Article Text

Abstract
To achieve a common base for understanding work related eye complaints in the office environment, it is necessary to merge approaches from indoor air science, occupational health, and ophthalmology. Based on database searches, it is concluded that precorneal tear film (PTF) alteration leads to eye complaints that may be caused by: (1) thermal factors (low relative humidity; high room temperature); (2) demanding task content (attention decreases blinking and widens the exposed ocular surface area); and (3) individual characteristics (for example, tear film alterations, blinking anomalies, gland dysfunctions, and use of contact lenses). These factors and conditions are able to progressively increase water evaporation and faster thinning of the PTF, which causes dryness and dry spot formation on the cornea, possibly followed by corneal and conjunctiva epithelial alterations and eye complaints. Another possible cause of eye complaints is certain irritating chemical compounds, in addition to oxidation mixtures that are formed in reactions between ozone and unsaturated organic compounds (alkenes). The effect may be exacerbated by low relative humidity.
- APTF, altered precorneal tear film
- BF, blinking frequency
- BUT, break-up time
- CL, contact lens
- LL, lipid layer
- OS, ocular surface
- PTF, precorneal tear film
- RH, relative humidity
- VDU, visual display unit
- VOC, volatile organic compound
- eye irritation
- occupational asthenopia
- chemical irritants
- indoor air quality
- ocular surface physiology
- microclimate
- VDU work
Statistics from Altmetric.com
- APTF, altered precorneal tear film
- BF, blinking frequency
- BUT, break-up time
- CL, contact lens
- LL, lipid layer
- OS, ocular surface
- PTF, precorneal tear film
- RH, relative humidity
- VDU, visual display unit
- VOC, volatile organic compound
- eye irritation
- occupational asthenopia
- chemical irritants
- indoor air quality
- ocular surface physiology
- microclimate
- VDU work
Eye complaints, such as burning, dryness, gritty, itchy, and stinging feeling, scratchiness, soreness, blurry vision, strain, etc (“eye irritation”), are commonly reported symptoms in epidemiological studies of the indoor environment.1,2 These symptoms, in particular perceived “dry eyes” and related ocular surface effects (also called “ocular discomfort”), are major eye complaints treated by ophthalmologists.3–5 Indeed, it has been concluded in one review that, “It was unclear just how often one should expect symptom-free individuals”.6 “Tired and strained eyes” have been reported to be the most common cause of disruption of office work, followed by mental fatigue and headache7 (cf. Begley et al8). Associations between complaints and work duration have been identified in visual display unit (VDU) workers.9,10 However, the pathogenesis of eye complaints is not well understood, mainly because there is no common terminology of the numerous kinds of symptoms as well as no consensus on the exposure evaluation procedures.
Eye complaints such as “dry eyes”, have been associated with occupational factors, such as office equipment,11 and indoor air pollution.12–14 Such eye complaints may be caused by alteration of the precorneal tear film (PTF) that protects the outer eye from environmental factors. “Alteration” in this paper is the process of thinning of the PTF followed by rupture (that is, PTF break-up) due to environmental conditions—mainly thermal factors (high room temperature, low relative humidity (RH)), and indoor pollutants.
The stability of the PTF is inter alia influenced by individual physiological characteristics such as the composition of (1) the outer lipid layer (LL), (2) the underlying water layer, and (3) the innermost layer of mucin.15 Clinical tests to evaluate the PTF integrity and stability are the “break-up time” (BUT, sec) and the thickness (μm).16,17 Eye blinking and tear secretion appear to be essential for the maintenance of a “normal” PTF,5,15,18,19 and are also important for achieving constant high quality retinal images.20,21
It is important to understand the physiological factors that are responsible for eye complaints in office environments with specific attention to VDU work, for example, in which the visual and cognitive demand can be high. In this regard, it is worth noting that “eye complaints” or “occupational asthenopia” among office workers have a multifactorial origin, including the possible overloading of accommodation and convergence caused by prolonged near work.22
The causes of eye symptoms remain unknown. They could be the result of PTF effects such as dryness derived from: (1) an increased water loss by evaporation due to thermal and/or other indoor environmental factors, (2) an altered PTF (APTF) caused by hyposecretion of tear fluids (because of gland dysfunctions), or (3) a trigeminal nerve ending stimulation by indoor pollution facilitated by an APTF.
The purpose of this review is twofold: firstly, to merge approaches derived from indoor air science, occupational health, and ophthalmology in order to achieve a common base for understanding work related eye complaints in the office environment; and secondly, to analyse if, and eventually how, in office workers:
-
Blinking alterations could play a role in increased PTF alterations.
-
PTF alterations are associated with some specific environmental factors, such as low RH and/or high room temperature and air velocity.
-
Indoor air pollution could cause PTF alterations and/or eye symptomatology.
Main messages
-
To avoid ocular surface dryness (that is, precorneal tear film break-ups and corneal dry spots), it is important, in particular during demanding visual tasking, for example, VDU work, with specific regard to computer design activities such as CAD-CAM, CAT, etc, to depress water evaporation by allowing sufficiently high periocular relative humidity.
-
Normal blinking and a small exposed ocular surface minimise water loss and early rupture of the precorneal tear film.
-
Sources of volatile chemically reactive compounds should be kept under surveillance, in particular in the presence of ozone.
-
In low humidity environments, where highly demanding visual/cognitive work is carried out, subjects suffering from ocular surface pathologies and/or contact lens wearers should be considered as more “susceptible”. These individuals should be included in specific health surveillance programmes according to Council Directive 90/270/EEC.
METHODS
Researchers with experience in indoor air science, occupational health, and ophthalmology have reviewed the indoor climate literature about eye irritation and related eye symptoms/signs. The search strategy also included physiology of the outer eye: precorneal tear film, tear physiology, blink frequency/rate, break-up time, dehydration, dry eyes, dry spots, epithelial damage of conjunctiva, gland (meibomian, lacrimal, goblet) dysfunctions, and objective eye sign measures. Search of the epidemiological literature focused on associations between eye irritation symptoms/signs and indoor air pollution, including human exposure studies with indoor pollutants. Exclusion criteria were within refractive related complaints, work related musculoskeletal disorders, lighting, and psychosocial and psychological factors. The search was carried out using the following databases: PubMed/Medline (from 1990) and ISI Web of Knowledge (from 2000).
FACTORS INFLUENCING EYE BLINKING
Distribution of the PTF
The PTF is essential in defending the ocular surface (OS) from environmental exposure, thus minimising injury. The distribution of the PTF is a coating process achieved by a narrowing of the palpebral fissure, proceeding from the lateral canthus towards the medial canthus during each blink.15,23 The PTF integrity depends on the complex interaction of the blink process with tear composition. Blinking is also important in mechanically removing deposited particles and cellular debris.24,25
Blinking types and dependencies
Blinking can be classified into three categories.26 Voluntary blinking is the result of a conscious decision to close and open the eyelids. Involuntary (spontaneous) blinking, however, occurs without any external stimulus and at a fairly constant rate; this probably arises from the activity of a central “blink generator” in the brain, although the neural basis in detail is not fully understood (cf. Acosta et al27). Reflex blinking is a rapid closure movement of short duration as a response to a variety of external stimuli, mainly visual or ocular, but also auditory, cognitive, trigeminal, or visual stimuli, as well as other motor behaviours. Reflex blinking is dominated by trigeminal stimulation.26 The major determinants of the blinking frequency (BF) at rest are extrinsic factors, such as dehydration as a result of water loss, arising from local PTF conditions of the cornea and conjunctiva and stimulation of their sensory receptors caused by task related and environmental factors.27–29 Visual tasks, temperature, RH, and lighting conditions also influence the BF (cf. Wolkoff et al11).
About 80% of blinks are complete, in which the descending upper eyelid covers more than two thirds of the cornea; about 18% are incomplete, in which the descending eyelid covers less than two thirds of the cornea; less than 2% are twitch blinking (flutter).30–32 BFs are individual with mean frequencies from less than 2–3 up to 20–30 blinks/min, but typically about 12–20 blinks/min if the subject is at rest under neutral environmental conditions.26,33–35 However, blinking is influenced inter alia by a number of individual and task related factors, for example, attention, task complexity, gaze direction, emotional state, and verbalisation36 (see table 1). For example, visual tasking—that is, work difficulty, complexity, and cognitive overload, lowers the BF. There appears to be an inverse relation between difficulty of task and BF. In addition, visual tasking competes with other external influences and stimuli such as high air velocity, and overriding may occur.27,35 Conversation on the other hand may result in some increase of the BF. The latter is usually highest for difficult tasks (see table 1).
Effects on blink frequency as function of mental and visual tasks
It has to be noted, however, that each subject has his/her own specific “blink pattern” with intra- and inter-individual daily variability of varying degree.33,35,37 The daily variation of the BF depends on a number of visual and environmental conditions, which may positively and negatively contribute to the summed BF.11,38
In order to compensate for the deterioration of visual quality by APTF, BF is likely to be lowered. The price to be paid for the maintenance of such a quality could be one of the possible contributions to the development of ocular/visual disturbances (cf. Piccoli22). Sustained BFs above the higher peaks of the normal range could indicate either environmentally induced eye irritation or a highly aroused mental state in normal subjects.35
EFFECTS ALTERING THE PTF
Water loss/dehydration of the PTF (aqueous tear deficiency)
Evaporation of water molecules from the intact PTF occurs by internal diffusion (that is, LL acts as a barrier) to the ambient air, when the RH is lower than 100%—that is, driven by the “evaporation driving force”.39 External diffusion (no barrier as opposed to internal diffusion) will dominate the water evaporation from an APTF. High air velocity will enhance the evaporation of water, resulting in a faster temperature decrease, especially at the cornea (see below). High air velocity (>1 m/s) may result in a slight increase of BF during resting conditions;28 this, however, can be overruled by visual tasking; for example, game playing or VDU work.27 In the latter case, VDU work becomes a special case in which BF decreases, becoming consistently overdue as a result of cognitive functions (effort). This causes BF to fall below “average” and possibly a widening of the exposed cornea, thus resulting in an increased water evaporation, possibly followed by ruptures as a result of an APTF (cf. Golding et al40 and Miller et al41).
High RH reduces the BF,42,43 and an inverse proportionality regarding the ambient temperature has been observed.43 In addition, BUT was found to be lower in dry and warm environments compared to that of cold and humid environments44 (cf. Berke45); similarly, BUT was found to be inversely associated with increasing temperature among female nurses.46 This, of course, may possibly have been the result of an associated lower RH. The findings support the fact that APTF recurs under conditions favouring water loss. For example, it was found in a crossover study in public office buildings that a 1°C decrease in temperature (within 22–26°C) correlated with 19% decrease of the mean value in severity of eye complains (dry, itching, irritated).47 The mean prevalence for eye complaints increased slightly from morning to afternoon in public buildings,8,48,49 which is compatible with the observation that the LL thickness decreases during an office working day,50 concurrently with an increase of the room temperature.51 Note that the intensity of symptoms among dry eye patients is significantly greater in the evening than in the morning.8 It is of note that BUT similarly decreases and eye irritation increases over time under controlled climate conditions of clean air.52
Increased water evaporation from the OS results in cooling of the cornea and the lids, in particular during condition of low BF, low RH, and upgaze, or combinations thereof.53,54 Rapid cooling appears to be related to APTF, possibly due to its inability to retard the evaporation, thus stimulating blinking.55 For example, subjects whose cornea showed a slower cooling following a blink showed a greater capacity to avoid blinking for a prolonged period of time.56 On the other hand, the corneal temperature in dry eye patients varied less than that in normal control subjects, possibly because of less water evaporation from the PTF of dry eye patients.54 This agrees with the proposal that thermosensitive cold fibres in the cornea may initiate reflex blinking by cooling.32,54 Stimuli which modify neural activity in the sensory fibres of the cornea and conjunctiva, such as increased evaporation or additional humidification, may change the involuntary BF. Evaporation of water has also been reported to increase in dry eye patients, accounting for the majority of the water loss,57 partly because it “pulls ahead” the tear secretion.58 In addition, dry eye patients generally have lower BUTs and higher surface tension of the tear liquid in contrast to normal eyes.59
Use of contact lenses
Dry eyes, redness, and grittiness are common complaints among contact lens (CL) wearers and are reported more frequently than among non-wearers;35,60–65 in addition, loss of optical qualities (for example, blurred vision) is often reported.21,66 The symptoms are more frequent in the evening than during the day.67
Indeed, it has to be noted that, once positioned, a CL separates coarsely the PTF tissue into a pre-lens and a post-lens fraction, producing two important structural and functional modifications: the disappearance of mucine in the pre-lens fraction and the disappearance of the LL in the post-lens fraction. Recently this has been objectively evaluated by interpherometry investigations.68 CL wear compromises the PTF stability, and the disappearance of the LL in the post-lens fraction, which causes an increase of water evaporation,69–72 followed by a corresponding increase of the physiological osmolarity, responsible for OS damage.65,73–75 These PTF alterations are consistent with the symptoms and disturbances reported in the occupational health and safety and indoor climate literature, and support the fact that some CL wearers are more susceptible than non-wearers to some specific adverse environmental conditions (cf. Wolkoff et al11), including enhanced sensitivity to low temperature and RH.69,76
Moreover, CL wearers have different PTF characteristics compared to that of non-CL wearers or intolerant CL wearers.77 For example, in a study of soft-CL wearers divided into complete and incomplete blinkers, the incomplete blinking group showed a significant decrease in the dehydration level of the inferior part of the soft lenses compared to that of the control group with low incomplete blinking. Consistent fluorescein staining of the inferior part of the cornea was observed in the incomplete blinking group. This group also suffered more from discomfort and dryness, including more lens deposits,78 (cf. Abelson and Holly30). It is of note that BUT was the same in both groups.
CONSEQUENCES OF BLINKING ANOMALIES
Ruptures of the PTF
The main consequence of incomplete and reduced BF is a significant increase of APTF.45,64,79 APTF films alter faster and/or more severely than normal ones.23,45,70,80,81 APTF consequent to a incomplete blinking is more prone to ruptures (staining areas into the “inferior paralimbal” part of the cornea). There are corneal sub-regions that are much thinner than others. For example, more than 10-fold reduction of the PTF thickness in 40 seconds has been modelled near the inferior lid.23 A critical thickness of PTF of 7 μm has been estimated to result in moderate to severe ruptures.70 Deliberate forceful blinking, on the other hand, was found to increase the thickness of PTF.82
In some subjects PTF thinning leads to its rupture before the next blink, and dry spots are thus formed, exposing the bare corneal and bulbar conjunctival epithelium to, for example, chemical pollutants for a limited period.83 Indeed, in normal subjects, the BUT exceeds the interval between blinks—that is, the PTF permanently covers largely all the cornea. Incomplete blinking results in less effective redistribution of the PTF; this results in more frequent and wider ruptures (that is, more leaky), in particular over the inferior part of the cornea (that is, where the upper eyelid reaches its lowest descent point).83–88
The water loss may be fourfold faster from an APTF.53 It has been proposed that enhanced thinning is preceded by evaporation.41 Note that BF and BUT are weakly associated,32 even though BUT and water loss are not necessarily inversely correlated in normal subjects,89 but are in dry eye patients.90 In addition, the evaporation is increased in dry eyes which accounts for the majority of water loss;57,91,92 this is possibly a result of a thin PTF.69,93 PTF not only becomes thinner at reduced BF, but also by a large exposed OS. VDU work or playing video games result in reduced BF, an enlarged exposed OS area, and a significantly greater water loss than during relaxed conditions or downward gaze (cf. table 1 in Wolkoff et al11). These circumstances can finally result in a reduced BUT.45 Thus, the combined effects of reduced BF, incomplete blinking, and wider OS lead to water loss, which may not be physiologically compensated for.
Hyperosmolarity of the PTF
PTF production (in terms of “quality” and “quantity”), lacrimal duct run-off, and water loss from the PTF are balanced by the homoeostatic mechanism to control and maintain the OS integrity.94 Tear hyperosmolarity (that is, above the physiological level of osmolarity, which is approx. 310 mOsm/l) is in part a consequence of the high rates of water loss and inadequate tear secretion from the lacrimal glands.95 The rate of water evaporation and osmolarity were found to be positively correlated, and both have also been found to be positively related to APTF,96 so the effect of evaporation on tear osmolarity is significant.94
It has been modelled how important the function of the LL, produced by the meibomian glands, is in maintaining normal PTF composition. In fact, an alteration of LL produces on PTF a domino effect consisting of higher water evaporation, increase of osmolarity, goblet cell sufferance, glycocalix disorder, and finally, dry spot formation.18,97 This is particularly evident in patients with meibomian gland dysfunctions, because in these patients the highest correlation between osmolarity and lipid function was found. Those with a high lipid volume were better at maintaining a low evaporation rate than those with a low lipid function—that is, a thin LL.94
EFFECTS OF INDOOR POLLUTION (VAPOURS AND PARTICLES) ON THE PTF
The PTF contains proteins with antibacterial activity, nutrients, lubricants, vitamins, and other substances to protect the OS against damage caused by, for example, microorganisms, ozone, and radicals.34,98,99 It has been inferred, but without further specification, that environmental factors may influence the PTF stability.35,87
It has previously been postulated that (prolonged) exposure to environmental pollution might cause eye complaints.12–14 In particular, lipophilic and/or surface active pollutants (for example, detergents) have been hypothesised to cause thinning of PTF, finally resulting in ruptures and epithelial alteration of conjunctiva, called “pollution keratoconjunctivitis”.14 According to present knowledge, exposure to lipophilic or hydrophilic indoor volatile organic compounds (VOCs) may alter the PTF at industrial concentration levels. APTF has been observed for exposure to decane100 and propylene glycol,101 representative of a lipophilic and a hydrophilic VOC, respectively. However, a number of glycol ethers and esters have not been shown to cause APTF at industrial concentration levels.102–105 Similarly, a mixture of 22 different VOCs dominated by butyl acetate and toluene did not alter BUT at a total level of 24 mg/m3.106 Office environment VOC concentrations are generally 3–4 orders of magnitude lower than industrial levels or occupational exposure limits. Further, there is no convincing evidence that either common (chemically non-reactive; for example, toluene, butyl acetate) VOCs or particles at typical indoor levels result in an APTF, and are able to cause eye complaints (cf. Wolkoff et al,11 Schneider et al107). At present, it appears that oxidation products from the reaction between certain unsaturated VOCs (that is, alkenes), like monoterpenes, that are used in household products as solvents or fragrances (for example, in air fresheners) and ozone may contribute to eye irritation,37 in addition to the well known eye irritants, for example, formaldehyde and acrolein.108
Smokers show a higher prevalence of eye complaints than non-smokers.2 In addition, BUT is lower among smokers compared with non-smokers, thus indicating that tobacco smoke causes APTF.109 Similarly, people living and working in more polluted environments have lower BUTs than people from less polluted areas,12 inferring that urban pollution causes APTF. A decrease of self-reported BUT has been attributed to certain VOC emissions from degraded polyvinyl chloride flooring, in particular 2-ethylhexanol.110 However, it is unlikely, based on present knowledge, that the low concentrations measured result in either APTF or trigeminal stimulation (cf. Emmen et al,102 Iregren et al105). It is possible, however, that access of VOCs to the corneal epithelium sensory receptors (nociceptors) would be increased by an APTF.15
An increase of the prevalence of eye complaints among asthmatic children has been associated with increased ozone concentrations and high temperature, including particles (<13 μm),111 and eye irritation among subjects with obstructive airway disease has been found to be related to ozone levels.112,113 Apparently, ionisation with negative ions relieved dry eye symptoms and increased the interblink interval in a hospital.114 It was hypothesised that the positive effect could be reduction of respirable particles. However, in a recent double blind crossover study at low levels in public office buildings, a 94% reduction of particles (<3 μm) was not associated with reduced eye symptoms.47 Neither is there convincing evidence that indoor particles by mass, per se, are causative of eye symptoms,11,107 except for special cases reported in a review.11
CORRELATION BETWEEN PERCEIVED EYE COMPLAINTS AND ALTERATIONS OF THE PTF
A number of office related eye complaints/disturbances (for example, occupational asthenopia, eye irritation, strained eye, visual fatigue, ocular discomfort, etc) have been reported in indoor field investigations. From a medical point of view, they have been characterised by specific symptoms/signs such as: burning, redness, gritty and itchy feeling, lacrimation, etc, and blurred vision, double vision, light intolerance, etc; however, information about location, duration, and onset is generally not reported,58 and neither is the use of certain medication, which acts as a confounding factor.24 Although positive associations with near work duration have been established, associations with the ophthalmic clinical picture are less clear. One reason for this is the wide range of “eye irritation” symptoms from mild to severe; for example, the “dry eyes” symptom appears only in certain indoor environments and generally under multifactorial conditions (as opposed to the disease “dry eyes”). Patients diagnosed with asthenopia of unknown aetiology may in fact have dry eyes.115 Dry air is another common complaint in indoor environments to consider.2 This may well be associated with eye complaints and not necessarily the RH, per se.
There appear to be many different mechanisms associated with the increase of office eye symptomatology (see table 2), which could either have the same origin (overlapping symptoms) or act synergistically. For example, a few studies have shown clusters of symptoms, such as “dryness, smarting, and itching”116 and “itching, irritating, grating, and sandy”.117 One study has shown that “external symptoms”, such as burning, irritation, tearing, and dryness were located in the front and inferior part of the eye, while “internal symptoms” comprised ache, pain, strain, and headache located behind the eyes.118 Among dry eye diagnosed patients, dryness and soreness were the most frequently reported symptoms of eye irritation.119
Some specific symptoms and their hypothesised pathogenesis
A number of identified correlations between reported eye symptoms and objective measures of an APTF, both in human exposure studies with indoor pollutants and in office investigations have been reported.11 However, there are also studies where such correlations are absent.6,11,16,120–122 This is comprehensible in view of both conceptual and perceptual overlap of reported symptoms. For example, it has been observed that occasional dry spots (observed by fluorescein staining of the PTF) occurred during the blink interval in about 50% of apparently normal patients. In less than 50% of patients with apparently normal eyes, dry spots were observed to occur consistently after blinking.86 Some of these patients with dry spots and epithelial alteration of conjunctiva (observed by lissamine green staining) neither blinked immediately after the spot formation nor expressed discomfort. Generally, however, the development of symptoms coincides with APTF more often than situations where it does not (for example, Wieslander et al;101 see also references in Wolkoff et al11). However, the observed location of dry spots may not correspond to the perceived location of symptoms such as smarting and stinging.123
Enhanced water loss and inadequate tear production lead ultimately to an APTF, hyperosmolarity, and corneal and conjunctival epithelial damage. This could obviously result in severe ocular/visual discomfort. For example, epithelial alteration of conjunctiva was significantly increased among female subjects carrying out typical office work for six hours in a simulated office environment (laser printer and photocopier) compared to exposure under similar, but clean environmental conditions.124 During their VDU work that included reading, it is likely that BF was reduced and OS enlarged, thus leading to a poor PTF redistribution and enhanced water loss. Indeed, reduced BF has been associated with reporting of increased discomfort, which further increased during exposure to high air velocity.27 The significant increase of reported dry eyes in the simulated office environment may thus be at least partially explained by enhanced PTF water loss. This has been confirmed in a study about VDU work in controlled environments of low RH125 (cf. Korb et al126). In addition, faster evaporation results in faster stimulation of cornea by cooling, which may be perceived as uncomfortable (that is, discomfort). However, the eyelids appear to be more sensitive than the cornea itself.127 Under these circumstances, the main cause of eye discomfort is increased activity of the sensory nociceptive terminals in the exposed OS. However, the discomfort experienced is unable to overcome the strong inhibition of involuntary and reflex blinking mechanisms during, for example, PC games/tasks.27,39,71
It has been reported that the increase of the RH from 35% to 43% had no effect on self-reported BUT (measured as the time before discomfort/pain is perceived after a blink with lids open), although the perception of dry air was reduced significantly128 (cf. Nagda et al129). One explanation could be that the increase of RH results in less water loss, possibly resulting in less cooling effect of the cornea. The above agrees with the observation that increased periocular RH resulted in a substantial increase of the thickness of the PTF that also relieved symptoms as a result of APTF;126 similarly, the use of glasses with side covers and moist inserts has a stabilising effect in dry eye patients by increasing the interblink time and reducing the blink duration.126,130,131
It appears that the intensity of eye symptoms among office workers increases during a working day,8,48,49 and in particular for CL wearers in the evening.48,49,67 Measurements showed some thinning of the LL in office workers during a working day.45,50,132 One explanation for the eye symptomatology increase could be the less effective redistribution of the PTF as a result of the increased cognitive effort or difficult visual tasking that decreases the BF. Additional explanations for the eye symptomatology increase could be the overloading of accommodation and convergence, and poor lighting design.133 Moreover, psychological fatigue (drowsiness) results in a longer blink duration—that is, a slower eyelid opening;134 it has also been suggested that this kind of fatigue results in more blink incompleteness.135 Since the PTF is formed during the opening phase of a blink, the upper lid velocity determines the thickness—that is, a slower upper lid movement leads to a thinner PTF.23 Eventually, this will result in an enhanced APTF, which could result in ocular/visual disturbances. Another explanation is additional water loss and reduction of the BF during a working day.47 Some authors have observed lower BUTs in warm and dry environments.44,46 The aqueous tear production also varies throughout the day, depending on stimuli through a reflex loop connecting the OS with the lacrimal glands (cf. Rolando and Zierhut18). Likewise, the meibomian production has its maximum just after wakening.136
It is clear that the perception of eye symptoms during the initial period after entering an office environment depends on both the RH and the air quality of the outdoor environment experienced during commuting and reflected in the stability of the PTF (cf. Saxena et al,12 Paschides et al44). This is important to consider in experimental human exposure studies as well as in clinical examinations.
Finally, allergic conjunctivitis associated with decreased BUT and less goblet cell density,137 in addition to other APTF conditions,138 adds to the overall dry eye prevalence.66,139
CONCLUSIONS
The purpose of this review is to identify some of the environmental (for example, thermal, and chemical) factors that cause alterations to the eye, resulting in complaints in office-like environments.
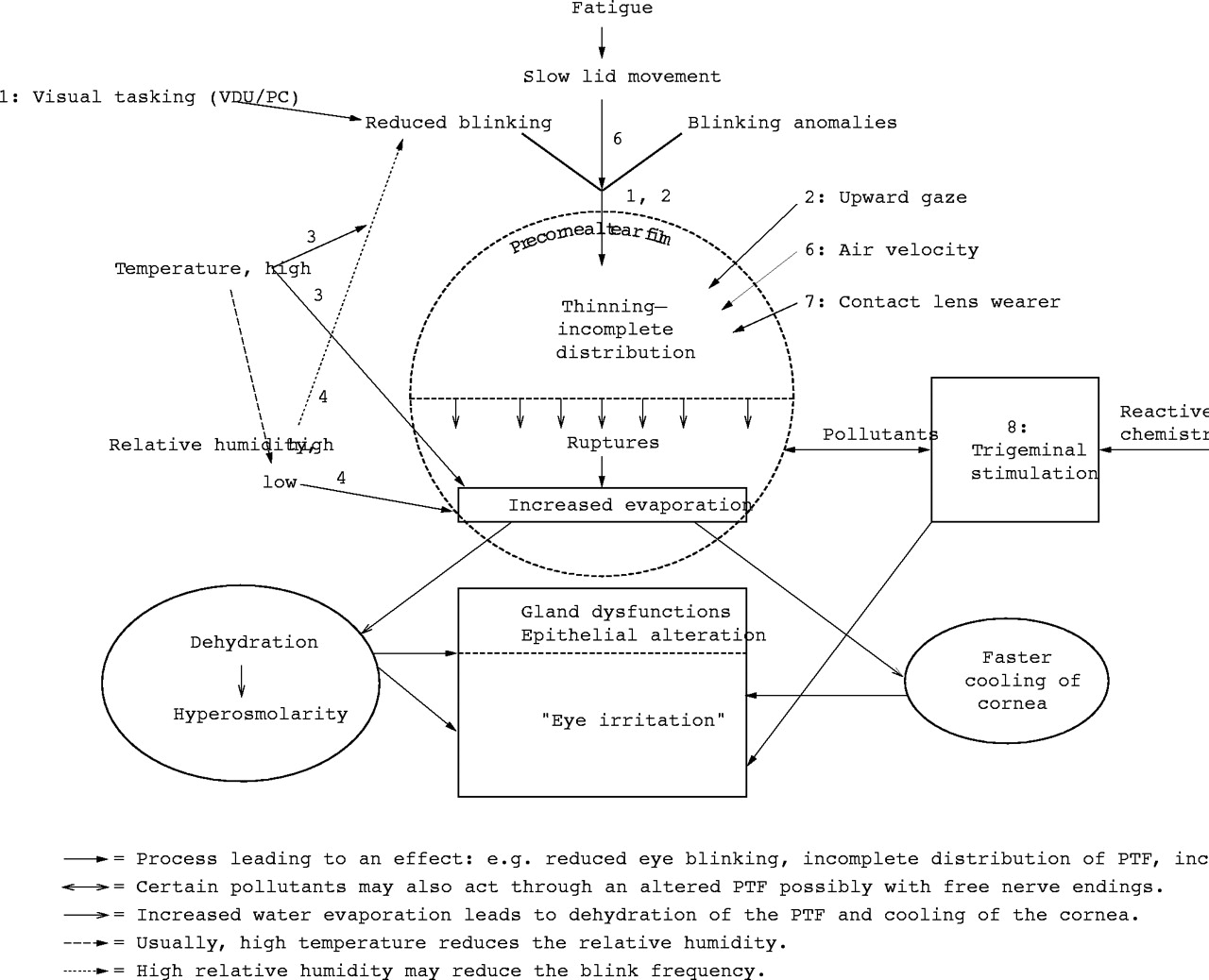
There is a mechanistic dichotomy of eye complaints mediated through trigeminal stimulation by the action of certain irritating indoor pollutants and dry eyes, mediated through corneal stimulation by an APTF (see fig 1). However, it is still difficult to fully understand the aetiopathogenesis of symptoms, in that individual, environmental, and task related causes can be synergistically involved, in addition to the use of certain kinds of medication. There is no indication that indoor pollutants, neither chemically stable VOCs nor particles, by themselves, can alter the PTF and result in eye complaints. However, gas phase oxidation mixtures between ozone and certain, common, chemically reactive VOCs (alkenes, like terpenes) can produce eye irritants, specifically in office environments, in addition to the well known eye and upper airway irritants, like formaldehyde. The impact of eye irritants might be further exacerbated by an APTF; for example, by prolonged low RH or high room temperature (see below).

{kind=link}
Diagram of processes resulting in altered precorneal tear film (PTF), which leads to increased water loss, damage of the epithelial layer of the PTF, and gland dysfunctions. In addition, certain irritant pollutants including “reactive chemistry” (for example, certain oxidation products) may stimulate trigeminus of the outer eye.
One alternative mechanism leading to perceived dried, tired, or irritated eyes is dehydration of the PTF, especially during work of high demand of visual tasking. Dehydration can occur by: (1) evaporative water loss; (2) tear composition deficiency—that is, gland dysfunctions, in particular meibomian140,141 and other lacrimal gland dysfunctions; and (3) blinking deficiency. Under these conditions, PTF is more prone to ruptures (that is, APTF), the severity of which increases with decreasing thickness.23,70 Once local thinning has occurred, resistance to further thinning decreases.41 Thinning, ruptures, and dry spots eventually result in enhanced water evaporation that is dominated by external diffusion. Lastly, blink anomalies that alter the PTF redistribution, thus causing ruptures, further aggravate the clinical and subjective picture. Moreover, an APTF decreases the optical quality of the eye, because of corneal irregularities.20,21
Conditions that may lead to increase of eye complaints in the office environment due to dryness of the PTF as a result of unbalanced water loss, and possible excess cooling of cornea, and the presence of certain reactive chemicals (irritants), include the following, according to fig 1:
-
VDU work or other near work with visual or cognitive tasking that reduces the BF leading to APTF, thinning of the PTF, and dehydration through unbalanced water loss
-
Upgaze direction, typical in VDU work, widens the OS exposure, consequently enhancing thinning and water loss
-
A high periocular temperature reduces the BF and enhances unbalanced water loss—that is, dehydration
-
Low periocular RH enhances water evaporation, leading to unbalanced water loss—that is, dehydration
-
High periocular air velocity (>1 m/sec) increases rapidly and consistently the water evaporation from OS, possibly also at lower velocities
-
A slower upper lid movement caused by fatigue/drowsiness leads to an incomplete PTF distribution on the OS
-
The use of CL alters the PTF profoundly and promotes the condition for water loss—that is, OS dehydration
-
The presence of specific eye irritants formed in reactions between ozone and certain unsaturated organic compounds (for example, alkenes). Their effect may be exacerbated at conditions of APTF.
The hypothesis remains that an APTF facilitates the access of typical indoor pollutants, resulting in eye complaints and/or OS irritation. Rather than chemically stable indoor organic pollutants being a cause of eye complaints, it appears more plausible that work related factors like VDU, including high temperature, low RH, demands of visual and cognitive tasking, and psychological fatigue, enhance the water loss leading to dehydration of the PTF. Unsaturated VOCs in the indoor environment that undergo oxidation reactions with ozone should be considered sources of irritation, in particular in low RH environments.
For individual preventive measures, maintenance of the physiological BF is important in order to keep the OS moist as well as retain the OS as small as possible by downward gaze. Regular voluntary (that is, conscious) complete or fast blinking exercises combined with breaks could also be beneficial, in particular when carrying out work of high demand of visual tasking. In addition, high room temperature and/or low RH should be avoided, while high periocular RH is beneficial, in particular for CL wearers suffering from dry eyes. CL wearers and subjects suffering from ocular surface pathologies, should be considered susceptible and offered a health surveillance programme according to Council Directive 270/EEC. A number of potential patients are probably overlooked in the clinic, because eye irritation may appear only under certain indoor environmental conditions and be absent during examination. In addition to better descriptors for eye irritation in both clinical and epidemiological work, future research should focus on occupational conditions of APTF in combination with indoor irritants.
Acknowledgments
The work was partially supported by The Danish Working Environment Council and Service Center (2001-25).