the introduction of TTF-1, a very specific positive marker for pulmonary adenocarcinoma).
The specificity and sensitivity of negative and positive markers for mesothelial cells with epithelial characteristics were assessed. The combination of one negative marker and two positive markers for mesothelial cells provides a specificity of 100% without overly reducing the sensitivity (79.9%).19 The use of molecular markers will probably make it possible in the future to resolve some questions that are still unclear today (preneoplastic conditions, early neoplasms, unclassified tumours).
We also assessed survival according to histological type. The study included 103 certified mesotheliomas for which exposure status and survival were known. Analysis showed that survival was best in subjects who were younger (p < 0.05) and in unexposed patients (p < 0.05). It was also best in those whose histological form was epithelioid, compared with mixed, and worst in sarcomatoid forms (p < 0.01).
The thorough certification procedure for pathological diagnosis implemented for NMSP (combination of morphological analysis and exhaustive immunohistochemistry) was especially useful in showing unusual histological forms in 15% of cases. Trend analysis showed a regular increase in the reports of these unusual variants, which were rarely if ever identified before 1998, and therefore major sources of diagnostic errors (6% in 1998, 8% in 1999, 14% in 2000, 15% in 2001, 19% in 2002). Among these unusual variants, we identified a series of 24 well differentiated superficial papillary mesotheliomas, a new entity characterised by development of proliferation on the surface of the pleura without infiltration of the deep underlying structures and by a slow course leading to long survival, ranging from 42.7 months to 74 months, with a mean survival time of 48.5 months.20
Recognition as a compensable occupational disease
This study covered the 1999–2001 period. During these three years, 449 cases were recorded in the 18 districts covered by NMSP and not subsequently excluded by the diagnostic confirmation procedure; 68% of these cases were covered by the General National Health Insurance fund. Only 62% of these subjects sought recognition for an occupational disease, and it was granted for nearly all (91%). The refusals (8% of the subjects) were all explained by failure to meet the administrative criteria for recognition. The outcome of the request was unknown for 1% of the subjects. Of the 38% of subjects who did not make this request, 39% were considered asbestos exposed, and 25% unexposed; because the exposure assessment were not performed at the time of this specific study, there was no exposure data available for 36%.
The proportion of subjects who did not make the request varied significantly by district, ranging from 13% to 46% (p < 0.01). This proportion was not associated with occupational exposure to asbestos and seems to be explained mainly by the physicians’ sensitisation to the issue, and/or the patient’s decision (to claim for compensation or not) which varied by region.21
DISCUSSION
The NMSP, which covers approximately 16 million inhabitants, or one quarter of the French population, is an epidemiological surveillance system intended to provide permanent information of the trends and course of the mesothelioma epidemic, which will continue to develop in France for at least two or three more decades.12,13 It provides important data to improve the knowledge of mesothelioma and allows monitoring of numerous aspects of this disease on a large scale.
National epidemiological surveillance systems for mesothelioma exist in several other countries, including Australia22 and Italy.23 The French NMSP nonetheless presents several original aspects. To our knowledge, the procedure of standardised and centralised pathological and clinical certification, systematic for all possible cases, is unique in the framework of such an epidemiological surveillance system. The NMSP also included a case-control survey to study risk factors associated with this tumour. The systematic analysis of its compensation as an occupational disease, while specific to the French situation, also sheds a different light on the phenomena of under-compensation found in other countries.24
Although the exploitation of the data brought together here has barely begun, in particular because of the long time gap between the occurrence of cases and the point when all the data have been collected and validated, the NMSP has already furnished useful information about the mesothelioma epidemic in France. The collection of data from the first five years will be completed shortly, and more detailed analyses will begin.
Main messages
-
The French National Mesothelioma Surveillance Program (NMSP) was established in 1998. The NMSP records all pleural mesothelioma in a large geographical area; it covers approximately 16 million people (more than one quarter of the inhabitants of France).
-
Each case reported in the NMSP undergoes a standardised pathological and clinical diagnostic confirmation procedure when the pathological conclusion is uncertain.
-
Each case registered undergoes a complete assessment of exposure to asbestos and other potential risk factors.
-
The NMSP provides accurate estimates of the incidence of pleural mesothelioma in France.
Policy implications
The French National Mesothelioma Surveillance Program (NMSP):
-
Estimates the trends in pleural mesothelioma incidence in France.
-
Estimates the proportion of these tumours attributable to occupational asbestos exposure.
-
Contributes to the research for other aetiological factors.
-
Improves the pathology diagnosis of pleural mesothelioma.
-
Assesses the recognition of pleural mesothelioma as a compensable occupational disease.
Acknowledgments
The authors thank the Scientific Committee (P Boffetta (chairman), E Chailleux, J Estève, J Faivre, and D Hémon), the directors and investigators of the registries, Marie Arslan, and Danièle Luce for her careful reading of the manuscript.
REFERENCES
Footnotes
-
Published Online First 9 February 2006
-
Funding: NMSP has received financial support from the National Institute for Health Surveillance (InVS), the Ministry of Labour, and the Ministry of Health. It also received financial support from the Foundation for Medical Research.
-
Competing interest: none