Article Text

Abstract
OBJECTIVES To assess the health of United Kingdom Gulf war veterans, to compare their health to that of similar personnel not deployed, to describe patterns of ill health in both groups, and to estimate their extent.
METHODS Main Gulf (n=4795) and validation Gulf (n=4793) cohorts were randomly selected within strata from the population deployed to the Gulf and a non-Gulf cohort (n=4790) from those who were not sent. Seven years after the war subjects completed a questionnaire about their health in the past month, including 95 symptom questions and two manikins on which to shade areas of pain or numbness and tingling. Responses were subjected to a principal component analysis with rotation and to a cluster analysis within each cohort. Mean symptom score was used as a measure of severity. Areas shaded on the manikins were coded to indicate widespread pain and possible toxic neuropathy.
RESULTS A response of 85.5% was achieved. Those who had been to the Gulf were more troubled by every symptom with a mean severity score (3.0) substantially greater than in the non-Gulf cohort (1.7). Seven factors were extracted accounting for 48% of the variance. The scores on five factors (labelled psychological, peripheral, respiratory, gastrointestinal, and concentration) were significantly worse in those who had been to the Gulf. Symptoms suggestive of peripheral neuropathy were found more often (12.5%) in the Gulf than the non-Gulf (6.8%) cohorts. Widespread pain was also found more often (12.2% Gulf; 6.5% non-Gulf). Those who had been to the Gulf were found disproportionately (23.8%) in three clusters with high mean severity scores; only 9.8% of non-Gulf respondents were in these clusters. There was no evidence of an important excess in the use of alcohol, tobacco, or referral to hospital specialists by those who had been to the Gulf. For the same level of reported ill health those who had been to the Gulf were less likely to be referred to specialists than non-Gulf veterans.
CONCLUSION 7 Years after the war, the Gulf war veterans were more troubled about their health than those who had not been sent, with a substantial subgroup reporting a pattern of symptoms suggestive of a significant decline in health.
- Gulf war
- symptoms
- clusters
Statistics from Altmetric.com
Follow up studies of random samples of men and women who served in the Gulf States in 1990–91 have shown—in the United States,1 2 Canada,3 the United Kingdom,4 and Denmark5—that veterans report considerably greater ill health than other service personnel. The syndromes identified in Gulf war veterans have been determined by the type of instrument used and the interest of the research team, but have included post-traumatic stress disorders,1 chronic fatigue syndrome,4 6 fibromyalgia,1 7 and multiple chemical sensitivity.6 Although several studies have considered the possibility of an unusual cluster of symptoms specific to experience in the Gulf, few study designs have had the capacity to investigate this thoroughly, and no novel syndrome has been identified that has been accepted by the scientific community.
The present report describes the pattern of symptoms reported by men and women from the United Kingdom who were sent to the Gulf and those who were not, and assesses the extent to which service in the Gulf was associated with excess ill health.
Methods
The Ministry of Defence (MOD) identified all men and women deployed to the Gulf or Gulf states between September 1990 and June 1991. These personnel were stratified by sex, age (in 5 year groups), service (army, Royal Navy, Royal Air Force), and rank (commissioned officer, other ranks). Each stratum was then matched with a randomly selected sample of equal size from the cohort of personnel in the military forces at 1 January 1991, who were not deployed to the Gulf but whose health, at the most recent medical assessment before the war, would not have prevented that deployment. The complete study cohorts of Gulf and non-Gulf personnel were included in a study of mortality.8 Because of security risks entailed by contacting subjects, those serving in the special forces were excluded from the present study and thus no conclusion can be drawn about the effects of exposure on their health. Three stratified random samples were then taken, a total of 14 372 men and women. To examine the consistency of results two equivalent cohorts were chosen from those who went to the Gulf—a main Gulf and validation Gulf cohort. A non-Gulf cohort was also selected. These study cohorts did not overlap with those in the United Kingdom study already reported4; all included here will have been approached eventually as part of a study of reproductive effects, that contact was made only after collaboration with the present study had been completed.
All subjects were given a health questionnaire which sought information on current employment (service or civilian), marital status, deployment to other areas of conflict, attendance at hospital since 1991, and habits (alcohol, tobacco). They were also asked in detail about health during the past month, indicating on an adjacent visual analogue scale, ranging from “not at all” to “very seriously”, how much they had been troubled by each of 95 symptoms. The choice of symptoms was made through review of published reports on Gulf war illness, discussion with service personnel who had been in the Gulf, and consideration of illness that might result from exposures—such as pesticides and smoke from burning oil wells—known to have occurred. Subjects were also asked to shade sites of pain (on one manikin) and numbness or tingling (on a second) that had been troublesome in the past month.
Those deployed to the Gulf also completed a second questionnaire giving details of the dates they had been deployed at each location and of exposures that they had experienced while in that area. They were instructed to complete the health questionnaire before beginning that on locations.
Questionnaires were always self completed but the method of administration differed between groups. For those no longer serving the first approach was by post, with discharge addresses supplied by the MOD. For those still serving the approach differed by service. Most of the serving personnel were in the army, and for these, bases were visited in the United Kingdom, Germany, and Cyprus; subjects selected for the study were gathered together to complete the forms in the presence of one of the research team. Such an approach was inappropriate for the navy where service at (or under) sea effectively precluded personal visits. For the air force, where small numbers were spread over many sites, visits by the research team to bases were not planned but one large air force base was included in the site visit to Cyprus. For army personnel not successfully encountered at the site visits and for those in the navy and air force the approach was by post to the service address supplied by the MOD.
Follow up of untraced subjects and non-responders took many forms. For those still serving, telephone contact was made with the base to ensure that the address was correct and that the subject was still stationed there. Where units had moved, the new location was supplied by the MOD. For those in civilian life possible new addresses were obtained through electoral registers, health authorities, and telephone directories. Questionnaires were forwarded by the Driver and Vehicle Licensing Authority (DVLA), by some general medical practitioners, and for a small group of non-responders who had served in the Gulf, the medical assessment programme of the MOD.9 Where a firm address had been established but the subject had not completed a questionnaire, a telephone contact or home visit was attempted. Where no other option seemed likely to succeed, subjects were asked to complete a shortened form of the questionnaire.
The first site visit was carried out in December 1997, 6.5 years after the end of the Gulf war. Follow up continued until September 1999.
STATISTICAL METHODS
Responses on each 10 cm visual analogue scale were allocated, as a symptom score, to 1 of 21 equally spaced segments. The mean symptom scores overall in both the Gulf and non-Gulf groups were highly skewed, with most respondents reporting little trouble, but the square root of the mean score approximated normality and has been used to test significance. Factor scores on seven specific dimensions were derived by principal component analysis (discussed later). With the technique of cluster analysis (discussed later) each respondent was allocated to a group (or cluster) within the same cohort in which the pattern of 95 symptom scores of others in the group were as similar as possible to those of the subject. The size of these clusters was used to estimate the extent to which experience in the Gulf had changed patterns of health.
Areas shaded on the manikin to indicate numbness or tingling were used to define patterns consistent with toxic neuropathy. Possible neuropathy was classified as “limited” if restricted to one or both feet and “extended” if numbness or tingling were reported in both feet and at least one hand or lower leg. Areas shaded to indicate pain (experienced for at least 24 hours in the past month) were used to define a syndrome of widespread pain present if there were axial skeletal and contralateral body pain.10
Principal component factor analysis
The symptom correlation matrix was analysed, with the initial extraction method that of principal components. The varimax procedure was used for rotation, producing a set of orthogonal factor scores, standardised to a mean (SD) of 0 (100). The matrix of weights in the rotated solutions for each of the three cohorts separately were compared by eye in successive analyses, with the extraction of increasing numbers of components. Solutions in which the matrices were judged to be essentially identical in the main and validation cohorts were retained. For each such solution the structure extracted in the Gulf and non-Gulf cohorts were compared, to explore the possibility of a replicable solution in those who had served in the Gulf but not present in the non-Gulf cohort.
Cluster analysis
A k means cluster analysis was used.11 12 The non-hierarchical method initially partitioned the respondents into k clusters (k specified by the investigator) with each subject reassigned in turn until an optimal solution was reached in which the distance between cases in different clusters was maximised. This analysis was carried out for the three cohorts separately, with scores from the 95 symptoms. In each case convergence was reached within 200 iterations. The solutions for the three cohorts were again compared by eye, as the number of clusters was increased sequentially. The solution chosen was that with the largest number of clusters in which the pattern of component scores seemed to be essentially the same in the different cohorts.
Validation cohort
The study design, with main and validation cohort selected from those deployed to the Gulf, permitted replication of analyses. Results from each of the Gulf cohorts are given where consistency between cohorts is important in assessing the weight that should be given to the interpretation.
Results
One hundred and eighteen members of the sample died before study contact but of 14 254 surviving, 12 191 (85.5%) completed a questionnaire (table 1). Of these, 164 were short questionnaires and seven were completed through the medical assessment programme; these have been excluded from the main analyses, the short questionnaires because they did not complete comparable symptom data, those completed through the medical assessment programme because there was no equivalent system for contacting sick non-Gulf subjects.
Response by cohort
The response was higher for those still serving (5645/6086, 92.8%) than those who had left the forces (6546/8168, 80.1%). Among the non-responders a very high proportion could not be traced to a current address. Although there were only four in the study for whom no address of any sort could be found (two absent without leave from the forces, two thought to be in Northern Ireland where security decreed only a minimal follow up) the address supplied by the MOD for many others proved to be outdated. Among subjects who were contacted to complete the study questionnaire 183 refused but were asked to confirm whether or not they were in good health. Of the 47 willing to provide this minimal information, only one admitted to being unwell.
In the surviving cohort 2.3% were women, 49.3% aged less than 25 years, and 12.5% were officers. The largest numbers were from the army (70.1%) with 18.8% from the air force and 11.1% from the navy. The pattern of response is shown in table 2. The response rate was somewhat lower in those who did not go to the Gulf, particularly in women and those under 25 years. In both Gulf and non-Gulf groups there was a marked increase in response with age. Younger service personnel were more likely to be on a short term engagement and to have left the forces without a pension; tracing in this group was particularly difficult as there was no incentive for them to maintain a current address on MOD records.
Response by subject characteristics2-150
SYMPTOMS
A total of 11 914 (99.1%) provided usable answers to at least 90 of the 95 symptoms and have been included in the main analysis. The subject's mean response to all other symptoms was assigned where five or less symptoms had been missed.
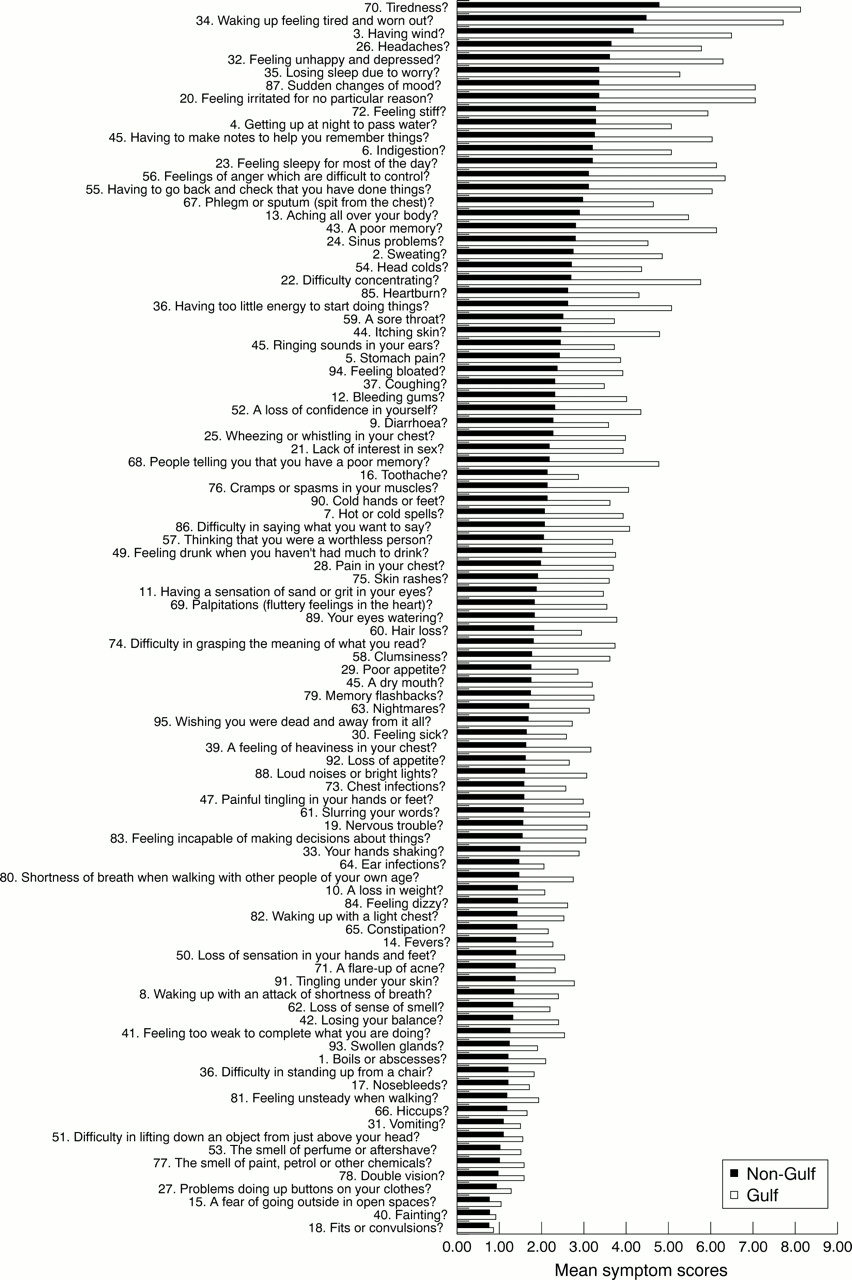
The mean score for each symptom is shown in figure 1 by order of decreasing severity in the comparison group. It is evident that symptoms that were rated as particularly troublesome in the non-Gulf group were also rated in much the same order in the Gulf group, with feelings of tiredness being the most troublesome symptom in both groups, and fits or convulsions the least. A rank correlation between mean scores for the 95 symptoms in the Gulf and non-Gulf cohorts exceeded 0.95. On every symptom the score was higher for those who were deployed. However this tendency to report greater severity in the Gulf group was not uniform; for example Q68 (people telling you that they have a poor memory) and Q16 (toothache) had very similar mean scores (2.1 for both) in the comparison group but in those who had been to the Gulf memory was seen as much more troublesome (with a mean score of 4.8) than toothache (2.8). The 14 symptoms on which the scores for the Gulf cohort were at least twice those for the non-Gulf cohort are shown in table 3.

{kind=link}
Mean symptom scores in the Gulf and non-Gulf cohorts.
Symptoms on which the mean score for Gulf veterans (n=8014) was at least twice that for the non-Gulf cohort (n=3900)
The difference between the two cohorts in the areas shaded on the manikins suggested that those who went to the Gulf were more likely to experience symptoms consistent with peripheral neuropathy (6.0% limited symptoms, 8.5% extended) than the non-Gulf cohort (4.5% limited, 2.3% extended). The proportion with widespread pain (12.2%) was also higher in the Gulf than in the non-Gulf (6.5%) cohorts.
Mean symptom severity scores were very similar in the main Gulf cohort (3.1) and validation cohort (3.0) but significantly lower in the non-Gulf cohort (1.7) (comparison of means for Gulf and non-Gulf cohorts; p<0.001).
In both Gulf and non-Gulf cohorts lower scores were found in older people (under 25 years 3.3, 25 years or older 2.8), officers (2.0, other ranks 3.2) and those still serving (2.7, no longer serving 3.4). Neither marital status at the time of the Gulf nor sex significantly affected symptom scores. Differences in severity score were found between services in both Gulf and non-Gulf cohorts; in the non-Gulf cohort those from the army had a mean score of 2.1, the navy 1.8, and the air force 1.7.
PRINCIPAL COMPONENT ANALYSIS
Principle component analysis (with rotation) was carried out to explore the structure of response to the symptom questionnaire. The analysis was conducted for each of the three cohorts separately and the results obtained by extracting different numbers of factors were examined. The solutions obtained for the main and validation cohorts were similar when up to seven components were extracted and rotated but when more components were extracted the factors differed between Gulf cohorts. In each solution up to seven components the rotated solutions seemed to be essentially the same for the non-Gulf as well as the Gulf cohorts. The analysis was then repeated (table 4) to obtain a single seven factor solution for all three groups together. To facilitate interpretation only questions on which the weight was 0.4 or greater on any of the first seven factors (accounting for 48% of the variance) are shown in table 4. A brief label has been given to each factor: (1) psychological, (2) peripheral, (3) neurological, (4) respiratory, (5) gastrointestinal, (6) concentration, and (7) appetite. These labels are for identification only and not necessarily of diagnostic significance. Factor 2 was most difficult to name in an informative way; peripheral reflects the skin and neuromuscular complaints weighted most heavily on this factor.
Analysis of principal components with varimax rotation: weights (⩾0.4) assigned on each of seven factors
The mean scores on each of these factors are shown for the three cohorts in table 5. The scores for the main and validation Gulf cohorts were very similar with no significant difference on any dimension. There was, however, a clear and significant difference between the Gulf and non-Gulf cohorts in six of the seven factors. Five factors (psychological, peripheral, respiratory, gastrointestinal, and concentration) had higher scores in the Gulf cohorts. One factor (appetite) was significantly lower than in the non-Gulf cohort. No difference was found for the neurological factor, which, as seen in table 4, had high weightings not only on peripheral symptoms but also on symptoms that might arise from poor functioning of the central nervous system.
Mean factor scores by cohort
CLUSTER ANALYSIS
To further assess the impact of service in the Gulf on the health of veterans, a series of cluster analyses was carried out using scores for all 95 symptoms and clustering subjects in each of the three cohorts separately. The aim was not to identify a cluster unique to the Gulf veterans, but to look for common groups of symptoms.
With six clusters a pattern was found that could be interpreted by use of the seven factors from table 4. When each subject was assigned to one of six clusters, the mean scores for each factor were as shown in table 6 with the six clusters arranged in order of decreasing numbers of subjects and increasing overall severity (table 7). The scores were standardised to a mean (SD) of 0 (100); thus from table 6 the mean factor score for psychological ill health for people in cluster 1 was about 0.5 SD below the mean in all three cohorts. The clusters formed independently from the main and validation Gulf cohorts were very similar. The differences between the Gulf and non-Gulf cohorts were greater, particularly on the smaller clusters (4–6).
Mean factor scores by cluster and cohort
Distribution of cohorts by cluster
Cluster 1 was essentially composed of those who were well, with scores appreciably below the mean on five factors and close to the mean on the remaining two. The proportion of the Gulf cohort in this healthy cluster was smaller (36.4%) than the non-Gulf (48.5%) (table 7). Those in cluster 2 (accounting for nearly 30% of each cohort) were also essentially well but with slightly higher symptom scores and perhaps more peripheral and gastrointestinal problems. Cluster 3 contained the same proportions of Gulf and non-Gulf veterans but the scores for those in the Gulf cohorts were appreciably higher on the two factors (psychological and memory or concentration) that characterise this cluster. In the remaining clusters those who served in the Gulf war were overrepresented. Thus cluster 4, with high scores on respiratory and gastrointestinal problems, accounted for only 4.5% of the non-Gulf respondents but 11.6% of the Gulf war veterans. In cluster 5, characterised by high scores for psychological ill health in all cohorts but with relatively high scores also for other factors in the Gulf cohort, the proportions from the Gulf cohort were again more than twice as high as in the non-Gulf cohort. Cluster 6, the smallest, contained only 3.1% overall, but again had higher proportions of those who went to the Gulf. Those in this cluster had high symptom scores on all factors with noticeably higher scores on the factor associated with neurological symptoms. Together these three least healthy clusters include 23.8% of the Gulf but only 9.8% of the non-Gulf cohorts.
HEALTH BEHAVIOURS
The proportion of subjects who had been referred to hospital by their general practitioner was high overall with only slightly greater rates in the main Gulf (52.5%) and validation Gulf (51.6%) than in the non-Gulf cohort (49.0%) (difference Gulf/non-Gulf p<0.002). The likelihood of being referred was strongly related, in both Gulf and non-Gulf cohorts, to the symptom cluster, with only 40.6% of those in cluster 1 consulting a specialist but 73.3% of those in cluster 6. It is of note that in the three least healthy clusters (4–6) Gulf veterans were less likely (65.9%) than non-Gulf veterans (73.3%) to be referred by their family physician for specialist investigation or treatment (p=0.005).
The proportion of current smokers was very similar in the three cohorts (36.5% main Gulf, 34.4% validation Gulf, and 33.4% non-Gulf). Only 7.0% of those who went to the Gulf, and 6.7% of those who did not, smoked more than 20 cigarettes a day at the time they were contacted. The proportions who drank more than 20 units of alcohol a week were also comparable, with 17.9% of Gulf war veterans and 16.6% of the non-Gulf cohort reporting this amount.
Discussion
The study reported here was set up to investigate whether there was an excess of ill health among those who went to the Gulf. It is clear that the veterans were more troubled about their health than comparable non-deployed subjects and that these concerns covered a wide range of symptoms. The use of cluster analysis, exploiting similarities rather than differences between the cohorts, allowed estimation of the size of the group affected; the proportion in the three least healthy groups was 14% more in the Gulf than in the non-Gulf cohorts, providing an estimate of about 7500 veterans (of 53 462 deployed) with ill health attributable to the Gulf. Less than half this number have so far presented to the MOD's medical assessment programme.9In a recently published and broadly comparable study from the United States,2 the proportions reporting “functional impairment” (that during the past 2 weeks they had stayed in bed or at home because of ill health) corresponded quite closely to the proportions in the three least healthy clusters in the present study. Among the United States Gulf veterans 27.8% reported impairment compared with only 14.2% of non-Gulf veterans.
Interpretation of these data is not easy, particularly in the absence of objective measures of the prevalence of conditions—such as peripheral neuropathy—which might plausably result from exposures in the Gulf. Previous studies in the United States have not found an increase in mortality13 or hospital admissions of Gulf War veterans14 15 and in the present cohort, those who had been to the Gulf were no more likely to have died.8Although there was no marked increase in the proportions who had been referred to specialist physicians, the lower referral rate for Gulf than non-Gulf veterans in the three least healthy clusters suggest that, in the United Kingdom, any increase in morbidity was being managed largely within primary care. In the most comparable United States study,2 more visits to a clinic during the previous year were recorded by Gulf (51%) than non-Gulf (41%) veterans. In the present study the greater psychological and other concerns in Gulf war veterans do not seem to be translated into higher rates of cigarette smoking or drinking of alcohol, which would lead to an excess of chronic ill health.
Although this lack of an excess in signs of severe morbidity is reassuring, there is nevertheless clear evidence, consistent across the cohorts, that among those who went to the Gulf there are substantial subgroups who feel unwell. Such ill health has been reported after previous conflicts16 and it may be that this reflects changes in perception resulting from disruptions of war rather than specific chemical, physical, infective, or psychological exposures. The hypothesis that exposures during deployment contributed to the ill health of United Kingdom Gulf war veterans is investigated in part II of this paper.17
Many journals, including the BMJ, have moved to a system of open reviewing, whereby authors know the names of reviewers of their papers. Research has shown that named reviews, although not of better quality than anonymous reviews, are not of worse quality either. Therefore in the interests of transparency, it seems fair to let authors know who has reviewed their paper. AtOccupational and Environmental Medicine we have considered the issue carefully. There are some concerns that reviewers, especially those who are more junior, might feel intimidated and not wish to make negative comments about papers submitted by senior people in the field. On the other hand, some reviewers might hide behind the cloak of anonymity to make unfair criticisms so as to reduce the chances of publication by rivals. We have decided to introduce initially a system of open reviewing if the reviewers agree explicitly. So when a reviewer is sent a paper, he or she is asked to indicate whether we can disclose their name or not when sending the authors their comments. We will be monitoring this to see how many of our reviewers are happy to be named. If it is most of them, we will move to a system of open reviewing as the norm, with a possible “opt out” clause for reviewers.
Acknowledgments
We are grateful to Priscilla Appelbe who administered the study, to Joanne Wren, Melanie Hopwood, Gill Prior, and Vincent Burke who implemented the follow up, and to Liz Foster and Tracy Field who cleaned the data. Ministry of Defence staff (in particular John Graham and Nick Blatchley) identified the study cohorts who were traced on the NHS Central Register by staff from the Office for National Statistics. We also thank everyone who helped with tracing, particularly Linda Walpole, Amanda Bale, Bernie Page (from DASA), and Steve McManus.