Article Text

Abstract
Background: Much of what is known about the exposure–response relationship between occupational noise exposures and hearing loss comes from cross-sectional studies conducted before the widespread implementation of workplace hearing conservation programmes. Little is known about the current relationship of ambient noise exposure measurements to hearing loss risk.
Aim: To examine the relationship between rates of high frequency hearing loss and measured levels of noise exposure in a modern industrial workforce.
Methods: Ten-year hearing loss rates were determined for 6217 employees of an aluminium manufacturing company. Industrial hygiene and human resources records allowed for reconstruction of individual noise exposures. Hearing loss rates were compared to ANSI 3.44 predictions based on age and noise exposure. Associations between hearing loss, noise exposure, and covariate risk factors were assessed using multivariate regression.
Results: Workers in higher ambient noise jobs tended to experience less high frequency hearing loss than co-workers exposed at lower noise levels. This trend was also seen in stratified analyses of white males and non-hunters. At higher noise exposure levels, the magnitude of hearing loss was less than predicted by ANSI 3.44 formulae. There was no indication that a healthy worker effect could explain these findings. The majority of 10 dB standard threshold shifts (STS) occurred in workers whose calculated ambient noise exposures were less than or equal to 85 dBA.
Conclusions: In this modern industrial cohort, hearing conservation efforts appear to be reducing hearing loss rates, especially at higher ambient noise levels. This could be related to differential use of hearing protection. The greatest burden of preventable occupational hearing loss was found in workers whose noise exposure averaged 85 dBA or less. To further reduce rates of occupational hearing loss, hearing conservation programmes may require innovative approaches targeting workers with noise exposures close to 85 dBA.
- hearing loss, noise induced
- noise
- occupational exposure
- hearing conservation
- occupational medicine
Statistics from Altmetric.com
The relationship between excessive noise exposure and hearing loss has been recognised since ancient times. An 1860 treatise noted that “Artillerymen, blacksmiths, and the blasters in mines often become deaf, and this seems to be dependent upon defective energy of the acoustic nerve, from having been so frequently over excited”.1 Implicit in this realisation was the assumption that the greater intensity of the noise, the greater the expected loss.
Early epidemiological studies of noise-induced hearing loss explored the damage–risk relationship between occupational noise exposure level and the degree of hearing loss. A classic cross-sectional study of female textile workers exposed to noise in the Scottish jute mill industry (without the benefit of hearing protection) found greater loss for individuals working at 100 dBA compared to those working at 90 dBA.2 A number of other cross-sectional studies performed in the 1950s and 1960s provided the basis of consensus documents such as the American National Standards Institute (ANSI) Standard 3.44 that include equations to predict expected hearing loss for a working population exposed at different noise levels.3 In these studies, the use of hearing protection varied widely. Results from these cross-sectional studies were also used to support regulation such as the 1983 US OSHA hearing conservation amendment.4 This regulation set a permissible exposure level (PEL) for noise as an 8-hour time weighted average of 90 dBA. It also set an action level of 85 dBA for enrolling workers in a hearing conservation programme, with hearing protection mandatory when exposures exceed 90 dBA TWA. As a result of the OSHA hearing conservation amendment and similar regulations in other countries, there has been widespread implementation during the last two decades of the 20th century of hearing conservation programmes providing hearing protection and annual audiometry for noise-exposed workers.
A shortcoming of the epidemiological studies used to develop the OSHA standard was a lack of longitudinal dose–response analyses of hearing loss over time, as well as limited availability of audiograms for workers exposed at noise levels below 85 dBA. A subsequent analysis of historical audiometric data (assembled by the National Institute for Occupational Safety and Health (NIOSH) between 1968 and 1972), concluded that there was a need to “collect and analyze data from populations exposed to noise at sound levels below 85 dB to learn more about the shape of the dose response relationship below 85 dB…More recent longitudinal data sets may be useful in examining risk below 85 dB”.5
More recent attempts to further explore the impact of noise exposure on hearing loss in the modern industrial setting have sometimes found, surprisingly, a lack of a dose–response relationship between ambient exposure level and rates of hearing loss, even at higher exposure levels.6 This phenomenon has been attributed to the difficulty in detecting the contribution of occupational noise over background non-occupational exposures in the era of hearing conservation programmes.7 However, such studies did not have access to detailed industrial hygiene data to assess longitudinal exposures to noise.
A major factor complicating recent studies of noise exposure and hearing loss is the use of hearing protection. While information about type of hearing protector worn is sometimes available, short-term field studies of hearing protector effectiveness have consistently shown that such effectiveness varies widely between individuals, making accurate individual estimates of protection impossible.8
We therefore performed a longitudinal cohort study of hearing function among workers in an industry where detailed noise exposure and hearing outcome data were available for recent time periods. The objective of the study was to assess the dose–response relationship between ambient noise level and hearing loss risk in a modern industrial setting where hearing protection was widely employed.
METHODS
We analysed data from Alcoa, Inc. during the period 1990–2004. Alcoa maintains a number of datasets on current and former employees. These include industrial hygiene records, surveillance audiograms, and human resources data on hiring and job transfers. The Yale School of Medicine Human Investigation Committee has approved a protocol for research in an anonymous manner on these datasets. Since the early 1980s, Alcoa has had a policy of enrolling workers in hearing conservation programmes in areas where at least 5% of the noise measurements samples exceed an 8-hour time weighted average of 82 dBA.
Consequently, some employees who receive periodic audiometric testing are working in areas where the median of ambient noise exposure measurements is less than 82 dBA. Furthermore, some Alcoa locations regularly perform audiometry on all employees, including those working in lower noise exposure areas. Since the early 1980s, hearing tests have been performed by certified audiometric technicians in test environments designed to meet OSHA standards for occupational hearing testing. Audiometric testing equipment and procedures were standardised across company locations during the study period as a result of the company-wide hearing conservation programme being under the direction of a single supervising audiologist.
Study cohort
We created a retrospective cohort by identifying hourly workers who were under audiometric surveillance at 10 Alcoa locations. We considered an individual to be under audiometric surveillance at the beginning of the study period if they had at least three audiograms recorded between 1990 and 1996. From among these 12 039 individuals, we selected for further study those who had at least five hearing tests subsequent to 1990 with the last test occurring 8–12 years from the date of the first test. A total of 8669 workers met these inclusion criteria, among whom 6217 had exposure information and questionnaire data allowing for calculation of noise exposure histories and assessment of risk factors for hearing loss (see below). These 6217 individuals constituted the study cohort.
Noise exposure assessment
In order to compare exposures between locations, a set of standardised job titles were determined after review by the company’s industrial hygienist and an ergonomic specialist. We used data recorded in the company’s industrial hygiene database, including all measurements of eight-hour time-weighted averages (in dBA) based on personal dosimetry sampling for each job title, by individual location, to create a job–exposure matrix for noise exposures that provided a mean ambient noise exposure level for each standardised job title during the period of follow-up. Time trend analysis was used to detect temporal trends for noise exposures within particular standardised job titles. If a significant trend was found we used the estimate from the specific years of follow-up. Of the 418 standardised job titles, we found a significant time trend for noise exposures in only 33. We then created job histories for individuals using the human resources database, and linked these job histories with the job–exposure matrix to allow calculation of individual noise exposure histories.
Calculation of noise exposure (Leq)
Personal noise exposure histories were calculated as time-averaged equivalent noise exposure levels (Leq), using previously described methods9 as follows:
Leq,T = A log [(1/T) × (t1 × 10(L1/A) + t2 × 10(L2/A) + … + tn × 10(Ln/A))]
where T is the time duration over which the equivalent level is being determined, A is the exchange rate selected (A = 10 for a 3 dB exchange rate), and L is the noise level for that time duration. For example, an individual who worked 3 years at 90 dBA, 5 years at 88 dBA, and another 2 years at 87 dBA would have a 10-year time-weighted noise exposure level (Leq,10y) = 10 log [(1/10) × (3 × 10(90/10) + 5 × 10(88/10) + 2 × 10(87/10))] = 88.5 dBA. We analysed noise exposure as a risk factor for hearing loss separately as a continuous variable, and as a categorical variable grouping individual noise histories into four categories (<82, 82–84, 85–87, ⩾88 dBA) to allow testing for non-linearity of the dose–response relationship between noise level and hearing loss.
Non-occupational noise exposure and other hearing loss risk factors
Results of questionnaires administered at the time of a hearing test were used to report non-occupational noise exposures and other medical and demographic factors that could contribute to hearing loss. Questionnaire forms and data collection were standardised across company locations and included information on date of birth, race, ear infections, hunting or shooting, family history of hearing loss, noisy hobbies, and other noisy jobs. If a questionnaire response for a particular hearing loss risk factor was “Yes” on at least one occasion, that individual was scored as positive for that risk factor.
Determination of hearing loss
For each individual, the rate of change (dB per year) in binaural average of hearing thresholds for the noise-sensitive frequencies of 3, 4, and 6 kHz was determined by performing a linear regression of all audiometric tests done over the study period. Rates of hearing loss were then compared to the equivalent noise exposures (Leq) for individuals in the cohort. In addition to this continuous measure of hearing loss, an age-adjusted 10 dB standard threshold shift (STS) was determined to have occurred during the study period if the final audiogram showed a 10 dB or more worsening from baseline in the average hearing thresholds at 2, 3, and 4 kHz in either ear, using age corrections based on tables 62-3 and 62-4 of the OSHA Hearing Conservation Standard.4
ANSI 3.44 predictions of hearing loss
To predict the hearing loss due to noise exposure and aging that would be expected for an individual in a particular noise exposure level, we used ANSI 3.44 formulae to calculate the expected hearing loss to noise and aging. The calculated Leq, based on exposure records, was used to compute the expected loss due to noise. Expected age-related and noise-related losses were added in the following manner to arrive at the expected rate of loss:
Total Expected Hearing Loss = Loss due to Noise + Loss due to Aging – (Loss due to Noise × Loss due to Aging/120)
For each individual, consequently, both an expected and an observed rate of hearing loss over the study period could be calculated. For this comparison, we analysed only white males in our cohort since the populations used to derive the ANSI equations were predominantly male and Caucasian. Since previous occupational noise exposure affects the predicted rate of loss in the ANSI equations, we assumed that individuals began employment at age 20 in a job that was at least as noisy as the one they were in at the time of baseline. For example, if an individual was 40 years old at the beginning of our follow-up period, and was working in an area where the equivalent noise exposure (Leq) was 90 dBA, we assumed that he had been working at 90 dBA for the past 20 years.
Examination for possible healthy worker effect
To determine whether individuals experiencing more hearing loss in a high exposure area were more likely to move to a lower exposure area, we first determined the rate of hearing loss over the first five years of the study period in the highest noise exposure group. We selected those workers in the highest and lowest quartiles of hearing loss rates, and then compared over the second half of the study period, whether workers who had the highest rate of hearing loss in the first five years of the exposure period were more likely to move to an area of lower noise exposure in the second 5 years. We also calculated the rate of hearing loss for the individuals excluded from our study. This rate was compared to the hearing loss rate in our study group to determine if self-selection out of the cohort, due to hearing loss, was an issue.
Risk factor analysis
The statistical analysis software SAS Release 8.02 (Cary, North Carolina, USA) was used to correlate measured noise exposure with hearing loss for individual subjects. Simple linear regression was used to analyse the relationship between independent covariates and the dependent variable of change in hearing thresholds. A multiple linear regression model was created to adjust for possible confounding and determine the independent predictors of hearing loss. We also tested for interaction effects between age and occupational noise exposure, baseline hearing status and occupational noise exposure, age and baseline hearing status, and hunting or shooting and occupational noise exposure. A backward elimination procedure was used with a cut-off value of p = 0.05 to select variables remaining in the final model. To further reduce the possible effects of confounding, we performed stratified analyses for the subgroups of younger individuals (age less than 35 at study entry), older individuals, white males, and individuals reporting hunting or shooting.
RESULTS
Demographic and other risk factors for hearing loss
Table 1 shows the demographics for the overall cohort, as well as for subgroups with different noise exposure levels. The study population was predominantly male and Caucasian. Individuals on average had at least one hearing test per year over the follow-up period. Certain risk factors for hearing loss were frequently reported, including hunting and shooting. The baseline binaural average at 3, 4, and 6 KHz was at the upper limits of normal for the overall cohort.
Demographics and hearing loss risk factors, by ambient noise exposure level
As Table 1 shows, the distribution of certain risk factors for hearing loss differed by noise exposure level. For example, workers in the highest noise exposure group were slightly younger, and more females and African-Americans were represented in this group. Individuals in the highest noise exposure group were also less likely to report hunting or shooting or other noisy hobbies. In addition, the binaural average of hearing threshold levels at 3, 4, and 6 KHz at the time of the first test during the study period was also lower for individuals in the highest noise exposure group compared to co-workers with lower levels of noise exposure.
Rate of hearing loss
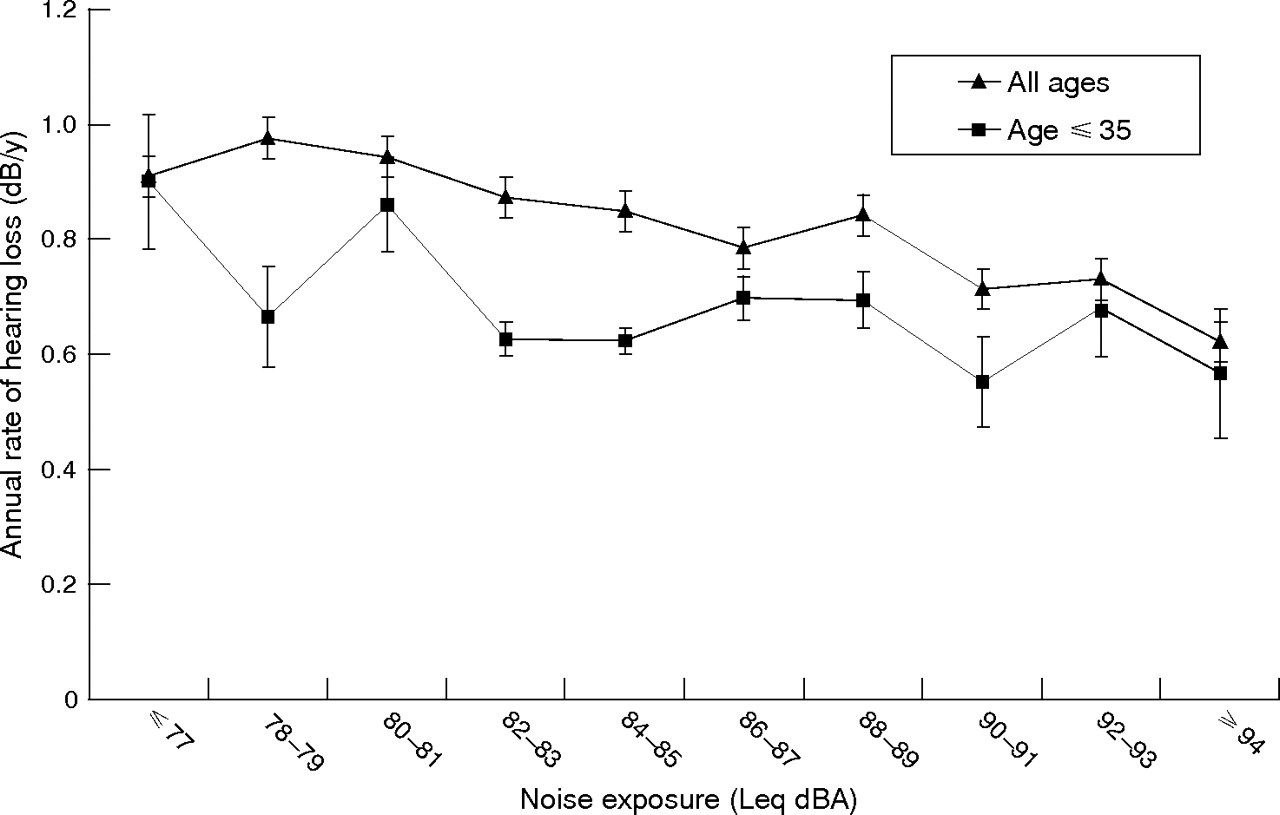
For the study cohort (n = 6217), the mean rate of hearing loss (annual change in average hearing threshold level at 3, 4, and 6 KHz) was 0.86 dB/year. Figure 1 shows the annualised rate of loss for all individuals in the cohort as well as individuals aged 35 or less at inception, according to Leq values for ambient noise exposure. Both the all ages cohort and the younger subgroup show a pattern of apparent decreasing hearing loss rates with increasing measured ambient noise exposure.
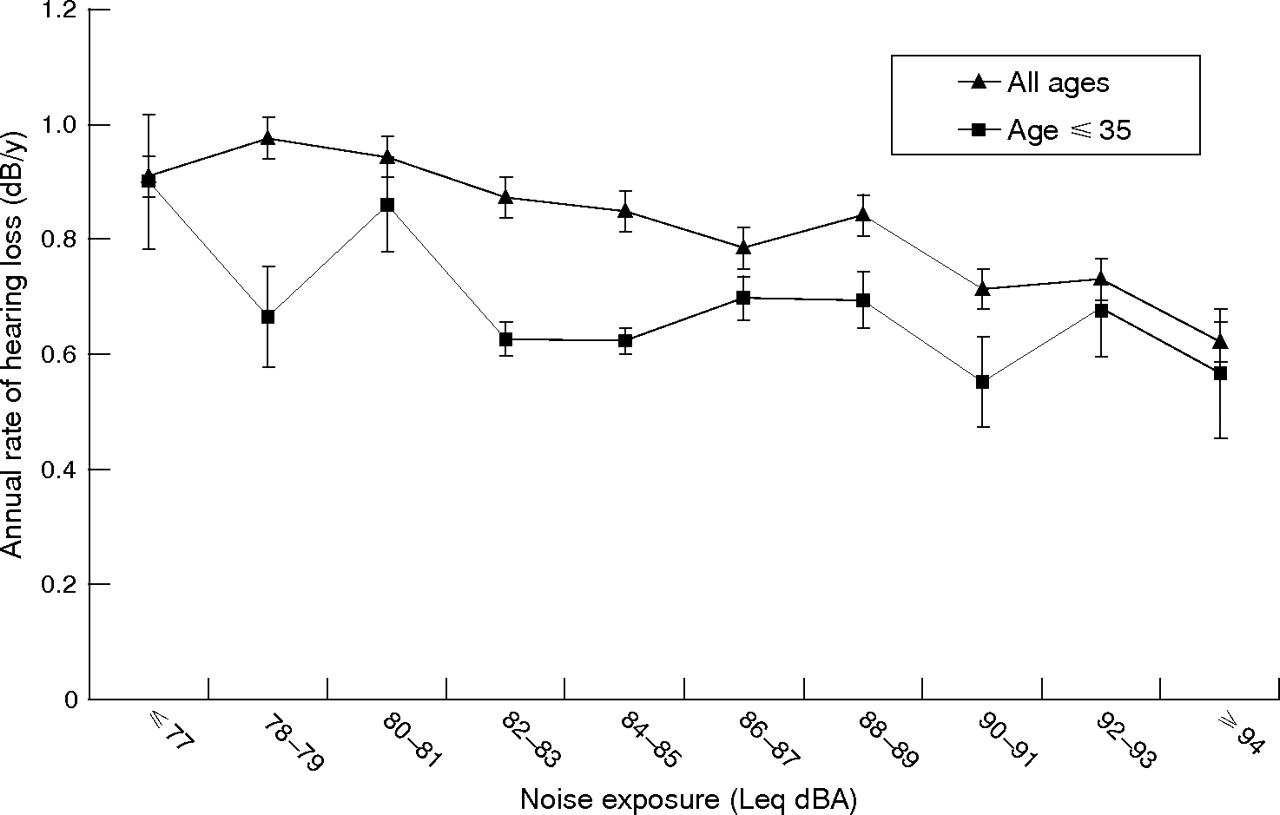
High frequency hearing loss by ambient noise exposure (n = 6217).
Figure 2 compares expected hearing loss rates, as calculated using ANSI 3.44 formulae based on age and equivalent noise exposure level (Leq), for White males in the cohort. At lower noise exposure levels there is good agreement between the ANSI predicted hearing loss and the actual observed rate of hearing loss, while at higher ambient noise exposure levels there is significantly less hearing loss observed than predicted by ANSI equations.

Observed versus ANSI-expected rates of hearing loss, white males (n = 5333).
Bivariate and multivariate analyses
Table 2 displays the results of bivariate and multivariate analysis for the association between various risk factors and hearing loss. For the overall study population, factors remaining significant in the multivariate model included age, male gender, African-American race, hunting or shooting, and family history of hearing loss. Several of the higher ambient noise exposure categories were associated with a significantly lower rate of hearing loss compared to the lowest reference group. In both the younger and older subgroups, there was no increase in risk of hearing loss with increasing ambient noise exposure. For the overall cohort, modelling noise as a continuous variable, there was a significant trend for decreasing hearing loss with increasing ambient noise level (p = 0.03, data not shown).
Bivariate and multivariate predictors of hearing loss
For the entire cohort, baseline hearing level was also associated with an increased risk of hearing loss. A significant interaction was detected between age and baseline hearing level, as the risk associated with baseline hearing declined with increasing age.
To explore whether the observation of lower hearing loss rates with higher ambient noise exposure level could be due to residual confounding by other risk factors for hearing loss, we performed stratified analyses considering either all non-hunters in the study or only white male non-hunters. These two models demonstrated a significant trend of declining hearing loss risk with increasing ambient noise exposure level (p = 0.03 and 0.04 respectively, modelling noise level as a continuous variable; data not shown) after adjusting for covariates.
Healthy worker effect
In an analysis looking for a possible healthy worker effect, we found that the Leq for noise exposure for individuals with the highest quartile of hearing loss during the first 5 years was 83.5 dBA v 84.3 dBA for the individuals with the lowest rate of loss. In the next five-year period, the “high hearing loss rate” individuals had Leq noise exposures of 83.2 dBA v 83.8 dBA for their “low hearing loss rate” colleagues. These differences were not statistically significant, and suggest that no healthy worker effect related to noise and hearing loss occurred in the cohort. Among individuals excluded from the study due to incomplete data (n = 5822), the rate of hearing loss was slightly lower compared to those in the cohort (0.82 v 0.86 dB/y), suggesting that workers with accelerated rates of loss were not self-selecting out of the cohort.
STS rate
Figure 3 shows the rate and absolute number of age-adjusted standard threshold shifts (STS) over the 10-year study period for the entire study cohort. This figure also shows the number of total individuals for each ambient noise exposure Leq level. As the figure demonstrates, the distribution of worker noise exposures over the follow-up period has an average of approximately 84 dBA. The rate of age corrected STS, however, shows a declining trend with increasing noise exposure. Consequently, the greatest number of age-corrected STS occurred among workers exposed below 85 dBA.

{kind=link}
{kind=link}
{kind=link}
Rate and absolute number of 10 dB age-corrected STS occurring over 10-year period, by ambient noise exposure level.
DISCUSSION
Our longitudinal cohort study of 6217 industrial workers tested between 1990 and 2004 found a dose–response relationship trending toward lower rates of hearing loss at higher levels of ambient noise exposure which remained significant in a multivariate regression analysis that adjusted for other risk factors for hearing loss. Even in a subgroup of younger individuals we found no positive dose–response trend. Furthermore, our analysis revealed a striking disparity between observed hearing loss rates and those predicted by ANSI 3.44 for workers in the higher noise exposure categories. As a result, the greatest burden of age corrected STS occurred among workers exposed to noise Leq values at or below the OSHA action level of 85 dBA.
The most logical explanation for these finding appears to be that hearing conservation measures, specifically the use of hearing protective devices, have managed to reduce hearing loss in this population, especially in the higher noise exposure areas of the facilities. At lower noise exposure levels, however, the observed rate of hearing loss appeared to closely match levels predicted by ANSI formulae.
There are several reasons why hearing protection may exert its greatest effect at higher ambient noise exposure levels. While no reliable information on actual use of hearing protection was available for analysis, it is well known that the actual attenuation of noise by hearing protectors varies widely in field settings, related in part to correctness and consistency of use. Workers in higher noise exposure areas may be more bothered by the noise levels and consequently more conscientious about the use of such protection than their co-workers in areas of lower noise exposure. In work areas where noise levels are lower or intermittent, many hearing protectors can give excessive attenuation, leading to interference with communication. As a result, workers in such areas may be more likely to remove hearing protectors in order to communicate. Additionally, in lower noise exposure areas between 82 and 85 dBA, hearing protection may not be required or enforced by management. In Alcoa however, action levels for exposures are determined based on the top 5% of exposure readings. If 5% of exposure levels in a job area exceed 85 dBA, workers are required to wear hearing protection. Therefore, the workers in the current study were generally in areas where hearing protection would have been required.
The finding that hearing loss rates do not increase with increasing measured noise exposure agrees with a previous study which examined workers in a hearing conservation programme that began in 1977, and found no statistical correlation between occupational noise exposure level and hearing threshold shifts.6 However, that study did not examine the exposure–response relationship between different noise exposure categories, and did not indicate whether, as we observed, the hearing loss rates at the highest exposure levels were lower than at lower ambient noise exposures.
The possibility of epidemiological confounding must be considered, since demographic and behavioural risk factors for hearing loss were more prevalent among workers with lower ambient noise exposures. Workers with lower noise exposures were more likely to be white, male, and to report hunting or shooting. However, in the multivariate linear regression models that adjusted for noise, race, gender, baseline hearing level and non-occupational risk factors for hearing loss, the trend toward lower hearing loss rates with increasing noise exposure persisted. Additionally, in stratified analyses including younger individuals, white males, and non-shooters, a similar dose–response relationship was found. Therefore, we do not believe that confounding can adequately or completely account for the observation of less hearing loss at higher ambient noise exposure levels.
Another possibility is that misclassification of noise exposures led to bias in our assessment of the dose–response relationship with hearing loss. It is true that we used job level determinations of ambient noise exposure level to assign individual exposures, and that individual exposure levels almost certainly could be expected to deviate from group medians. Also, for a particular job or work area, the noise exposure measurements show variation, whereas we used the median of such measurements to assign exposure. Any such exposure misclassification, however, would tend to be non-differential across noise exposure levels, therefore biasing the results toward the null. In contrast, we observed a statistically significant negative correlation between hearing loss and measured ambient noise exposure level that persisted in a multivariate model. Therefore, we do not believe that exposure misclassification could adequately explain our study results. Further supporting the validity of our predictive model is the fact that other identified risk factors agree with those found in previous investigations, including a positive risk associated with age, hunting, and male gender, and a protective effect associated with African-American race.10
Another reason for an unexpectedly low rate of hearing loss at the highest exposure levels could be the “healthy worker effect”. This phenomenon is felt to attenuate the exposure–response relationship at higher exposure levels for many occupational exposures such as silica, radon, diesel fumes, nickel, and arsenic.11 For this effect to operate, workers in a higher exposure category who are more susceptible to the effect of a hazard selectively leave employment or move to lower exposure levels, leaving behind a healthier “survivor” cohort in the high exposure areas. Our analysis found the reverse: that workers who were in the top quartile for degree of hearing loss during the first five years had lower ambient exposures than those in the worst quartile for hearing loss, and that in the subsequent five years, individuals who had lost more hearing were less likely to move to lower noise exposure jobs compared to their counterparts who lost the least amount of hearing. Therefore, a healthy worker effect does not seem a likely explanation for our findings. In addition, we found that individuals who were excluded from the cohort did not have higher rates of hearing loss, arguing against self-selection as an explanation of the results.
Main messages
-
Workers with higher ambient noise exposures were found to experience less hearing loss than co-workers in less noisy areas.
-
One explanation could be differential use of hearing protection in noisier versus less noisy environments.
-
The majority of workers who developed standard threshold shifts in hearing had average noise exposures of 85 dBA or less, indicating that more could be done to prevent hearing loss in moderately noisy jobs.
Policy implications
-
To further reduce rates of occupational hearing loss, more attention needs to be directed towards prevention in workers in jobs with noise exposures between 80 and 85 dBA.
-
The current regulatory action level of 85 dBA for enrolment into hearing conservation programmes may not be sufficiently protective.
Our finding that the greatest amount of hearing threshold shifts are occurring among workers with low and moderate ambient noise exposure levels has important implications for established hearing conservation programmes intent on further reducing occupational hearing loss. In our cohort, more than half of noise-exposed employees had calculated Leq exposures less than 85 dBA. Therefore, while their hearing loss rates were close to what was predicted by ANSI equations, the burden of hearing loss attributable to noise exposure, and therefore theoretically preventable through enhanced hearing conservation continues to be great. In fact, the highest rate of age-adjusted STS occurred in workers exposed at those lower ambient noise levels. Consequently, the greatest degree of further preventable hearing loss may be occurring among workers exposed at “lower” ambient noise levels. In these exposure settings, a new set of approaches may be necessary to achieve further reductions in hearing loss. These might include methods of ensuring effective use of hearing protection in areas of intermittent noise exposure, better selection of correctly attenuated hearing protection in such areas, and widening the enrolment criteria for hearing conservation programmes to include workers exposed at ambient noise levels less than 85 dBA.
Acknowledgments
The authors thank Elliott Berger, MS and Robert Dobie, MD for helpful review of earlier versions of this manuscript, and Alcoa Inc. for access to company databases. Jessica Duda assisted with data preparation. This study was funded in part by grants from CDC-NIOSH (1 R01 OH07724-01) and the Network on Socioeconomic Status and Health, John D and Catherine T MacArthur Foundation.
Footnotes
-
Published Online First 14 September 2006
-
Competing interests: Dr Rabinowitz, Dr Cullen, Mr Galusha, and Mr Slade provide consultant services to Alcoa Inc. Ms Dixon-Ernst is the corporate audiologist for Alcoa Inc.