Article Text

Abstract
OBJECTIVES In a cross sectional study, work related health complaints and diseases of 58 compost workers and 53 biowaste collectors were investigated and compared with 40 control subjects. Levels of specific IgG antibodies to moulds and bacteria were measured as immunological markers of exposure to bioaerosols.
METHODS With a standardised protocol, the participants of the study were interviewed for work related symptoms, conditions of exposure to bioaerosols at their workplaces, exposure to bioaerosols from other sources, atopic diseases, and smoking habits. They were clinically examined by physicians specialised in occupational medicine. Also, concentrations of specific IgG antibodies against antigens of moulds and actinomycetes occurring regularly at these workplaces were measured and compared with the health complaints of the workers.
RESULTS Compost workers had significantly more symptoms and diseases of the airways (p=0.003) and the skin (p=0.02) than the control subjects. Health complaints of biowaste collectors did not differ significantly from those of the control group. Subjects with atopic diseases were underrepresented in the compost workers (p=0.003). Significantly increased antibody concentrations against fungi and actinomycetes were measured in workers at composting plants. The concentrations in biowaste collectors did not differ significantly from those in the control subjects. A significant association between the diseases and increased antibody concentrations were found in the compost workers.
CONCLUSION The high exposure to bioaerosols of compost workers is significantly associated with a higher frequency of health complaints and diseases as well as higher concentrations of specific antibodies against moulds and actinomycetes. A healthy worker effect is indicated by the underrepresentation of atopic diseases among the compost workers compared with biowaste collectors and the control group.
- exposure to bioaerosols
- organic dust
- IgG antibodies
- moulds
- actinomycetes
Statistics from Altmetric.com
Filamentous fungi (moulds) and bacteria grow in biowaste or on biologically contaminated waste. When these materials are handled, airborne microorganisms and spores are emitted into the air as inhalable organic dust or bioaerosols.1 These terms are often used synonymously. Concentrations of 107 colony forming units per m3 air (cfu/m3) of airborne microorganisms have regularly been measured in composting facilities, whereas exposures of biowaste collectors were in the range of 105 cfu/m3 air.
EXPOSURE TO BIOAEROSOLS IN WASTE TREATMENT INDUSTRIES
In 1993 a German multicentre study was conducted, which identified hundreds of different species of moulds and saprophytic bacteria, including thermophilic actinomycetes, in the air of waste treatment plants.2-4 Also, low concentrations of pathogenic bacteria2 and viruses5 were identified. Exposures of biowaste collectors were substantially lower in recently published studies.6 7 Table 1 summarises the study results and reference measurements.2-8
Orders of magnitude of exposure to fungus spores, total bacteria (excluding actinomycetes), and actinomycetes in the air of waste handling workplaces, and reference measurements (cfu/m3 air)
In most studies, exposure to bioaerosols was estimated by measuring culturable microorganisms (cfu/m3). However, this procedure includes only viable microorganisms, whereas the total count of viable and non-viable cells measured by scanning electron microscopy or fluorescence microscopy is much higher.6 9 These non-viable microorganisms can contribute to health risks from toxic or immunopathogenic effects.
HEALTH EFFECTS OF BIOAEROSOLS FROM WASTE TREATMENT INDUSTRIES
The primary effect of exposure to bioaerosols is often an inflammatory response of the upper airways with congested nose, sore throat, and dry cough often in connection with symptoms of the eyes like redness and tears (mucous membrane irritation), subsiding several hours after the end of exposure.10-12
Toxicoses
Bioaerosols are capable of inducing severe toxic reactions such as the organic dust toxic syndrome, also called toxic pneumonitis.10 13 Endotoxins from gram negative bacteria were identified as a cause of these toxic symptoms and were also associated with acute14-16 and chronic17 18impairment of lung function.
Infections
Increased health risks due to exposure to bioaerosols, mainly infections of the upper air ways and the skin, were reported in workers sorting waste.19 20 Dermatological and respiratory symptoms, including infections, were also found in a study on landfill employees in New York.21
Allergies
Allergens of moulds can trigger type I allergies—such as bronchial asthma and allergic rhinitis—in people predisposed to atopic diseases.13 Induction of extrinsic asthma was reported in workers sorting waste.22 Antigens of fungi and actinomycetes can also cause type III allergy—namely, extrinsic allergic alveolitis —which is also called hypersensitivity pneumonitis. Cases of extrinsic allergic alveolitis in workers handling compost have been reported in Belgium23 and the United States.24 25 One case of a waste collector with simultaneous symptoms of allergic bronchopulmonary aspergillosis and extrinsic allergic alveolitis was described in Germany.26Increased concentrations of IgG antibodies specific to the responsible agents are often found in patients with extrinsic allergic alveolitis, as well as in many symptomless people with high exposures to the antigens of moulds and actinomycetes.27-31
The objectives of the study were the examination of compost workers and biowaste collectors for health effects related to exposure to bioaerosols, the exploration of specific IgG concentrations to moulds and actinomycetes as immunological markers of exposure to bioaerosols, and a possible association with the symptoms and diseases of the waste workers.
Material and methods
The study was performed in the city of Hamburg and in seven small towns throughout Germany from 1996 to 1998. The investigations were performed in the months from July to September of each year.
HANDLING AND TREATMENT OF BIOWASTE
Biowaste was collected from private households (kerbside collection) on a 2 week schedule, and to a minor extent from other sources such as food or fodder processing plants and restaurants. The contents of bins and containers from 110 litres up to 600 litres were dropped into rear loading compactor lorries by hydraulic lifters. The biowaste was transported to composting plants and dumped into bunkers for further processing.
At the composting plants non-compostable materials were removed by manual sorting. The biowaste was mixed with shredded garden waste or hay and straw and piled up in rows by shovel loaders or specially designed vehicles. After the biodegradation process and before delivery, the compost was sieved to exclude non-biological compounds which had not been removed during manual sorting.
STUDY PARTICIPANTS
A total of one female and 151 male full time employees participated in the study. They answered occupational, environmental, and symptom orientated questions in a brief standardised interview performed on the occasion of a preventive physical examination. Work related symptoms in the previous 30 days were registered. The workers were interviewed and examined by physicians specialised in occupational medicine. Diagnoses were coded according to the international classification of diseases, 9th revision, clinical modification (ICD-9-CM) when possible.32 Serum samples for measurement of specific IgG antibodies were taken on the same occasion.
Sixteen compost workers and 24 biowaste collectors who were newly employed in the investigated workplaces served as control subjects. They answered the questionnaire and were examined before taking up the occupation or within the first 3 weeks of employment. The female worker who was employed at a composting plant was excluded from evaluation for statistical reasons. The resulting 151 data sets, including 58 compost workers, 53 biowaste collectors, and 40 control subjects, were processed and analysed further.
MEASUREMENT OF SPECIFIC ANTIBODIES
Serum concentrations of specific IgG antibodies to antigens of seven moulds and four actinomycetes were measured as immunological markers of exposure in 111 waste handling workers and 40 controls, with an indirect immunofluorescence test (IIFT) and an enzyme linked immunosorbent assay (ELISA).
After taxonomic verification of the species, antigens were prepared from pure cultures of fungi and actinomycetes which were identified in the air at compost plants in the German multicentre study. The IIFT and ELISA were developed with these antigen preparations as purified and standardised antigens of most microorganisms were not available from commercial suppliers.33 34 As serum samples of waste workers with known extrinsic allergic alveolitis could not be obtained, positive reactions of the antigen preparations were evaluated with serum samples from five farmers with extrinsic allergic alveolitis. The serum samples which were tested positive with the prepared antigen solutions were pooled and used as positive controls for the ELISA and the IIFT. Chemicals for buffers and compounds not otherwise specified were obtained from Merck (Darmstadt, Germany) and Riedel-de Haën (Seelze, Germany).
Indirect immunofluorescence test (IIFT)
The IIFT was shown previously to be a useful method for the measurement of specific IgG especially against cell wall antigens of moulds.35 36 The IIFT technique was chosen due to its higher sensitivity compared with an ELISA technique based on the soluble antigen fractions of the same moulds.33 The following fungi were included: Aspergillus fumigatus, Aspergillus nidulans, Aspergillus niger, Aspergillus versicolor,Penicillium brevicompactum, Penicillium crustosum. They were predominant in air samples from these workplaces. Aspergillus sydowii was identified in low concentrations (<103 cfu/m3) at several of the plants investigated. This fungus was used for testing of cross reactions with specific IgG of the other aspergillus species. A detailed description of the preparation of fungal antigens and the IIFT antibody determination has recently been published.34
Briefly, the procedure involves the separation of mycelia and spores of moulds from pure cultures grown on malt extract agar plates (Difco Laboratories, Detroit, MI, USA); the resulting antigen solution was lyophilised and stored at −20°C until use. For IIFT the dried material was redissolved in phosphate buffered saline (PBS, pH 7.3), treated with a microdisperser (Ultra Turrax, Braun, Melsungen, Germany), and diluted to a concentration of about 10 μg/ml with PBS, resulting in a homogenous monolayer of fungal material on the microscopy slides.
The antigen solution (20 μl) was pipetted onto specially prepared microscopy slides (bioMérieux, Marcy-l'Etoile, France) and dried for 2–3 hours. Serum samples were log 4 diluted with PBS to concentrations up to 1:1024 and also applied to the slides, which were incubated for 30 minutes at 37°C. After three washing procedures, each slide was stained with Evans blue (1%, bioMérieux) and specific IgG was detected with a fluorescein labelled goat antihuman IgG (Fluoline G, bioMérieux). All examinations were performed by the same laboratory technician and confirmed independently by a second investigator. The highest dilution of each serum sample which gave definite cell wall fluorescence was taken as the end point. Concentrations of 1:1024 were considered positive, and higher dilutions were prepared and investigated likewise.
Enzyme linked immunosorbent assay (ELISA)
The ELISA was developed by Engvall and Perlmann37 and is routinely used to detect specific antibodies to soluble antigens of actinomycetes.38 Predominant species of actinomycetes were: Saccharopolyspora rectivirgula(formerly named Micropolyspora faeni), Saccharopolyspora hirsuta, Saccharomonospora viridis, Streptomyces thermovulgaris. A detailed description of the preparation of actinomycete antigens and the antibody measurement with ELISA has been published previously.33
Briefly, the procedure involves growing of liquid cultures of actinomycetes in synthetic broth AOAC (Difco Laboratories, Detroit, MI, USA) at 37°C (Saccharopolyspora hirsuta,Streptomyces thermovulgaris) or 50°C (Saccharopolyspora rectivirgula,Saccharomonospora viridis) for 14 days; then soluble antigens were derived by ultrasonication and centrifugation of the cultures. The supernatant was dialysed against double distilled water for 24 hours to remove nutrient media and low molecular weight components. Antigens of Streptomyces thermovulgaris were prepared with the double dialysis method of Edwards,39 modified by Treuhaft et al.40
Flat bottomed 96 well microtitre plates (Maxisorp F96, Nunc, Denmark) were coated with these antigens at concentrations of 8–20 μg/ml and incubated overnight at 4°C. After washing and blocking, the plates were dried and stored at −20°C until use. For the assay 100 μl serum diluted 1:800 with PBS was pipetted to each well of the microtitre plates. Controls for unspecific binding (PBS), as well as negative and a pooled positive serum were tested with each microtitre plate. After incubation for 1 hour at 37°C the plates were washed three times, and 100 μl PBS containing 0.1% peroxidase coupled antihuman IgG (Organon Teknika) was added. The plates were incubated again for 1 hour at 37°C and washed three times. Then 100 μl of the substrate buffer containing 0.2% ABTS (2,2-azino-di-(3-ethyl-benzthiazoline-6-sulfonate)) (Boehringer, Mannheim, Germany) and 0.2% H2O2 were added. After an incubation of 30 minutes at 37°C, the optical density of each well was measured with a microtitre plate reader (Spectra, SLT Instruments, Crailsheim, Germany). All samples were analysed in duplicate and measurements were repeated within one week. The variation coefficients within the day were regularly below 20%. However, results from week to week varied up to 50% at maximum. All measurements with coefficients of variation of >20 % were repeated. Values were expressed as means and corrected for differences between control measurements of the singular microtitre plates. Antibody concentrations exceeding 3 SDs of the mean were considered to be high.
STATISTICS
Data were stored with Access 97 (Microsoft, Seattle, USA); descriptive and analytical calculations were performed with Statistica 5.1 (StatSoft, Hamburg, Germany). Graphs were drawn with Statview 4.57 (Abacus Concepts Berkeley, USA) and Excel 97 (Microsoft). The differences between variables from compost workers, biowaste collectors, and controls were analysed with unpairedt test, Fisher's exact test, and Kruskal Wallis test where appropriate. No correction was performed for the confounding effects of smoking as there was no significant difference in smoking habits between the three groups and an exclusion of the smokers (>55% of all workers in each group) would have lowered the statistical power of the study greatly.
Results
The biowaste collectors were significantly younger than the compost workers and had a significantly shorter duration of employment. The mean duration of employment for compost workers was 3 years, whereas biowaste collectors had been employed for only 1.5 years. About 13% of all workers had previous exposure to bioaerosols from farming and working in buildings with cattle, swine, or poultry. One compost worker had simultaneous exposure from working on his own farm in the evenings. Non-significantly fewer biowaste workers than workers from the other groups were exposed to bioaerosols from these sources. The number of current smokers was high compared with data from population based studies in Europe, but there was no significant difference between the three groups. An overview of the group characteristics and confounding factors is given in table2.
Demographic characteristics and confounding variables of biowaste collectors, compost workers, and control subjects
According to the physical examinations, 22 compost workers had up to three health complaints compared with only three biowaste collectors, and one control subject (table 3). Compost workers had a significantly higher prevalence of tracheobronchitis. Mucous membrane irritation, sinusitis, eczema, dermatomycosis, pyoderma, and otitis externa were also diagnosed more often in the compost workers, but these singular results were not significant when compared with the control group. One compost worker complained of typical symptoms of organic dust toxic syndrome. The health complaints of biowaste collectors did not differ significantly from those of the control group. Severe infections were not found, and no cases of extrinsic allergic alveolitis or asthma were reported.
Diseases of the airways and the skin in the waste workers, diagnosed by occupational health physicians (in workers with >1 disease only the leading disease was considered)
Four compost workers reported nausea in the questionnaire whereas no member of the other groups complained of gastrointestinal symptoms. Also, compost workers had a significantly lower prevalence of allergic rhinitis than biowaste collectors and the control subjects. The prevalence of atopic diseases was also significantly lower in the families of the compost workers (table 4).
Gastrointestinal symptoms and atopic diseases of waste workers and their families as reported by the workers
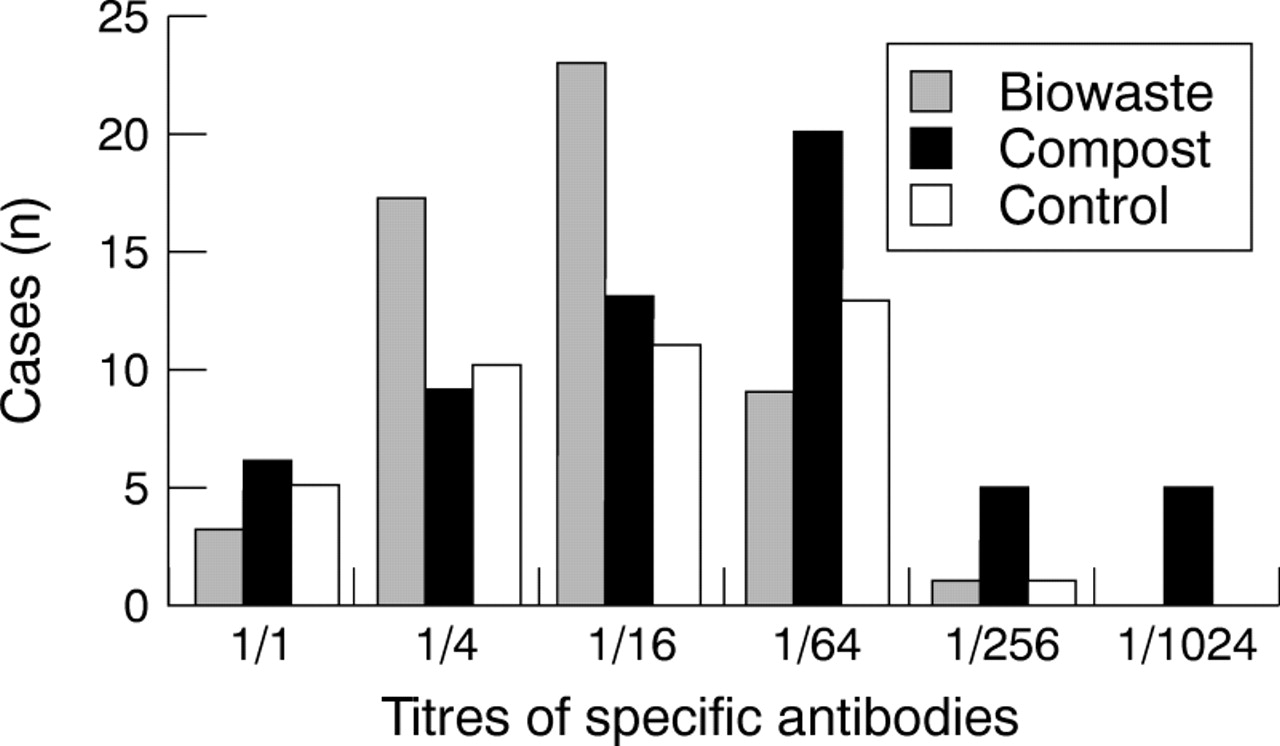
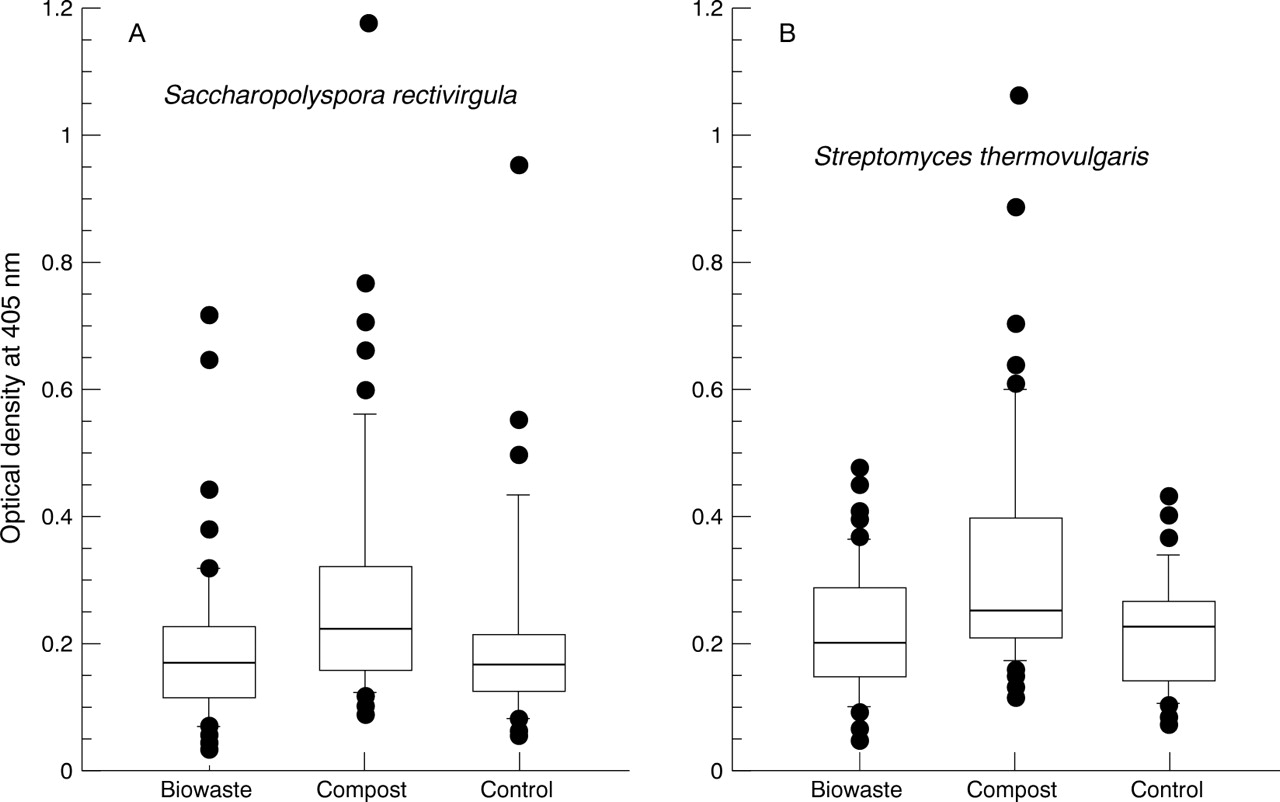
Measurable IgG antibody concentrations were found in over 95% of both the employees and the control group. Significantly higher antibody concentrations to Aspergillus fumigatus were measured in workers at composting plants, whereas antibody concentrations of the biowaste collectors were not higher than those of the control subjects (fig 1). When the six other fungal antigens were tested, compost workers also had higher titres in each singular test compared with biowaste collectors and control subjects (p<0.001 in Kruskal Wallis test for each). Significantly increased antibody concentrations were also obtained for actinomycetesSaccharopolyspora rectivirgula and Streptomyces thermovulgaris in the compost workers (fig2). The concentrations forSaccharopolyspora hirsuta were increased as well (p<0.001 in Kruskal Wallis test), whereasSaccharomonospora viridis showed no significant difference.
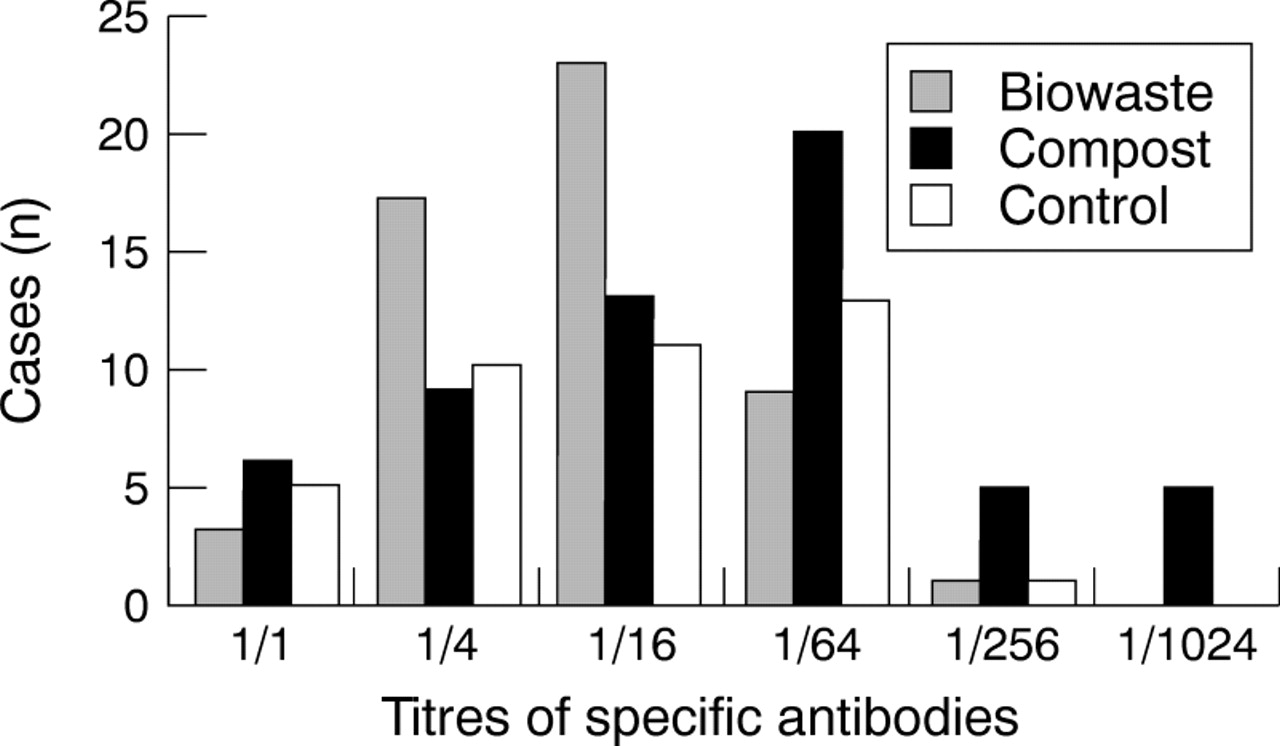
Specific IgG antibody concentrations to Aspergillus fumigatus split by groups of workers and controls, p=0.02 with the Kruskal Wallis test.

Specific IgG antibody concentrations to actinomycetes split by groups of workers and controls, p<0.001 with the Kruskal-Wallis test.
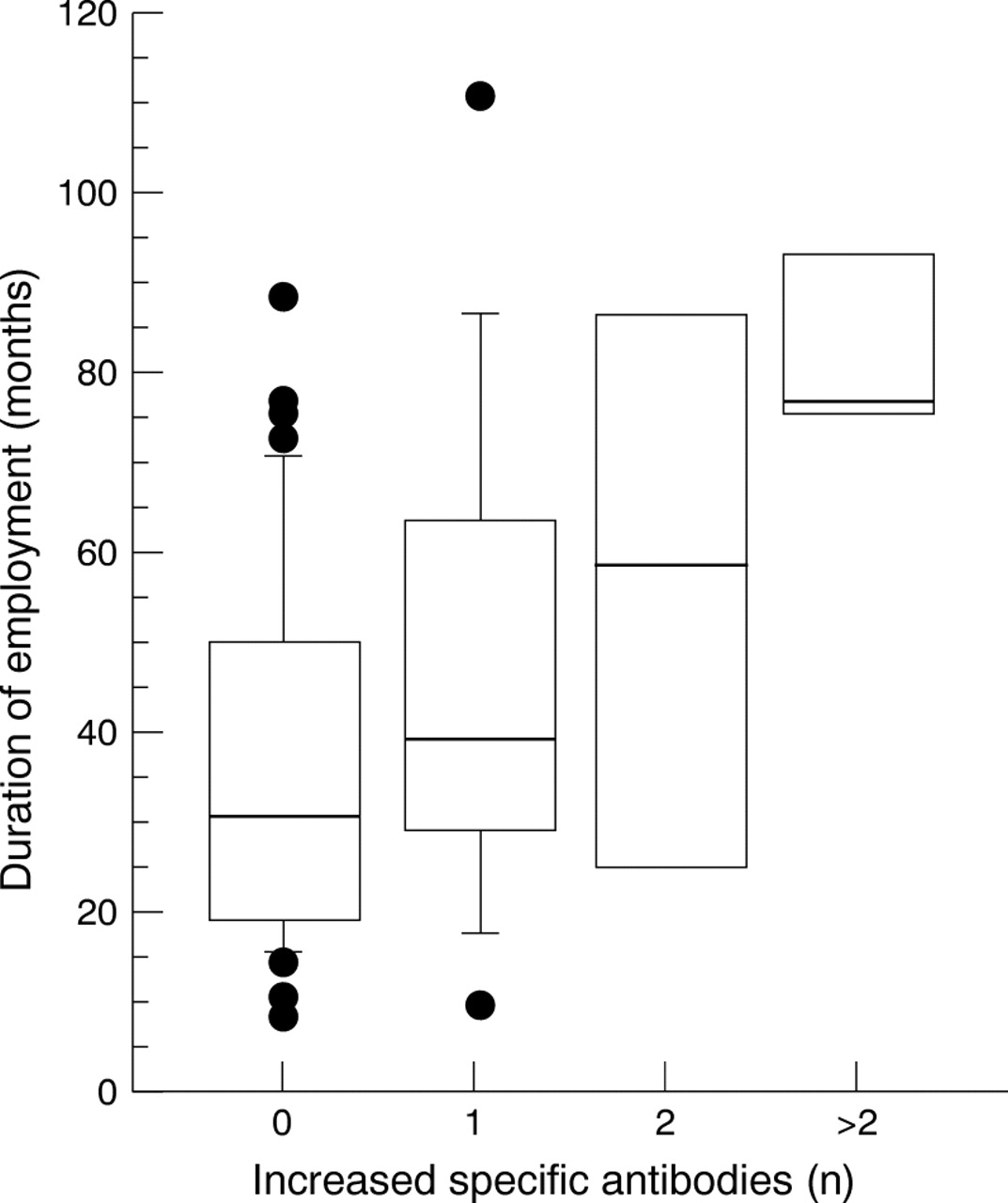
Twenty compost workers had one or several increased antibody concentrations, compared with only three biowaste collectors and one subject of the control group. There was a significant association between diagnosed diseases and increased IgG antibodies in the compost workers (table 5). After exclusion of the compost workers with confounding exposure to bioaerosols (three workers with disease and four workers without) the results were still significant (table 6). No such association was found for the biowaste collectors. Two biowaste collectors and the control subject with increased specific IgG had earlier confounding exposure to bioaerosols. A significant association was also found between the duration of employment of the compost workers and the number of increased IgG concentrations (fig3). No such association was found in the biowaste collectors.
Comparison of the diseases of the compost workers with increased specific IgG concentrations against actinomycetes and moulds (antibody concentrations were considered to be increased when optical density exceeded 3 SD of the mean of the control subjects for actinomycetes and for fungi at titres ⩾1:1024)
Comparison of the diseases of the compost workers with increased specific IgG concentrations against actinomycetes and moulds after correction for confounding bioaerosol exposures (antibody concentrations were considered to be increased when optical density exceeded 3 SD of the mean of the control subjects for actinomycetes and for fungi at titres ⩾1:1024)

{kind=link}
{kind=link}
{kind=link}
Association of the duration of the employment of the compost workers with the number of increased specific IgG antibody concentrations; p=0.03 with the Kruskal Wallis test.
Discussion
Up to now, published information on health risks of compost workers is scarce. In 1984, Clark et aldiagnosed infections and mucosal irritation in workers who composted sludge of waste water treatment facilities.41 The exposed workers reported burning eyes and skin irritation significantly more often than workers without exposure to bioaerosols. In the physical examination, a significantly higher prevalence of diseases of the skin, mainly due to infections, and of the upper airways was diagnosed in the exposed workers. Four exposed workers had an ear infection. One of them had chronic otitis media, requiring a tympanomastoidectomy.Aspergillus niger was isolated from the effluent of the ear. The same worker had signs of a diffuse interstitial lung disease on his chest x ray film. A very similar pattern of symptoms and diseases was found in the biowaste composting workers of this study, except for signs of interstitial lung disease.
Danish waste workers reported a significantly higher prevalence of symptoms of mucous membrane irritation and organic dust toxic syndrome due to sorting rubbish compared with workers employed in facilities supplying drinking water.22 Eight compost workers included in this study reported chronic bronchitis, chronic dry cough, and irritation of the nose. However, the analysis of health complaints of this group gave no significant results, probably due to few subjects. Symptoms of mucous membrane irritation were also reported in waste collectors in Sweden who handled compostable waste and household waste that was not separated.42
In 1980, Lundholm and Rylander reported nausea, headache, and diarrhoea in four of 11 workers in an experimental compost plant.43Nausea was also reported by four compost workers in this study, although this number of symptoms was not significantly higher than in the control group. In an investigation based on 1747 answered questionnaires, Danish waste collectors reported significantly higher prevalences of gastrointestinal symptoms—such as nausea and diarrhoea.44 Gastrointestinal symptoms—such as nausea, vomiting, and particularly diarrhoea—were also found in the two Scandinavian studies.22 42 However, it remained unclear if these symptoms had been caused by infections, toxic compounds, or other adverse effects at the workplaces. Nausea was attributed by some workers to the smell of rotten waste.44 A bad smell was also reported by some biowaste collectors in this study, but was not associated with nausea.
Chronic impairment of pulmonary function due to exposure to bioaerosols was found in workers of the grain processing and animal feed industries and was associated with high endotoxin and total dust concentrations.18 As in our study, similar results have not yet been found in waste handling workers.20 22 42 By contrast, Swedish waste collectors had a significantly higher forced expired volume in 1 second than controls.42 This was interpreted as a healthy worker effect.
The significantly lower prevalence of allergic rhinitis in compost workers than in biowaste collectors and control subjects indicates a selection bias (healthy worker effect) in this study as well. Sigsgaardet al reported underrepresentation of asthma among garbage handling workers.22 Subjects with atopic diseases were also underrepresented in studies on workers exposed to organic dust in the grain processing and animal feed industries18 and in the potato processing industry.45 Therefore, health risks due to exposure to bioaerosols are likely to be underestimated at these workplaces.
The implemented IIFT and ELISA techniques are very sensitive methods of detecting specific antibodies, as IgG concentrations of people exposed solely environmentally (controls) can even be measured.46High exposure to organic dust in workplaces where compost is handled is associated with increased concentrations of specific IgG antibodies to actinomycetes and moulds. Nevertheless, cross reactivity of fungus antigens is likely to occur in the aspergillus group, as titres ofAspergillus sydowii, which was rarely identified at compost workplaces, were also significantly increased in compost workers, and one worker who had titres of 1:1024 for three other Aspergillus species, had a titre of 1:1024 for Aspergillus sydowii.
Specific IgG antibodies are involved in the aetiology of extrinsic allergic alveolitis, but so far none of the investigated subjects with increased specific IgG concentrations in this study had symptoms of that disease. The significant association of the diagnosed diseases of the airways and the skin in the compost workers with increased specific antibody concentrations is probably not cause dependent, but both effects are due to the high exposure to bioaerosols of the workers.
The increased concentrations of specific antibodies to fungi and actinomycetes reflect the results of the high exposures at compost workplaces measured in previous studies (table 1). The absence of significant increases of specific IgG antibodies in the biowaste collectors can be explained by the substantially lower exposures to bioaerosols. However, this result may also be due to the significantly shorter duration of employment, as a association between increased specific IgG concentrations and duration of employment was found in compost workers. Thus we suggest the further evaluation of these variables as immunological markers of exposure to bioaerosols. Whether workers with increased antibody concentrations are at risk for extrinsic allergic alveolitis should be investigated in longitudinal studies.
Acknowledgments
We thank the following laboratory technicians for their excellent assistance: Gesa Homann, Martina Lange, Anke Seeckts, Petra Tucholla, Jutta Utermöhle.