Article Text

Abstract
OBJECTIVE To estimate the individual and combined associations of physical and psychosocial working environment with disabling shoulder pain and to identify groups at “high risk” for shoulder pain.
METHODS A cross sectional survey was conducted at five manual occupational settings in south Manchester, United Kingdom (n=775, 83%).
RESULTS Both the duration of occupational physical demands (working postures, manual handling activities, and repetitive arm movements) and psychosocial working environment (psychological demands and lack of opportunity to learn new skills) were found to be significantly associated with shoulder pain. Three occupational factors identified a high risk group for shoulder pain: duration of lifting with one hand (prevalence rate ratio (PRR) (highest third) 2.0, 95% confidence interval (CI) 1.4 to 2.8), duration of working above shoulder level (PRR (highest third) 2.2, 95% CI 1.5 to 3.3), and whether employees found their work stressful (PRR (highest third) 1.4, 95% CI 1.0 to 2.1). In addition, a measure of psychological distress (General Health Questionnaire (GHQ) score) was found to identify a group at high risk for shoulder pain (PRR (highest third) 1.9, 95% CI 1.3 to 2.9). In employees exposed to three or more of these factors, 79% (23/29) reported shoulder pain compared with only 16% (56/353) of those not exposed to any.
CONCLUSION This study has identified a variety of occupational physical demands and psychosocial factors associated with shoulder pain. It has also identified groups of employees at a “high risk” for shoulder pain by their exposure to both physical and psychosocial factors.
- shoulder pain
- occupational physical demands
- psychosocial working environment
Statistics from Altmetric.com
Shoulder pain is both common and disabling in the general population. It has been estimated that as many as one third of adults in the UK experience shoulder symptoms with some associated disability—namely, limitation in activities of daily living, in any one month.1 Conditions in the workplace are thought to be important contributors to shoulder pain and there has been much research into the possible relation between features of the working environment and the development of shoulder pain in this adult group.1-5 Evidence has been largely based on prevalence studies, which have identified an increased occurrence of shoulder pain in particular occupational groups.6 Features of the occupational environment believed to increase the risk of shoulder pain include awkward or uncomfortable working postures,7 manual handling of loads,3 and repetitive arm movements,8 though accurate or comprehensive assessment of such physical demands has rarely been carried out. In addition, the focus of research to date has been primarily based on specific occupational groups, limiting the generalisability of results to other occupational settings which might have very different occupational exposures. Finally, studies of the physical demands of work have rarely considered the role of psychosocial work factors in the development of shoulder symptoms.9
This study aimed to (a) estimate the association of disabling shoulder pain with occupational physical demands, (b) estimate the individual and combined associations of physical demands and psychosocial working environment, and (c) identify groups at high risk for disabling shoulder pain. It was conducted across a variety of manual occupational settings.
Patients and methods
DESIGN AND STUDY GROUP
A cross sectional survey was conducted of five manual occupational settings in south Manchester, United Kingdom. The occupational groups were selected to comprise subjects undertaking a variety of manual occupational tasks which might be associated with shoulder pain. All the available workforces were surveyed (total n=931): 135 mail sorters (post office), 198 cashiers and shelf stackers (supermarket), 169 cashiers and shelf stackers (department store), 250 production line workers (packaging factory), and 179 nurses and nursing auxiliaries (hospital).
SURVEY QUESTIONNAIRE
The survey questionnaire comprised three sections: (a) the physical demands of work, (b) psychosocial working environment and psychological wellbeing, and (c) assessment of the presence of shoulder pain and related disability.
Physical working environment
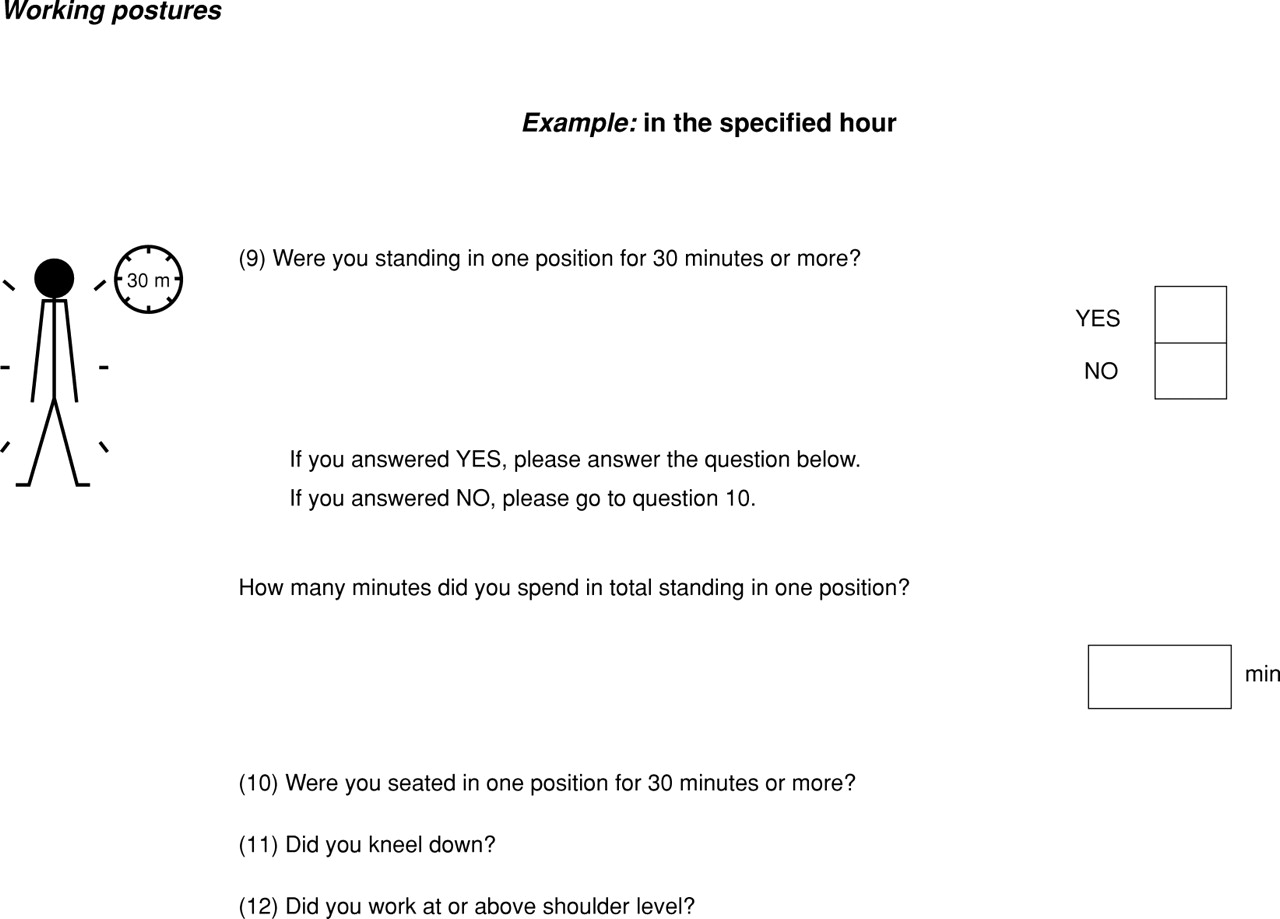
The Manchester Occupational Physical Demands Questionnaire, developed by the authors, was used to assess the physical demands of work.10 This questionnaire is an instrument evaluating self reported information on working postures, manual handling activities, and repetitive arm movements () assessed for one specified hour of an employee's shift. It has previously been validated within the study population by comparing responses to the questionnaire with direct simultaneous observations.10
Psychosocial working environment and psychological wellbeing
Psychosocial working environment was measured according to the demand-control-support model developed by Karasek.11 Three items related to psychological demands and were previously used in the West of Scotland Twenty-07 Study of Health in the Community12 and in a population study of low back pain.13 Responses to the questions were categorical: “never”, “occasionally”, “about half the time”, “always/most of the time”. Two items were used to measure job control: “Are you able to decide how to carry out your work?” and “Do you learn new things at work?”. One item was used to measure social support from colleagues: “How satisfied are you with the support you receive from your workmates?”. These questions have been previously used in a study of back and limb disorders.14
The level of psychological distress was assessed using the 12 item General Health Questionnaire (GHQ). This instrument has been tested for reliability, validity, and sensitivity as a screening tool for mental disorder and as a measure of short term psychological distress.15 Subjects score between 12 and 48, with high scores indicating high levels of distress.
Assessment of shoulder pain
Self reported shoulder pain was assessed using a preshaded manikin; symptoms in and around the shoulder complex (fig 1) lasting for more than 24 hours in the month before the survey. Associated disability was assessed as limitation in carrying out activities of daily living using items from a previously validated 22 item shoulder disability questionnaire.16 The definition of morbidity used in this study is reporting shoulder pain with at least one disability. This classification of disabling shoulder pain was made to exclude the more minor or transient episodes of shoulder pain.1

Boundary used for the shoulder in defining shoulder pain.
STATISTICAL ANALYSIS
Variables reflecting the duration of occupational physical demands, psychosocial working environment, and psychological wellbeing were each categorised into three levels. Information on physical demands was first divided into those with some or no exposure, then, within those with some exposure, a further division was made into low and high duration, with approximately equal numbers in each group. Scores based on completion of the GHQ were categorised into tertiles based on the distribution, with approximately equal numbers in each group. The lowest tertile of GHQ score was used as the referent group for estimating associations with disabling shoulder pain. Univariate associations between exposure information and disabling shoulder pain were summarised with prevalence rate ratios (PRR) and 95% confidence intervals (95% CI) and adjusted for age, sex, and type of workplace.
To identify a group of factors which were most commonly associated with shoulder pain a forward stepwise Cox regression procedure was used.17 Factors significantly associated with shoulder pain in the univariate analysis were potential candidate variables for entry into the appropriate multivariate models. Two models were constructed: (a) including occupational physical demands and (b) including psychosocial working environment and psychological wellbeing. A final model was created including variables selected into each of the two models described above adjusted for age, sex, and type of company. All the analyses were carried out using Stata.18
Results
In total, 775 survey questionnaires were completed, giving an overall participation rate of 83%. The response rates were similar for the five occupational settings taking part in the study, ranging from 80% for mail sorters to 86% for cashiers and shelf stackers.
Of the 775 subjects 198 (26%) had a one month period prevalence of disabling shoulder pain. Although the prevalence of disabling shoulder pain was similar across the five occupational settings, a significantly higher proportion of older employees compared with younger employees and women compared with men reported disabling symptoms (table 1). Most of the shoulder pain episodes were unilateral (127/198, 64%).
Prevalence of disabling shoulder pain by company, age, and sex
OCCUPATIONAL PHYSICAL DEMANDS
Working above shoulder level was found to be significantly associated with disabling shoulder pain (table 2), with respondents working for the longest time in this way having more than a twofold increase in risk relative to those who did not carry out this activity.
Association of the duration of occupational physical demands (for one specified hour) with disabling shoulder pain
Four of the six manual handling activities were significantly associated with disabling shoulder pain (table 2). The risk of disabling shoulder pain increased significantly with the duration of lifting weights with one hand, lifting weights above shoulder level, pulling weights, and carrying weights on one shoulder, with approximately a doubling of risk seen for exposure to these activities for the longest time compared with no exposure.
Both repetitive movements of the wrists and arms for continuous periods of 10 minutes or more were significantly associated with disabling shoulder pain (table 2). Approximately a doubling of the risk of disabling shoulder pain was seen for the duration of repetitive use of the wrists and arms, at any level of exposure.
PSYCHOSOCIAL WORKING ENVIRONMENT AND PSYCHOLOGICAL WELLBEING
The risk of disabling shoulder pain significantly increased with the amount of time spent in a psychologically demanding working environment; whether employees found their work hectic or too fast, monotonous or boring, and stressful (table 3). Employees who reported being exposed to psychological demands “always/most of the time” had an increased risk of disabling shoulder pain of between 50 and 90% relative to the reference group of those who worked in a psychologically demanding environment “never/occasionally”.
Association of psychosocial working environment and psychological wellbeing with disabling shoulder pain
Variables relating to decision authority and social support did not appear to be associated with disabling shoulder pain. However, the ability to learn new skills at work was associated with those employees reporting that they “seldom” or “very seldom” had the opportunity to learn new skills at work having a 70% increase in the risk of disabling shoulder pain (table 3).
Psychological distress, according to the GHQ, was found to be significantly associated with disabling shoulder pain (table 3), with a GHQ score in the highest tertile (24–48), based on the distribution of scores, being associated with more than a doubling of risk compared with the lowest tertile (12–20).
MULTIVARIATE ANALYSIS
Of the eight occupational physical demands significantly associated with disabling shoulder pain and offered as candidates to the first regression model, three were entered into the model as best describing the occurrence of disabling shoulder pain within the study group: duration of standing in one position, lifting weights with one hand, and working above shoulder level. In the second regression model two of the five variables relating to psychosocial working environment and psychological wellbeing were entered into the model: the GHQ score (psychological distress) and whether the employees found their work caused them stress or anxiety.
These five variables were placed into a final multivariate model together with age, sex, and type of company to assess the independent associations with disabling shoulder pain (table 4). For the duration of occupational physical demands and the GHQ score (psychological distress) the doubling of risk for the highest tertile of exposure relative to the lowest, seen in the univariate analysis, was maintained.
Association of factors entered into the final model (after being selected into stepwise models (a) and (b)4-150) with disabling shoulder pain
Table 5 shows how well the variables entered into the final regression model describe the occurrence of disabling shoulder pain. Variables were dichotomised into “high exposure” (the highest tertile of each variable) and “not exposed/low exposure” for this analysis. In the final regression model only 56/353 (16%) of the employees who reported being “not exposed/low exposure” to all of the variables reported disabling shoulder pain. This compared with 73/276 (26%) of those who reported a “high exposure” to only one variable, 43/97 (44%) of those who reported a “high exposure” to any two variables, and 23/29 (79%) of those employees who reported a “high exposure” to three or more variables.
Occurrence of disabling shoulder pain by number of variables reported by subjects entered into the final model
Discussion
Previously it has been shown that occupational conditions, such as sustained work above shoulder level and repetitive arm movements, are related to the development of shoulder symptoms.19-24 The findings from this study are consistent with these observations. However, manual handling as a potential risk factor for shoulder and arm pain has rarely been investigated, with greater emphasis being placed on the association of such activities with low back pain.25 In the current study it was found that lifting weights, carrying weights, and pulling weights were all significantly associated with disabling shoulder pain. This highlights the importance of considering the full range of occupational physical demands (working posture, manual handling activities, and repetitive arm movements) when investigating the role of the physical working environment in the occurrence of shoulder pain.
All aspects of the psychosocial working environment relating to psychological demands were found to be significantly associated with disabling shoulder pain. These findings are consistent with those of other cross sectional surveys, which report a modest but significant increase in the risk of shoulder pain for jobs with high psychological demands.26 ,27 However, there was no association between decision authority, social support, and disabling shoulder pain; features of the psychosocial working environment described previously as being related to the development of shoulder symptoms.27
The GHQ score, representing psychological wellbeing, was also found to be significantly associated with disabling shoulder pain. This finding is consistent with other studies of musculoskeletal pain, which have found psychological distress to be related to the subsequent development of symptoms.28
The modelling procedure was used to identify groups at high risk for the occurrence of disabling shoulder pain. Different strategies of intervention would be needed to deal with the three occupational factors found to contribute independently to risk. Ergonomic redesign of jobs would help to reduce the duration of working above shoulder level and lifting weights with one hand. The reasons for rating the work environment as stressful were not investigated in this study, but appropriate intervention would need to be devised and evaluated in workplaces in which stress is found to be a problem.
METHODOLOGICAL ISSUES
Although every effort was made to survey the full workforce from all the occupational settings, some employees were absent at the time of the survey. This could lead to a distortion of the results owing to the “healthy worker effect”; employees with musculoskeletal symptoms being more likely to be away from work on sick leave because of their symptoms. However, only 30 such people were identified and after consultation with the personnel departments it was found that none of these were absent owing to shoulder symptoms.
Measurement of the physical demands of work was made over a one hour reference period selected randomly throughout the employees' shifts. This period was selected in preference to extended time periods and average exposure measurement during a shift, given the limitations in validating such assessment.10 After observing the working practices of the study group, it was evident that occupational activities could be well defined in a relatively short reference period because tasks did not vary substantially across the shift.
Finally, interpretations from this study are limited by its cross sectional design as it is not possible to establish the temporal course of events leading to the onset of disabling shoulder pain; both the exposures and disease are measured at the same point in time. It is unlikely that having disabling shoulder pain would result in employees working with greater physical demands (although there is a possibility that employees with symptoms might perceive their work as more physically demanding). However, the relation between psychosocial factors and shoulder symptoms is less clear. For example, although significant associations were found between occupational psychosocial demands (work defined as monotonous/repetitive, too hectic/fast, or causing stress/worry) and disabling shoulder pain, it might be the case that having such shoulder symptoms actually causes employees to experience greater psychological demands rather than the psychological demands themselves being risk factors for disabling shoulder pain. However, in a detailed review of studies considering the role of the occupational psychosocial working environment in the development of arm pain, Bongers et alidentified two longitudinal studies which identified occupational psychological demands as predictors of neck/shoulder pain.9 In addition, it has been noted that psychological factors often predict the future onset of physical symptoms, such as musculoskeletal pain.28 ,29 It is therefore likely that the occupational factors identified in this study as being associated with disabling shoulder pain are likely to precede the onset of such symptoms rather than occur exclusively as a consequence of such pain.
Summary
This large cross sectional survey has identified a wide range of occupational physical demands associated with disabling shoulder pain across a variety of manual occupational settings using a validated self completion questionnaire. We have shown that the amount of time spent in constrained working postures, carrying out manual handling activities, and making repetitive arm movements are all associated with disabling shoulder pain. In addition, this study has identified features of the psychosocial working environment associated with shoulder symptoms. Using multivariate analytical techniques, we identified groups of employees at a “high risk” for disabling shoulder pain due to exposure to both physical and psychosocial factors. The study provides useful information for possible ergonomic interventions in order to reduce the burden of such symptoms.
The Manchester Occupational Physical Demands Questionnaire


{kind=link}
{kind=link}
{kind=link}
{kind=link}