Article Text

Abstract
Background: There is widespread public concern that exposure to road vehicle traffic pollution causes asthma, but epidemiological studies in developed countries have not generally confirmed a strong effect and may have underestimated the risk as a result of relatively high and widespread exposure to traffic in everyday life.
Aims: To investigate the effect of living close to a traffic bearing road on the risk of wheezing in Jimma, Ethiopia where road traffic is generally low and restricted to a limited network of roads.
Methods: Data have been previously collected on respiratory symptoms, allergic sensitisation, and numerous demographic and lifestyle factors in a systematic sample of inhabitants of Jimma town. In 2003 the homes of these people were retraced; the shortest distance to the nearest surfaced road, and traffic flows on these roads were measured.
Results: Distance measurements were collected for 7609 (80%) individuals. The overall prevalence of wheeze was similar in those living within 150 m of a road compared to those living further away (3.9% v 3.7%), but among the 3592 individuals living within 150 m, the risk of wheeze increased significantly in linear relation to proximity to the road (adjusted odds ratio = 1.17 per 30 m proximity, 95% CI 1.01 to 1.36). This relation was stronger, though not significantly so, for roads with above median traffic flows.
Conclusion: These findings indicate that living in close proximity to road vehicle traffic is associated with an increased risk of wheeze, but that other environmental factors are also likely to be important.
- CI, confidence interval
- OR, odds ratio
- air pollution
- wheezing
- asthma
- vehicle emissions
Statistics from Altmetric.com
There is widespread public concern that living close to a main road and the consequent exposure to road vehicle traffic pollution causes asthma. In developed countries, several studies have shown an increase in asthma risk in people who live close to a main or busy road,1–10 but the magnitude of the effect is modest and the evidence far from consistent, with a number of studies reporting no evidence of increased risk.11–15 It is possible that these studies have underestimated the true effect because everyday exposure to relatively high levels of road traffic pollution is so widespread in developed countries, and hence misclassification of exposure likely. Conversely, estimates of risk may be inflated by reporting bias arising from the public perception that traffic is a cause of asthma. It is therefore important to investigate this effect in populations where these biases are less likely to apply.
Jimma in Ethiopia is an urban community at a relatively early stage of economic development, with generally very low levels of road vehicle traffic restricted to a limited network of surfaced roads. Jimma also has no major industry contributing to air pollution, and the prevalence of asthma in the general population, and awareness of road traffic pollution as a potential cause of asthma, is relatively low. We have therefore used data from a previous survey of asthma symptoms in Jimma,16 linked to measurements of the distance between homes and the nearest surfaced road, to investigate the relation between road traffic pollution and asthma risk at relatively low levels of vehicle traffic flow.
METHODS
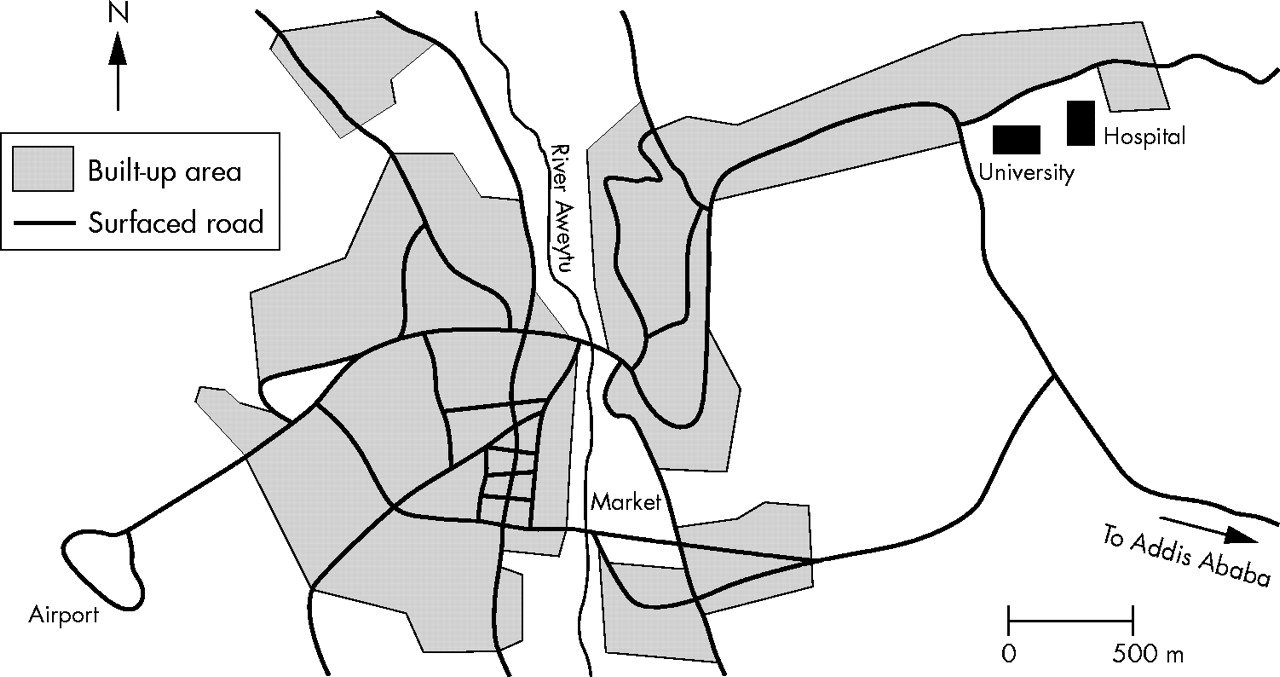
In 1996 we surveyed respiratory symptoms, allergic disease, and demographic and lifestyle factors for 9844 children and adults living in a systematic sample of 2025 households in 21 administrative districts in the urban area of Jimma in Ethiopia, and measured allergen skin sensitisation to Dermatophagoides pteronyssinus in a one-in-four subsample, as previously described.16 In spring 2003 we retraced these homes and measured the shortest distance between the home and the nearest surfaced road using a measuring wheel (Trumeter Company Ltd, Manchester, UK). The road structure in Jimma town, which is almost completely unchanged since 1996, is shown in fig 1. Vehicle pollutant concentrations in developed countries fall exponentially with distance from the road, reaching background levels within 150 m,17 and we have assumed a similar dispersion pattern in this population. Therefore we did not measure distances estimated to be more than 200 m, and we excluded all 64 households (264 participants) from one district with no surfaced roads within 200 m. We measured traffic flows on surfaced roads by counting all vehicles passing between 6 am and 6 pm on two separate days, one market day and one non-market day, and taking the average of these for analysis. This is because markets are the primary factor affecting traffic in Jimma, with more traffic on the three market days than the three weekday “non-market” days, and very little traffic on a Sunday. A variable representing average flow for diesel vehicles only was computed in the same way. Ethics approval for the study was granted by the Jimma Institute of Health Sciences and Nottingham City Hospital Ethics Committees.

Map of road network in Jimma town (adapted from Ethiopian Mapping Agency map of Jimma; series ETH 4, sheet 0736 B4).
We used multiple logistic regression (STATA version 8.0, Stata Corporation, Texas, USA) to estimate odds ratios (OR) (with 95% confidence intervals (CI) adjusted for clustering by household) for self-reported wheeze in the past year, and the secondary outcomes self-reported rhinitis and eczema symptoms and sensitisation to D pteronyssinus (defined as a mean wheal diameter of at least 3 mm greater than the saline control), in relation to distance from the nearest surfaced road. Wheeze in the past year is a commonly used and accepted marker of asthma which was chosen in this study because of concerns about the reliability of a diagnosis of asthma. Distance was initially examined as a binary variable representing 150 m or less, and greater than 150 m. To explore the nature of any exposure-response relation within 150 m of the roadside, distance was categorised into 30 m bands and treated as a factor. The fit of this model was compared with that fitting a trend through the categories using the likelihood ratio test, and if the two models were not significantly different, linearity was assumed. If linearity was shown, odds ratios were computed using the original continuous distance variable. All estimates were adjusted for confounding by age, sex, socioeconomic status (based on ownership of goods), smoking status, and kerosene use, a previously identified risk factor for allergic disease in this population,18 and all p values presented are two sided. To investigate any modifying effect of traffic flow density we stratified the analysis by level of traffic flow (above and below median flow). Similarly, we stratified by age group (<16 years and 16+ years) to explore whether the relation differed between children and adults.
Main messages
-
Results suggest an adverse effect of living in close proximity to road traffic on asthma risk, even when levels of traffic are significantly lower than in the Western world.
-
Among people living within 150 m from a road, where the primary traffic related pollutants are known to be increased, the risk of wheeze increased with increasing proximity to a road.
-
The prevalence of wheeze in those living away from roads (>150 m) was not as low as expected, suggesting some other environmental factor(s) may be playing an important role in asthma aetiology in this population.
RESULTS
We successfully retraced the homes of 7609 (80%) of the 9550 eligible individuals studied in 1996. Of the 1941 individuals not retraced, the homes of 58 had since been demolished and those of 1883 could not be relocated because they were not numbered or otherwise identifiable. The characteristics of the 7609 study subjects are shown in table 1, and with the exception of socioeconomic status, these did not differ from the characteristics of the subjects who were not successfully traced.
Characteristics of study subjects and comparison with subjects from original sample who were not retraced
Policy implications
-
Further research is warranted in countries where exposure to traffic pollution remains low and is not yet widespread in order to fully quantify the effect of traffic pollution on asthma risk.
The prevalence of wheeze was not significantly greater for those living within 150 m of a surfaced road compared with those living more than 150 m away (3.9% and 3.7% respectively; adjusted OR = 1.03, 95% CI 0.79 to 1.34, p = 0.82). However, among the 3592 individuals who lived within 150 m of a surfaced road, the risk of wheeze increased significantly in linear relation to proximity to the road (fig 2; adjusted p value for trend = 0.048). Since there was no evidence of departure from linearity in this relation (likelihood ratio test, p = 0.76), distance was fitted as a continuous variable and the adjusted OR per 30 m proximity estimated at 1.17 (95% CI 1.01 to 1.36, p = 0.03; table 2). Control for other potential confounders (including vaccinations, bedding and housing variables, older siblings, use of biomass and other fuels, level of current smoking, occupation, and educational level) had little effect on the magnitude or significance of these odds ratios. When children and adults were considered separately, the estimated magnitude of effect was slightly highly in children than adults (table 2) but there was no statistically significant interaction.
Odds ratios for wheeze in relation to proximity to nearest road for subjects living within 150 m of a surfaced road, stratified by age group and traffic flow

{kind=link}
{kind=link}
Odds ratios and 95% CIs for wheeze in relation to proximity to nearest surfaced road in Jimma. Odds ratios adjusted for age, gender, socioeconomic status, smoking status, and kerosene use. p value for trend through 30 m categories = 0.048.
Traffic flows measured on 71 surfaced roads ranged from 37 to 2640 vehicles (median 653) over 12 hours, with flows for diesel vehicles ranging from 17 to 750 (median 212). Level of traffic flow on the nearest road was itself unrelated to an individual’s risk of wheeze, both in the whole population and among those living within 150 m of a road, but did appear to modify the relation between proximity and wheeze. The effect of proximity on wheeze was seen to be stronger for those living within 150 m of an above median flow road (adjusted OR per 30 m proximity = 1.26, p = 0.02) than those living near low flow roads (OR = 1.08, p = 0.50; table 2), and similar findings were seen when associations were stratified by diesel traffic flow (adjusted OR per 30 m proximity = 1.24 and 1.12 for above and below median flow roads respectively). These interactions, however, were not statistically significant.
Results for rhinitis and eczema symptoms were similar to wheeze; both showed no relation with distance overall as a binary variable, but within 150 m showed a positive, though non-significant relation with proximity to road (adjusted OR per 30 m proximity = 1.14, 95% CI 0.97 to 1.33, and OR = 1.19, 95% CI 0.93 to 1.53, respectively). In the 1721 subjects with skin sensitisation data, living within 150 m of a road was associated with a borderline significant increased risk of sensitisation to D pteronyssinus (adjusted OR = 1.76, 95% CI 0.98 to 3.15, p = 0.06). Among those living within 150 m of a road, the risk of sensitisation increased with increasing proximity but the relation was not statistically significant (adjusted OR per 30 m proximity = 1.10, 95% CI 0.82 to 1.46).
DISCUSSION
This study shows an exposure-response relation between proximity of residence to a surfaced road and the risk of wheeze in the past year among adults and children living within 150 m from a road. This corresponds to an estimated doubling of risk for those living immediately adjacent to a road compared to those living 150 m away. This effect appears to be greater for relatively busy roads (at least 55 vehicles per hour).
Distance between the home and the nearest surfaced road is a proxy marker of exposure to traffic pollution, and personal exposure will additionally depend on such things as time spent near the home and meteorological factors, including wind direction. However, in this population our distance variable is likely to be a reasonably accurate estimate of individual exposure because traffic in Jimma is restricted to a rudimentary network of surfaced roads and individuals are less mobile than in developed countries. Hence exposure to traffic will occur primarily in those living close to roads and will generally be very low in those living away from these roads. Our findings are unlikely to be distorted by bias in reporting, since our information on wheeze was collected independently of exposure in an earlier survey, and exposure data were collected objectively by fieldworkers who were blind to disease status. Although exposure was measured some time after the original survey of symptoms, the road network in Jimma did not change in this period so relative exposure at the time of the traffic survey will be similar to that in 1996. Selection bias is also unlikely to be a problem as the original participation rate in the study was very high (over 95%), and while we were unable to obtain an exposure measure in 2003 for 20% of subjects, this proportion was similar for wheezers and non-wheezers. Failure to retrace a home was primarily due to poor numbering on houses which is likely to be more of a problem for the lower quality housing structures, and may explain the socioeconomic difference between the original sample and those retraced. This slight over-representation of the socially advantaged in the analysis could bias the results if these individuals are more likely to be wheezers who live near a road. However wheezing was unrelated to socioeconomic status in our original survey.16 While confounding by some unmeasured factor, such as diet or parasite infection, cannot be ruled out, we did try controlling for a wide range of other demographic and lifestyle factors, and associations with distance were seen to persist.
The nature and magnitude of the exposure-response relation observed in people living within 150 m of a road in this study is similar to that in secondary schoolchildren and primary school girls in our earlier study of wheeze in Nottingham schoolchildren.6 A recent study of US male veterans also examined the exposure-response relation using 50 m bands and saw an increased risk of persistent wheeze only for those living within 50 m of a major road (OR = 1.31 for all roads and 1.71 for roads with average daily traffic of at least 10 000 vehicles).8 Other previous studies that have measured distance have tended to use a single cut point and have reported an odds ratio of wheeze of 2 for children living within 100 m of a freeway,1 and odds ratios of chronic wheeze of 2.75 and 1.52 (two successive surveys) for women living within 20 m of a busy road, although no increased risk was seen in a third survey.7 Three other studies of asthma conducted in the UK have used a larger cut-off point (150 m or 200 m) and shown weaker, non-significant effects.11–13 A clear difference between the studies to date and the current study is the level of traffic on the roads, with average daily traffic flows between about 10 000 and 100 000 vehicles in the above studies compared to under 1000 (median 653 for 12 hour daylight period) in Jimma. This may explain why the size of effect seen in Jimma was no higher than previously reported despite the likely reduction in exposure measurement error.
The findings of this study suggest that even at a relatively early stage of urbanisation where levels of traffic are significantly lower than in the Western world, exposure to pollution arising from road vehicle traffic has an adverse effect on respiratory health. However the fact that overall risk of wheezing was similar in people living within 150 m from a road to those living further away, despite the absence of road vehicle pollution sources in the latter group, suggests that traffic pollution is not a major determinant of asthma risk in this population. Similar proportions of lifetime Jimma residents with and without current wheeze had ever moved home (33.6% and 30.1% respectively), suggesting that a tendency for asthmatics to move away from roads is not an explanation for the finding. However, clear lifestyle differences were observed between those living less than and greater than 150 m from a road, including fewer wealthy subjects (based on ownership of goods) in the distant group, and although none of the factors measured in this study altered the estimated difference in wheeze risk between these two groups, it may be that some other unmeasured environmental or lifestyle risk factors are influencing the risk of asthma in those areas away from roads.
A number of possible mechanisms have been proposed to explain the effect of traffic pollution on asthma, and these have been outlined extensively elsewhere.19 However, the fact that we observed associations of similar magnitude (although not significant) for rhinitis and eczema symptoms and skin sensitisation, and others have shown effects of traffic pollution on allergic outcomes,14,20 suggest that the effect may be general to all allergic disease rather than something specific to asthma. This finding also suggests that allergic asthma accounts for much of the wheeze reported in our study population. Some studies have suggested that exposure to diesel vehicles may be more strongly related to respiratory health than other traffic,1,3 and while we found no suggestion of this in our study, some error may have occurred in identifying diesel vehicles by the fieldworkers. Particulate matter has also been linked with adverse respiratory health,19 and may be of particular importance in this study as the relative proportion of roadside particulate pollution attributable to dust agitated by vehicle wheels may be higher than in developed countries.
In conclusion, these findings suggest that living in close proximity to road vehicle traffic increases the risk of wheeze, and possibly other allergic diseases, in both children and adults, but that other environmental risk factors are also likely to be contributing to the aetiology of asthma in this population.
Acknowledgments
We thank Zegeye Bekele for data entry in Jimma; the staff at Jimma University for their support; and the fieldworkers for their help in data collection.
REFERENCES
Footnotes
-
Funding: we thank the Wellcome Trust and the Association of Physicians of Great Britain and Ireland for financial support
-
Competing interests: none
Linked Articles
- Commentary