Article Text

Abstract
Aims: To develop a model of prognosis for time receiving workers’ compensation wage replacement benefits in the first year.
Methods: A prospective cohort of 907 injured workers off work because of soft tissue injuries was followed for one year through structured telephone interviews and administrative data sources. Workers were recruited at workers’ compensation claim registration. Only those still off work at four weeks post-registration were included in the analysis. Data from several domains (demographics, clinical factors, workplace factors, recovery expectations) were collected at approximately two weeks and a subset again at four weeks. Outcome was duration on total temporary wage replacement benefits. Variable selection was carried out in two steps using content experts and backward elimination with the Cox model.
Results: Body region specific functional status, change in pain, workplace offers of arrangements for return to work, and recovery expectations were independently predictive of time on benefits. Change in pain and workplace offers interacted, so the largest mutual association occurred for those whose pain was getting worse—that is, reduction in median duration from 112.5 to 32.5 days. Across observed values, widely different recovery profiles of groups of workers resulted; for example, at four months, only one third of the highest risk group had gone off benefits while over 95% of the lowest risk group had done so.
Conclusions: Focus on a relatively small set of prognostic factors should enable occupational health practitioners to triage injured workers within the first month and concentrate on those requiring additional assistance to return to work.
- prognosis
- musculoskeletal disease
- proportional hazards model
- occupational injury
- workers compensation
- cohort study
- OWSIB, Ontario Workplace Safety & Insurance Board
- RTW, return to work
- WMSD, work related musculoskeletal disorders
Statistics from Altmetric.com
- prognosis
- musculoskeletal disease
- proportional hazards model
- occupational injury
- workers compensation
- cohort study
- OWSIB, Ontario Workplace Safety & Insurance Board
- RTW, return to work
- WMSD, work related musculoskeletal disorders
Soft tissue injuries are a major cause of work related disability in industrialised countries. In North America, low back sprain and strain is typically the largest single category of lost-time claims to Workers’ Compensation Boards,1 and a recent study suggested that the numbers of claims and costs of work related musculoskeletal disorders (WMSD) of the upper limb are approaching those of low back pain.2 The majority of costs associated with these disorders are typically incurred by a small minority of claimants who remain off work (or on benefits) for long periods of time3,4; for instance, 7.4% of cases absent from work for six months in an inception cohort of occupational back pain claimants accounted for about 70% of lost days, medical costs, and wage replacement costs.3 Because of the economic burden incurred by these longer term cases, return to work and compensation costs are important outcomes for employers and compensation boards. Health care practitioners are interested in return to work (RTW) as a clinical outcome and injured workers are interested in reintegration into work. Occupational physicians must often work with multiple stakeholders to arrange RTW.
Early prognostic factors of return to work could be used to identify workers likely to recover quickly, therefore requiring minimal care or intervention, and to identify workers less likely to recover, therefore requiring more intensive medical and/or vocational interventions. The literature on prognostic factors is more extensive for low back pain than for other soft tissue injuries. There are several published studies from a variety of settings employing appropriate methodology5 to identify prognostic models for acute low back pain with work related outcomes.6–16 The published studies tend to be either of small to moderate sample size with a large number of clinical measures,6–8,12–15 or of large sample size with a small list of mostly administrative measures.17–22 However, two recently published studies involved fairly large samples of compensated workers accrued from either a clinical setting11 or a compensation setting,16 and the analysis incorporated a range of measures from physical examinations and/or questionnaires. On the other hand, for WMSD of the upper limb, there have been very few published studies of high methodological calibre to date.23
The study presented here makes a unique contribution in several ways. First, it covers a breadth of soft tissue conditions of the back, upper extremity, and lower extremity. Second, it is based on a large sample of workers. Third, the sample provides representativeness in that it was drawn from a workers’ compensation setting which covers 70% of the working population in the province. Fourth, it includes a broad range of clinical, workplace, and administrative factors measured on two occasions in the first four weeks of injury. Finally, it uses as the inception point four weeks post-injury, the end of the “acute” phase, which is considered a critical time for decision making around interventions for soft tissue injuries.24,25 The objective was to build a model of prognosis predicting length of time receiving workers’ compensation benefits using factors measured during the initial four weeks.
METHODS
Study design
The Ontario-wide cohort of injured workers with lost-time claims for soft tissue disorders was part of a larger programme evaluation,26 conducted in conjunction with the Ontario Workers’ Compensation Board (now Ontario Workplace Safety & Insurance Board or OWSIB). Since the OWSIB has the statutory authority to ask claimants about relevant issues in order to inform programme and policy development, the study protocol did not undergo external ethical review. However, all respondents were free to decline participation and were assured that participation status would not affect their access to OWSIB services. Further, confidentiality of their individual responses was guaranteed, with only aggregate data from analyses provided to the OWSIB. The sampling strategy, eligibility criteria, and participation rates are described in detail elsewhere.26
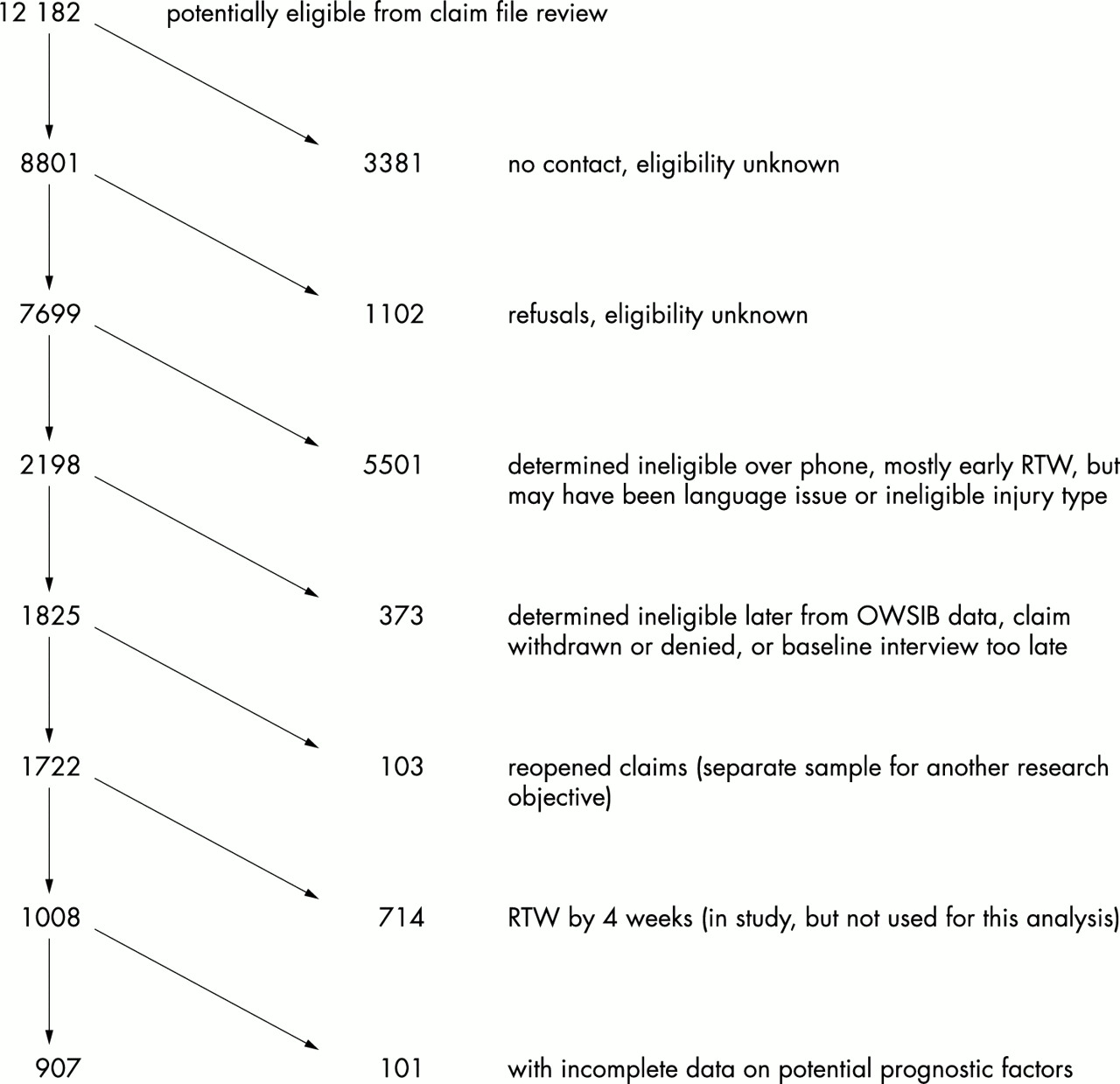
The cohort includes workers accrued from throughout the province of Ontario with new allowed lost-time claims for soft tissue injuries of the back, upper limb, or lower limb. Soft tissue injuries were clearly defined by inclusion and exclusion criteria,26 and included sprains and strains, inflammation of joints, tendons, or muscles, contusions, repetitive strain injuries, bursitis, synovitis, tenosynovitis, and tendinitis among the diagnoses applied. Accrual took place between May and November 1993, and only subjects first interviewed within 21 days of the onset of wage replacement benefits were eligible. Figure 1 shows the flow of potential participants from initial identification to final inclusion in the analysis presented here. Of the 3381 claimants who could not be contacted and the 1102 claimants who declined participation, 1218 were lost-time claimants with a soft tissue injury, with date of accident in the study accrual period, claim registration within two weeks of the accident date, and still on benefits four weeks post-accident, and therefore would have been eligible for this study. A comparison of the 907 in the study group with these 1218 claimants shows very similar characteristics in terms of the distribution of age (mean (SD) of study participants 38.6 (10.9) versus non-participants 38.8 (11.0)), sex (participants 49% male, non-participants 54% male), part of body injured (participants 59% back injuries, 27% upper limb injuries, and 15% lower limb injuries; non-participants 51% back injuries, 26% upper limb injuries, 12% lower limb injuries, and 12% unknown), and time on benefits (25th centile, median, and 75th centile of the duration distribution are 47 days, 75 days, and 152 days for participants; and 47 days, 76 days, and 157 days for non-participants).

Sample selection to n=907 included in analysis.
For the analysis presented here, only workers still on wage replacement benefits at four weeks post-onset were included. The male to female ratio of claimants to the OWSIB is approximately 2:1; the sampling strategy in this study, however, was designed to include approximately equal numbers of male and female workers. Telephone interviews took place at baseline (the first contact), and subsequently at approximately 4 weeks, 10 weeks, 16 weeks, and 52 weeks post injury. The other main source was data routinely collected by the OWSIB for all lost-time claimants.
Measures
Information was gathered in a wide range of domains as listed in table 1: demographic, clinical, nature of workplace, workplace psychosocial, and recovery expectations. The broad domains and specific factors were chosen based on previously cited publications, critical reviews, and suggestions for prognostic research made in the literature. Wherever possible, standardised instruments with demonstrated measurement properties were selected. For instance, in the clinical domain, standardised instruments were used to measure generic health related quality of life (SF-36 Acute27), body region specific functional status (Roland Morris) for back injuries14,15, the modified ASES (American Shoulder and Elbow Surgeons) for upper extremity injuries,28,29 and the WOMAC (WO from the University of Western Ontario and MAC from McMaster University) for lower extremity injuries30,31 and pain (pain intensity subscale of the Chronic Pain Grade32). A more detailed description of these instruments and their properties is given elsewhere.26 The body region specific functional status measures and the pain grade were all rescaled to range from 0 to 100, with 0 representing poorest health and 100 representing best health. The rescaling was done so that the scale of these measures would have the same range and orientation as the SF-36. In the work domain, response of the workplace to the disabling injury and to compensation status was of particular interest, based on the literature and qualitative studies of injured workers.33–35 Finally, recovery expectation factors build on similar scales used in clinical research. Factors measured at baseline and/or four weeks were eligible for inclusion in the prognostic model.
Factors collected in early claimant cohort either at the baseline or four week interview, or from the Workplace Safety and Insurance Board (WSIB) by major domain
The outcome was the length of the first episode receiving wage replacement benefits from the OWSIB. Follow up started at four weeks post-injury and continued until one year post-injury; that is, the inception point for this study was four weeks post-onset. The outcomes of subjects still receiving wage replacement benefits at one year post-injury were considered censored. It is recognised that “time receiving wage replacement benefits” is a proxy for, but not necessarily equivalent to, “return to work” and/or “recovery” since these terms are often used synonymously in the literature. Given the administrative source of these data and known discordance between time to RTW and time on benefits, however, we have chosen to use time on wage replacement benefits throughout this paper. “Termination of benefits” refers to temporary wage replacement benefits, although workers could go on to receive a more permanent type of benefit later.
Analytical approach
A multidisciplinary research team was assembled to devise a strategy for investigating prognostic factors and developing prognostic models using the study data. A two step approach to variable selection was used. In the first step, variables were clustered into their respective domains as shown in table 1, and small multidisciplinary working groups of researchers with expertise in a particular area met to review preliminary descriptive analysis and recommend variables from their domain to be used in an integrated model of prognosis. This reduction process was used because of the large number of factors measured and because of the probable correlation among some of the factors within groups. Although a more data driven method for data reduction has been used by other investigators,7–11,13,15,16 a great deal of content expertise had been developed within the working groups which we wanted to bring to bear on variable selection decisions. Detailed explanations of each group’s approach are summarised elsewhere.36–39
In the second step, a random sample of approximately half of the cohort was drawn for a learning sample, and model building was carried out using this sample following the procedure outlined in Harrell and colleagues.40 Later, the learning sample and the remainder of the data were pooled to serve as a testing sample. Using the learning sample and starting with all recommended variables as main effects in a Cox proportional hazards model, backward elimination was applied with a p value of 0.05 or greater for removal of factors. For modelling purposes only, each body region specific functional status measure was set to zero for subjects not injured in that particular body region; for instance, the Roland Morris14,15 variable used for modelling was set equal to the measure obtained from the worker if the worker had a back injury; otherwise, it was set to zero. In these modelling steps, the dummy variables representing categorical factors were treated as individual variables and could have been dropped or included regardless of the presence of other levels of the same factor. But for the final model, the following rules were applied. (1) Either all three functional status measures were included in the model or none were, and if included, then the major part of body would also be included (because of scaling differences between the three instruments). (2) For categorical variables, if only one or some dummy variables were selected by the stepwise procedure, a new model was fit using all levels. If the likelihood ratio statistic for that entire variable was significant at the 5% level, or if including all levels altered the coefficients of the chosen levels substantially, the multiple levels were maintained. Otherwise, only the chosen levels were maintained.
Interactions suggested by the working groups were tested after all main effects had been selected. The proportional hazards assumption was checked for all variables in all models using time varying coefficients in a piecewise proportional hazards approach as suggested by Gore and colleagues.41 If the proportional hazards assumption was violated, then the piecewise terms were maintained in the model. The proportion of variance explained by the model R2 and the marginal and partial variance explained for each factor in the model was calculated using the bootstrap approach of Schemper.42,43 Then, the factors in the model were ordered according to the partial R2 values and, following the procedure used by Harrell and colleagues,40 a series of models were fit to the learning sample data, starting with the one most important variable (largest partial R2), then the two most important variables, and so on. A concordance statistic described by Harrell and colleagues44 was calculated for both the learning sample and the testing sample. The value of the concordance measure should continue to rise so long as additional variables improve the discrimination of the model. A variable selected due to noise in the learning sample might not improve discrimination or could make discrimination worse in the testing sample. This would be reflected by a stable or decreasing concordance measure. In this application, a factor which did not increase the concordance measure in the testing sample led to that particular factor and all subsequent factors being dropped from the model.
RESULTS
Altogether there were 1008 workers with new lost-time claims for soft tissue injuries, who were still on benefits at four weeks post-onset, and 907 of those workers had provided complete information on the factors recommended by the working groups. These factors are displayed in tables 2 and 3. Table 2 shows baseline characteristics of the sample. Among the 907 workers, 532 (59%) had soft tissue injuries to the back, 243 (27%) to the upper limb, and 132 (15%) to the lower limb. Four hundred and forty four (49%) were male and 463 (51%) were female. Twenty five per cent of the workers with back claims reported pain radiating below the knee, and 24% of all the workers reported that the injury under study was a recurrence of a previous injury. Just 28% of the workers reported being offered arrangements for return to work by their workplace.
Baseline characteristics of the study sample (n=907) using factors recommended by the working groups
Baseline and four week characteristics of the study sample (n=907) for factors recommended by the working groups
Table 3 shows descriptive statistics for those factors which were measured at both the baseline and four week interviews. Most of the health status and pain measures show significant improvement between baseline and four weeks—although the magnitude of change varies. However, in all cases, the standard deviation of the change scores exceeds the mean, showing that change in the first few weeks is highly variable. The general health dimension of the SF-36 worsened, although the average decline is only 2.5 points on the 0–100 scale. The role emotional dimension of the SF-36 did not show statistically significant change over the two assessments.
The learning sample consisted of 453 observations. The results of variable selection using the learning sample are shown in table 4, listed in order from largest to smallest partial R2 contribution in the learning sample. The three body region specific functional status measures from the four week interview along with indicator variables for part of body contribute the most to the model of time on benefits. Change in pain, workplace offers of arrangements for return to work, and the interaction of these two factors contribute the next highest amount, and these three factors are considered together because of the interaction. Workplace offers of arrangements most often included flexible working hours or modified or altered duties, but rarely changes to the physical work environment. Next recovery expectations are dichotomised into two levels reflecting workers who, either at baseline or at four weeks, report that they will recover soon versus workers who do not think they will recover soon. Also included were household income dichotomised at $60 000 (Cdn) and marital status dichotomised into widowed or divorced versus single or married. The last factor on the list is a dichotomous workplace psychosocial variable representing whether workers reported a negative reaction from their supervisor regarding their claim or that filing a claim might affect their job versus reporting neither of these.
Factors maintained in the Cox model backward elimination ordered by partial R2 values; the concordance index is shown for both the learning (n=453) and testing samples (n=907)
The concordance measure steadily increases with the addition of each variable in the learning sample (table 4). In the testing sample, however, the index stops increasing after the addition of recovery expectations. The results from the validation sample are indicating some over fitting in the model which includes the final three variables. Therefore, the final model, presented in table 5, does not include these final three factors of income, marital status, and the workplace psychosocial factor.
Final Cox model including β coefficient, standard error (SE), p value, hazard rate ratio (HRR), and a 95% CI for the HRR
Table 5 shows the final model including the β coefficients, their standard errors, the associated p value for each coefficient, a hazard rate ratio, and a 95% confidence interval for the rate ratio. Overall, this model explains 39% of the variance in the outcome in the learning sample. As indicated in the right hand column of the table, two of the functional status measures (for back and upper extremity injuries), the change in pain grade and the interaction between change in pain and workplace offers, were modelled using piecewise proportional hazards terms. For each of these, the relation between the factor and the outcome was found to be strongest over the first eight weeks under study (that is, from four weeks post-accident date to 12 weeks post-accident date) and negligible for the remainder of the follow up period. In other words, these factors have a relation with the rate of ending benefits for the eight weeks after the measurement was taken, but after that, they do not contribute to the prediction model. Generally, the model indicates that the higher the functional status measure, the more quickly benefits ended. When no offers of arrangements for RTW were made by a workplace, then change in pain between the baseline and four week interviews is predictive of time on benefits with workers whose pain was improving showing more rapid termination of benefits than those whose pain was stable or worsening. Like functional status, this measure’s relation with the outcome is strongest in the first eight weeks of follow up.
However, the interaction term indicates that when workplace offers of arrangements for RTW were made, the relation between change in pain and time on benefits is much weaker. Table 6 shows the interaction between these two factors. Median days on benefits are shown for those workers receiving or not receiving workplace offers of arrangements over different groupings based on reported change in pain, functional status, and recovery expectations. Also shown is the percentage in each group who received workplace offers. This percentage clearly declines as severity of injury increases. For those workers whose pain was improving and functional status and recovery expectations were high, there was little or no difference in median days on benefits for those with and without workplace offers. There are large differences, however, for those reporting stable or worsening pain as well as for those reporting improving pain but low functional status and recovery expectations. Finally, workers who did not think they would recover soon at both the baseline interview and the four week interview, remained on benefits longer than those workers who thought they would recover soon.
Median days on benefits (and 95%CI) in the test sample for given combinations of key variable from the predictive model
Of note, in reviewing the reduced list of variables, is the overlap between those that remain in the final model and those that were dropped. For instance, the Roland Morris disability scores (which are included in the final model) were significantly worse in the sample for those back injury claimants with radiating pain, those with constant pain (rather than intermittent pain), those with a past history of back pain, those who have had prior surgery to their back, those whose supervisor reacted to the injury in a negative way, those who thought filing a claim would affect their job, those who are older, those with poor facility with the English language, and those with lower household incomes. All of the latter variables were not retained in the final model.
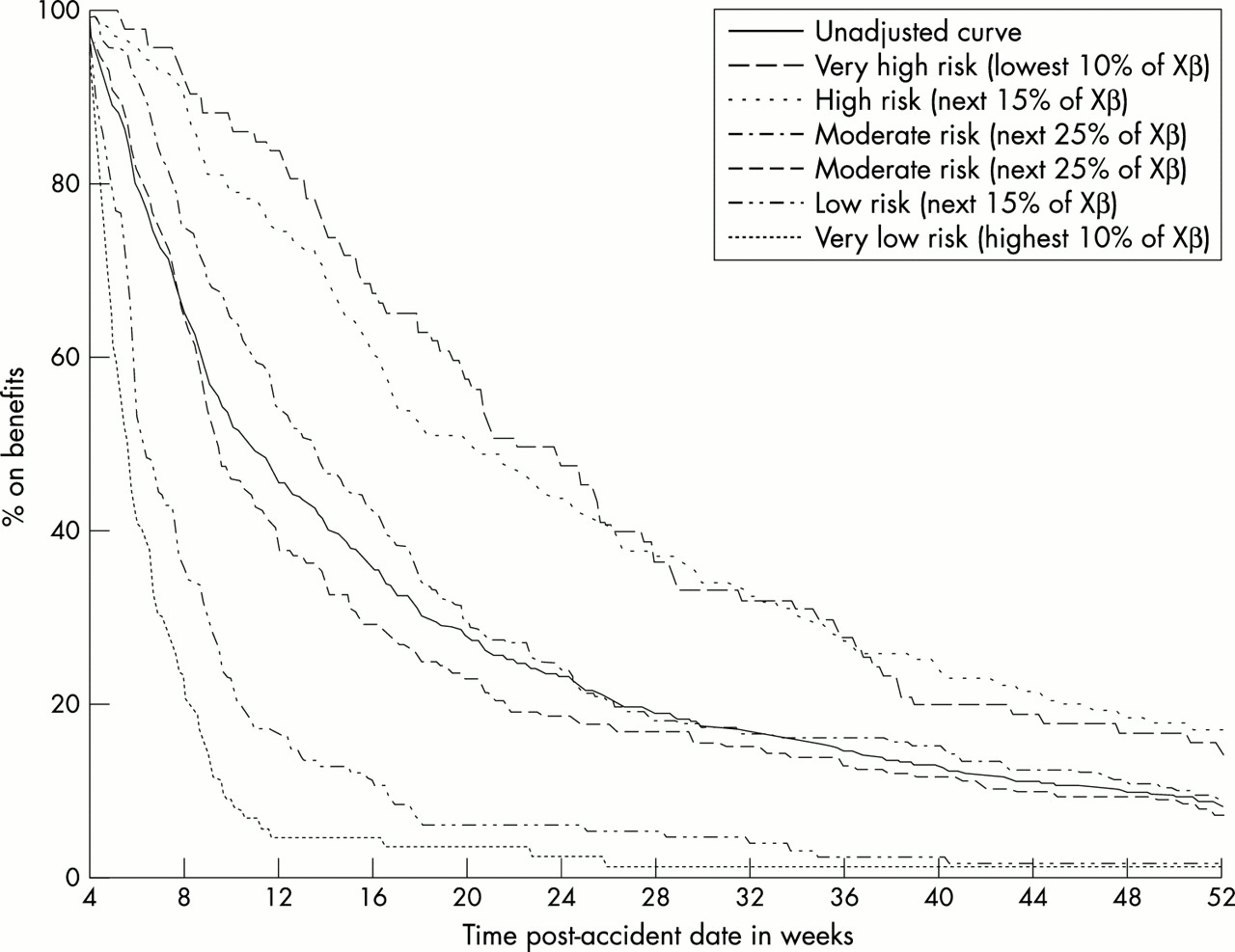
The empirical survivor function for the sample of 907 workers is shown as the unadjusted curve in fig 2. Although 50% of claimants received wage replacement benefits for 75 days or less, approximately 10% received wage replacement benefits continuously for the entire year post-injury, and 16% went on to receive longer term future economic loss awards due to permanent impairment. Note that the shape of the curve here may be somewhat different from other published soft tissue recovery curves,1,3,4,18,45 not only because of differences in jurisdiction and setting, but also because of the sampling scheme used in this study; only workers who were still on benefits at four weeks post-onset were included. Also in fig 2, the workers in the testing sample have been grouped according to the value of Xβ, the risk score, from the fitted model shown in table 5, where β is the vector of coefficients from the model and X represents the vector of selected variables (functional status, change in pain, etc). For the time varying coefficients of functional status and change in pain, the coefficient value for the first eight weeks is used. Based on these values of the risk score, the subjects were divided into six groups: the 10% with the lowest value of Xβ (lowest rate of RTW), followed by the next 15%, the next 25%, the next 25%, the next 15%, and then the final 10% (highest rate of RTW). The unadjusted duration curve presented is included in the figure for comparison. A marked distinction in duration experience is apparent for these six groups, with considerable variation around the unadjusted curve—for example, at four months, only one third of the highest risk group had gone off benefits, while over 95% of the lowest risk group had done so.
{kind=link}
{kind=link}
Duration curves for time on benefits for different risk groups as defined by the prognostic model, with the unadjusted curve for comparison. Xβ, the risk score; β, the vector of coefficients from the Cox model in table 5; X, the vector of selected variables (functional status, change in pain, etc).
DISCUSSION
This study of workers’ compensation claimants with soft tissue injuries has identified a relatively small number of factors, gathered in the acute phase of disability, which predict prolonged disability in the first year. In terms of rigour, it met generally accepted criteria for quality of evidence from prognostic studies.5,23,46 A prospective cohort was recruited close to the onset of disability (inception) and it was of sufficient size to detect prognostic factors of importance. Clear inclusion and exclusion criteria were applied. Building on earlier critical reviews,47 a very broad range of prognostic factors from distinct domains were measured at baseline, using both primary data collection and administrative data sources. Using an administrative database for outcome assessment guaranteed both blinding and complete follow up. Missing data were kept to a minimum, preserving sample size for modelling purposes. The statistical methods employed have taken into account the time dependent nature of potential prognostic factors, their joint effects, and the need for learning and test phases of model development. Hence, we can have greater confidence in the results than has been possible for many prognostic studies in this area of research.47
Significant prognostic factors in this study cover three domains that were felt to be important in other studies of prognosis for soft tissue injuries: clinical, work, and recovery expectations. In the clinical domain, three body region specific measures of functional status, which were all summary rating scores from multi-item questionnaires, greatly contributed to the predictive model. The attenuation in their ability to predict time on benefits past the eight week period after they were measured probably reflects their changing values during recovery, suggesting the possibility that they may need to be periodically readministered. This attenuation could also be related to natural healing times, since clinically, 12 weeks post-onset is considered to be the approximate time of biological healing for soft tissue injuries. A number of studies in the low back pain literature have also identified the predictive ability of functional status measures, although no others have reported the attenuation seen here. Of the six studies identified earlier which included such a measure,7,8,12–16 the functional status or disability score remained in the final model in five cases. For the one exception,13 the investigators point out a high correlation between the disability score and another variable in the model, the number of days off work prescribed by a physician. This observation parallels some observations we made with this data set; that is, the relation between functional status and some other, previously identified prognostic factors for soft tissue injuries. The functional status measures are established multi-item measures with shown measurement properties,14,15,28–31 unlike some of the other measures under consideration. Therefore, there may be less measurement error associated with these multi-item measures than with the others. This too could explain the selection of the functional status measures over a number of other potential prognostic factors. Or perhaps functional status measures are able to sum up or capture the overall state of the individuals with respect to their injuries in much the same way that an observant health care practitioner is able to give an overall assessment of the state of an individual.
Also within the clinical domain was “change in pain” between baseline (on average two weeks post-injury) and approximately four weeks post-injury. Pain has been included in the predictive model of some of the studies reviewed earlier,8,10,12 but often as an initial measurement rather than a change score across the acute stage.
The contribution of “change in pain” to prediction was substantial, not only alone as a clinical factor, but also in interaction with a factor from the workplace domain, workplace offers of arrangements for return to work. Availability of alternative duties was considered, but not included in the final model, in just one of the reviewed studies.9 However, in that study, a variable based on the worker’s company of employment was included, perhaps capturing the availability of alternative duties which depend on company specific policies and programmes. Workplace programmes for rehabilitation or early RTW have been studied by other investigators and found to be effective in reducing the amount of time lost from work in a variety of jurisdictions including Québec and Manitoba.25,48–50 Caution is called for, however, when interpreting the influence of such offers in jurisdictions such as Ontario and Québec, where workers are obliged to cooperate when their workplace tries to accommodate an RTW. If the worker does not return to work, she/he may face a reduction in the amount of wage replacement received in workers’ compensation benefits. We also cannot tell whether those going back to work after offers of accommodation incurred any harm, perhaps by increasing workers’ pain or increasing the risk of reinjury. Although such possibilities require further investigation, we believe that our finding that offers of accommodation can particularly reduce work disability duration among those with little change or even worsening of pain and poor expectations of recovery should bolster workplace accommodation efforts for such high risk cases.
The variable in our model on recovery expectations is different from that encountered in the soft tissue literature to date. The Vermont Rehabilitation Engineering Center predictive model for low back pain is based on a questionnaire which includes two questions on expectations: one on trouble sitting or standing in six weeks, and one on working in six months.6,10 In our current study, whether the injured worker thought she/he would recover soon or not was the only variable to contribute significantly to prediction. Recovery expectations may reflect some of the psychological response to pain found predictive by Klenerman and colleagues.12 They may also be an injured worker’s way of reflecting on his/her overall state and comparing it with past experience, knowledge of the course for co-workers with similar injuries, and an estimate of job demands. Given the important role recovery expectations play in prediction, response to treatment and negotiation of return to work, they warrant further systematic investigation in the compensable soft tissue injury area.
Absent among our predictive factors were domains of importance in some other prognostic studies: demographic factors and workplace descriptors. Income and marital status were among those demographic factors that initially accounted for some variance, but neither age nor gender were significant predictors. Similarly, company size, industrial sector, and job factors were not significant. Their exclusion, along with a range of clinical variables cited in the literature, may be because some of the variance due to other features of the injury, the individual, the workplace or the clinical presentation was captured by factors already in the model. As examples, one might think of the poorer health of women and older people as measured by functional status measures,51 the variation in availability of modified work programmes by company size and industrial sector,52 and the correlation of past history of back pain and radiating pain with poorer scores on the Roland Morris disability score. In these instances, the measures in the model may be markers for factors that other researchers have identified as prognostic. Alternatively, the study population and the context of work related disability from soft tissue injuries in Ontario may be different. Such interjurisdictional concerns can only be allayed through replications of primary and secondary data collection on a range of potential predictors under other workers’ compensation systems.
By basing our prognostic model on such measures, it may be of limited utility to compensation administrators or clinicians without access to the factors measured on the injured workers with whom they deal. Administrators may prefer workplace descriptors to facilitate targeting of secondary prevention programmes. Clinicians may prefer signs on physical examination which must be documented anyway. On the other hand, each of our predictors could be routinely collected without much additional effort via simple questionnaires, either during claims processing or office visits. Nevertheless, alternative models for such constituencies could be developed based on the data from this study, but using only factors readily available in those constituencies while excluding global disability measures, the same way that clinical researchers have focused on rapid measures which can predict chronicity in the office setting.6,10
Our results have shown that after four weeks of lost time, we are able to identify claimants likely to end benefit receipt very quickly and others likely to remain on benefits for longer periods of time. It is less clear what these factors say about the longer term process of recovery. This process may best be studied by including repeated measures over time to focus on later predictors of the evolution of chronic problems, and we plan to continue the work presented here by undertaking such an analysis. At a minimum, we suggest that whenever primary data are being collected, researchers include formal assessment of pain and functional status, so that the clinically sensible determination of changes in such variables can be incorporated into prognostic modelling. We would also urge both researchers and clinicians to consider asking simple questions about workplace efforts to make accommodations as well as patient expectations of recovery. For clinicians in particular, this may lead to fruitful avenues of discussion with the injured worker and the other workplace parties. Open communication between the worker, the health care provider, and the workplace is of demonstrated importance in the return to work process.53 Finally, these results may lead to interventions which will facilitate more rapid return to work, to the benefit of injured workers, employers, compensation insurers, and society at large in the reduction of prolonged disability due to soft tissue injuries.
Main messages
-
Wide variations in time on compensation benefits can be predicted by a set of simple questions repeated during the first month off work among those with soft tissue injuries.
-
Early assessment of pain and functional status during the course of recovery from a workplace musculoskeletal injury can be used to predict the likely future course.
-
Offers of workplace accommodations for return to work provided the greatest reduction in time on benefits among workers with little change in pain and poor recovery expectations.
Policy implications
-
Injured workers with soft tissue injuries could be triaged within the first month using a small set of prognostic factors. Such triage would enable focused efforts to promote return to work among those at highest risk of remaining off work.
Acknowledgments
SJS, SHJ, DC, and JF designed the study, SJS prepared the protocol and conducted the study, and SHJ conducted all the analysis presented in this paper. SHJ was the lead writer of the paper with co-author DC. The Prognostic Modelling Workgroup (SHJ, DC, SJS, JF, DB, CB, ASB, JC, SF, HH, PH, RM, MM, HS, SS, JS) conducted early exploration of the prognostic factors and contributed to initial variable selection and interpretation. This project was sponsored by the Institute for Work & Health. The Institute, an independent, not-for-profit research organisation, receives support from the Ontario Workplace Safety & Insurance Board.
REFERENCES
Footnotes
-
Early Claimant Cohort Design Group (John W Frank, Sandra J Sinclair and co-authors)
-
Early Claimant Cohort Prognostic Modelling Workgroup (Dorcas Beaton, Claire Bombardier, Ann Sylvia Brooker, Judy Clark, Sue Ferrier, John Frank, Hassan Haidar, Pam Hudak, Robert Marx, Michael Mondloch, Harry Shannon, Susanne Shields, Sandra J Sinclair, Jonathan Smith, and co-authors)