
Abstract
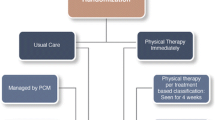
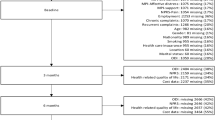
In an attempt to prevent acute low-back pain from becoming a chronic disability problem, an earlier study developed a statistical algorithm which accurately identified those acute low-back pain patients who were at high risk for developing such chronicity. The major goal of the present study was to evaluate the clinical effectiveness of employing an early intervention program with these high-risk patients in order to prevent the development of chronic disability at a 1-year follow-up. Approximately 700 acute low-back pain patients were screened for their high-risk versus low-risk status. On the basis of this screening, high-risk patients were then randomly assigned to one of two groups: a functional restoration early intervention group (n = 22), or a nonintervention group (n = 48). A group of low-risk subjects (n = 54) who did not receive any early intervention was also evaluated. All these subjects were prospectively tracked at 3-month intervals starting from the date of their initial evaluation, culminating in a 12-month follow-up. During these follow-up evaluations, pain disability and socioeconomic outcomes (such as return-to-work and healthcare utilization) were assessed. Results clearly indicated that the high-risk subjects who received early intervention displayed statistically significant fewer indices of chronic pain disability on a wide range of work, healthcare utilization, medication use, and self-report pain variables, relative to the high-risk subjects who do not receive such early intervention. In addition, the high-risk nonintervention group displayed significantly more symptoms of chronic pain disability on these variables relative to the initially low-risk subjects. Cost-comparison savings data were also evaluated. These data revealed that there were greater cost savings associated with the early intervention group versus the no early intervention group. The overall results of this study clearly demonstrate the treatment- and cost-effectiveness of an early intervention program for acute low-back pain patients.
Similar content being viewed by others

REFERENCES
Deyo RA, Cherkin D, Conrad D, Volinn E. Cost, controversy, crisis: Lowäback pain and the health of the public. Annu Rev Pub Health 1991; 12: 141–156.
Mayer TG, Gatchel RJ. Functional restoration for spinal disorders: The sports medicine approach. Philadelphia: Lea & Febiger, 1988.
Feuerstein M, Berkowitz SM, Peck CA. Musculoskeletal related disability in U.S. army personnel: Prevalence, gender, and military occupational specialties. J Occup Environ Med 1997; 39: 68
Krause N, Ragland DR. Occupational disability due to lowäback pain: A new interdisciplinary classification used in a phase model of disability. Spine 1994; 19: 1011–1020.
National Research Council. Musculoskeletal disorders and the workplace: Lowäback and upper extremities. Washington, DC: National Academy Press, 2001.
Crombie IK, Croft PR, Linton SJ, LeResche L, Von Korff M. Epidemiology of pain, Vol. I Seattle: IASP Press, 1999.
Linton SJ. A cognitiveäbehavioral approach to the prevention of chronic back pain. In: Turk DC, Gatchel RJ, eds. Psychological approaches to pain management: A practitioner's Handbook, 2nd edn-New York: Guilford, 2002.
Gatchel RJ, Polatin PB, Mayer TG. The dominant role of psychosocial risk factors in the development of chronic low-back pain disability. Spine 1995; 20: 2702–2709.
Linton SJ, Bradley LA. Strategies for the prevention of chronic pain. In: Gatchel RJ, Turk DC, eds. Psychological approaches to pain management: A practitioner's handbook. New York: Guilford, 1996.
Gatchel RJ, Polatin PB, Kinney RK. Predicting outcome of chronic back pain using clinical predictors of psychopathology: A prospective analysis. Health Psychol 1995; 14: 415–420.
Pulliam C, Gatchel RJ, Gardea MA. Psychosocial differences in high risk versus lowärisk acute lowäback pain differences. J Occup Rehabil 2001; 11: 43–52.
Lachin JM, Matts JP, Wei LJ. Randomization in clinical trials: Conclusions and recommendations. Control Clin Trials 1988; 9: 365–374.
Stout RL, Wirtz PW, Carbonari JP, Del Boca FK. Ensuring balanced distribution of prognostic factors in treatment outcome research. J Stud Alcohol 1994; 12: 70–75.
Mayer TG, Prescott M, Gatchel RJ. Objective outcomes evaluation: Methods and evidence. In: Mayer TG, Polatin P, Gatchel RJ, eds. Occupational musculoskeletal disorders: Function, outcomes and evidence. Philadelphia: Lippincott Williams & Wilkins, 2000.
Mayer TG, Gatchel RJ, Mayer H, Kishino N, Keeley J, Mooney V. Prospective twoäyear study of functional restoration in industrial lowäback injury. JAMA 1987; 259: 1181–1182.
Hazard R, Fenwick J, Kalisch S, Redmond J, Reeves G, Reid S, Frymoyer J. Functional restoration with behavioral support: A oneäyear prospective study of patients with chronic low-back pain. Spine 1989; 14: 157–161.
Turk DC, Gatchel RJ. Psychological approaches to pain management, 2nd edn-New York: Guilford, 2002.
Dworkin SF, LeResche L. Research diagnostic criteria for temporomandibular disorders. J Craniomandib Disord Facial Oral Pain 1992; 6: 301355.
Bureau of Labor Statistics. 2002 Report. Washington DC: U.S. Department of Labor, 2002.
Medical fees in the United States 2000. Los Angeles: Practice Management Information Corporation, 2002.
Drug topics Redbook 2000. Montvale, NJ: Thompson Medical Economics, 2002.
Goossens MEJB, Evers SMAA. Economic evaluation of back pain interventions. J Occup Rehabil 1997; 7: 15–32.
Mitchell JH. Neural control of the circulation during exercise. Med Sci Sports Exerc 1990; 22: 141–154.
Mitchell RI, Carmen GM. Results of a multicenter trial using an intensive active exercise program for the treatment of acute soft tissue and back injuries. Spine 1990; 15: 514–521.
Mitchell RI, Carmen GM. The functional restoration approach to the treatment of chronic pain in patients with soft tissue and back injuries. Spine 1994; 19: 633–642.
Webster B, Snook S. The cost of 1989 workers' compensation lowäback pain claims. Spine 1994; 19: 1111–1116.
Maetzel A. The economic burden of lowäback pain. Best Pract Res Clin Rheumatol 2002; 16: 23–30.
Annertz M, Wingstrand H, Stromqvist B, Holtas S. MR imaging as the primary modality for neuroradiologic evaluation of the lumbar spine. Acta Radiol 1996; 37: 373–380.
Boden S, Swanson A. An assessment of the early management of spine problems and appropriateness of diagnostic imaging utilization. Phys Med Rehabil Clin N Am 1998; 9: 411–417.
Carey T, Garrett J, Jacknam A, McLaughlin C, Fryer J, Smucker D. The outcomes and costs of care for acute lowäback pain among patients seen by primary care practitioners, chiropractors, and orthopedic surgeons. N Engl J Med 1995; 333: 913–917.
Rosen N, Hoffberg H. Conservative management of lowäback pain. Phys Med Rehabil Clin N Am 1998; 9: 435–472.
Friedlieb O. The impact of managed care on the diagnosis and treatment of low-back pain. Am J Med Qual 1994; 9: 24–29.
Moffett JK, Torgenson D, BelläSayer S, Jackson D, Llewlyn-Phillips H, Farrin A, Barber J. Randomized controlled trial of exercise for low-back pain. BMJ 1999; 319: 279–283.
Butterfield P, Spencer P, Redmond N, Feldstein A, Perrin N. low-back pain: Predictors of absenteeism, residual symptoms, functional impairment, and medical costs in Oregon workers' compensation recipients. Am J Ind Med 1998; 34: 559–567.
Torstensen T, Ljunggren A, Meen H, Odland E, Mowinckel P, Geijerstan S. Efficiency and costs of medical exercise therapy, conventional physiotherapy, and self exercise in patients with chronic low-back pain. Spine 1998; 23: 2616–2624.
Skouen J, Grasdal A, Haldorsen E, Ursin H. Relative cost effectiveness of extensive and light multidisciplinary treatment programs versus treatment as usual for patients with chronic low-back pain on long term sick leave. Spine 2002; 27: 901–910.
Mannion A, Muntener M, Taimela S, Dvorak H. Comparison of three active therapies for chronic low-back pain. Rheumatology 2001; 40: 772–778.
Bolten W, Kempel-Waibel A, Pforringer W. Analysis of the cost of illness in backache. Med Klin 1998; 93: 388–393.
McInstosh G, Frank J, HoggäJohnson S, Bombardier C. Prognostic factors for time receiving workers' compensation benefits in a cohort of patients with low-back pain. Spine 2000; 25: 147–157.
Chibnall J, Tait R, Merys S. Disability management of low-back injuries by employer retained physicians: Ratings and costs. Am J Ind Med 2000; 38: 529–538.
Hashemi L, Webster B, Clancy E. Trends in disability duration and cost of workers' compensation low-back pain claims (1988–1996). JOEM 1998; 40: 1110–1119.
Hashemi L, Webster B, Clancy E, Volinn E. Length of disability and cost of workers' compensation low-back pain claims. 39 1997;10.
Sundararajan V, Konrad T, Garrett J, Carey T. Patterns and determinants of multiple provider use in patients with acute low-back pain. J Gen Intern Med 1998; 13: 528–533.
Boden S, Dreyer S, Levy H. Management of low-back pain. Phys Med Rehabil Clin N Am 1998; 9: 419–433.
Foa FB. Psychological treatment of posttraumatic stress disorder. J Clin Psychiatry 2000; 61: 43–51.
Author information
Authors and Affiliations
Rights and permissions
About this article
Cite this article
Gatchel, R.J., Polatin, P.B., Noe, C. et al. Treatment- and Cost-Effectiveness of Early Intervention for Acute Low-Back Pain Patients: A One-Year Prospective Study. J Occup Rehabil 13, 1–9 (2003). https://doi.org/10.1023/A:1021823505774
Issue Date:
DOI: https://doi.org/10.1023/A:1021823505774