Article Text

Abstract
Objective To describe the survey methodology and initial general findings of the first Central American Survey of Working Conditions and Health.
Methods A representative sample of 12 024 workers was interviewed at home in Costa Rica, El Salvador, Guatemala, Honduras, Nicaragua and Panama. Questionnaire items addressed worker demographics, employment conditions, occupational risk factors and self-perceived health.
Results Overall, self-employment (37%) is the most frequent type of employment, 8% of employees lack a work contract and 74% of the workforce is not covered by social security. These percentages are higher in Guatemala, Honduras and El Salvador, and lower in Costa Rica, Panama and Nicaragua. A third of the workforce works more than 48 h per week, regardless of gender; this is similar across countries. Women and men report frequent or usual exposures to high ambient temperature (16% and 25%, respectively), dangerous tools and machinery (10%, 24%), work on slippery surfaces (10%, 23%), breathing chemicals (12.1%, 18%), handling toxic substances (5%, 12.1%), heavy loads (6%, 20%) and repetitive movements (43%, 49%). Two-thirds of the workforce perceive their health as being good or very good, and slightly more than half reports having good mental health.
Conclusions The survey offers, for the first time, comparable data on the work and health status of workers in the formal and informal economy in the six Spanish-speaking Central American countries, based on representative national samples. This provides a benchmark for future monitoring of employment and working conditions across countries.
Statistics from Altmetric.com
What this paper adds
-
As a result of current economic models, informal employment is increasing and thought to be associated with worse working conditions.
-
Presently there exists no surveillance of work-related health effects or hazardous exposures suitable to assist in policy-making, anywhere in Latin America.
-
The First Central American Survey of Working Conditions and Health (ECCTS, by its Spanish acronym) offers, for the first time, comparable data on the work and health status of workers in the formal and informal economy in the six Spanish-speaking Central American countries, based on representative national samples.
-
The ECCTS underscores the low quality of a large part of employment in Central American countries, with three out of four members of the workforce lacking social security, a third being self-employed, and almost one out of ten salaried employees working without either a written or oral contract.
-
The ECCTS provides a reference measure for future monitoring of employment and working conditions across countries.
Introduction
Central America contains six Spanish-speaking countries: Guatemala, Honduras, El Salvador, Nicaragua, Costa Rica and Panama. Although countries differ considerably in development index ranging from 0.58 in Guatemala to 0.78 in Panama,1 the region has geographic, cultural and economic cohesion. Efforts towards greater integration have been ongoing for over 50 years,2 an important tool to eliminate poverty and improve living and working conditions of the Central American population.
In Central America, there is a dearth of information on working conditions and health.3 This creates barriers for informed policy decisions to improve health and well-being in this politically and economically important region. The establishment of reliable information systems is a top priority of several global health and development programs, including the United Nations Millennium Development Goals,4 the World Health Organization Workers’ Health Global Plan of Action 2008–2017,5 the Global Strategy in Occupational Safety and Health6 and the Ibero-American Strategy in Occupational Safety and Health (2010–2013) of the Ibero-American Social Security Organization.7
As a result of current economic models favouring external markets with deregulated formal work sectors, productivity and employment have been growing in the Latin American and Caribbean region.8 Also, in the context of the free trade agreements between Central America and North America, Europe and other Asian and South American economic blocks, occupational safety and health has become an issue of major relevance. It has been reported, however, that this growth has been accompanied by a general deterioration of working conditions for much of the population in Central America. This pattern has also increased informal employment, thought to be associated with worse working conditions for the majority of the working population.9
Although more than a decade ago the Pan-American Health Organization began promoting surveillance based on sentinel occupational health events information (fatal occupational injuries, pesticide poisonings and low back pain) in selected Latin American countries as a means to improve prevention and control measures,10 surveillance systems have been difficult to implement or to sustain over time. Today, there exists no surveillance of work-related health effects or hazardous exposures suitable to assist in policymaking, anywhere in Latin America.
Surveys are another tool to monitor workers’ conditions and health and, in fact, a common strategy used around the world. The European Working Conditions Survey has been conducted periodically since 1990, the fifth and most recent one in 2010, involving 34 member states.11 They provide important prevalence and time trend data on perceptions of workers about a variety of risks and their well-being. The results of these surveys play an important role in defining priorities for more in-depth research and also actions, on national and regional levels.
In Latin America, national surveys on working conditions and health have recently been completed successfully in Colombia,12 Argentina,13 Chile14 and Uruguay,15 but none in Central America. These surveys focused primarily on the formal sector because this sector is more accessible from a methodological viewpoint and because the formal sector is traditionally the main or only sector addressed by ministries of labour in Latin America.3 In Central America, the informal sector, including those employed in microenterprises, homes and the self-employed, was reported to be about half of the labour force in 199916 and 64% in 2006.9 Therefore, data systems on working conditions and health in Central America must address also informal workers.
Given the lack of reliable and comparable data on work and health in the Central American countries, in 2011 we developed and implemented the First Central American Survey of Working Conditions and Health (ECCTS, by its Spanish acronym),i targeting workers in both the formal and the informal economies. The goals of this paper are to describe the survey methodology and present initial general findings on work and health status in the region.
Subjects and methods
Study design and sample
The ECCTS was a cross-sectional survey of workers aged 18 or older, in the formal and informal economy and all economic activity sectors, who had worked for economic remuneration in the previous week for at least 1 h in the six Spanish-speaking countries of Central America (ie, excluding Belize).
The total regional sample consisted of 12 024 workers (data set is available upon request), applying a similar criterion used by the European Working Conditions Survey, in which the number by country is fixed around 1000. In our case, in each country, a same size representative sample of 2004 was drawn from the last census data available, randomly selecting 167 census segments from all departments (Guatemala, El Salvador, Honduras y Nicaragua) or provinces (Costa Rica and Panama) proportional to the respective populations in the departments or provinces. Within each sampling segment, 12 households were selected by random block walking. When a household was empty, interviewers returned once; if unsuccessful, the adjacent household was selected (between 47% in Panama and 32% in Costa Rica). In each household, only one worker was interviewed. When there was more than one eligible candidate in a household, the one with the nearest birthday was selected. When a worker did not consent participation, he was replaced by the one with the nearest birthday in the same household or someone from the adjacent household. Overall, participation rates before replacement were approximately 50% in Costa Rica, 60% in Honduras and 80% in Guatemala, El Salvador, Nicaragua and Panama.
To correct for differences between the sample and the source population of each country and the region as a whole, each individual included in the sample was weighted by sex, age (18–30, 31–50 and 51–65), economic sector (primary (agricultural), secondary (manufacturing and construction) and tertiary (services)) and country, according to the weighting methodology of the European Working Conditions Surveys.17 Weighting by occupational groups would have been useful, but was not possible as this information was not available from the census. Self-employed workers and the other occupational groups were classified into their respective economic activity sectors.
Questionnaire and survey administration
The questionnaire (available upon request) was designed based on prior review of the questionnaire of the Spanish Survey on Working Conditions (mainly health, safety and psychosocial items),18 ,19 the questionnaire of the European Survey on Working Conditions (ergonomic and hygiene items),11 the ILO Manual of Occupational Injury Statistics (injury)20 and the 12-item General Health Questionnaire (mental health).21 The questionnaire was developed in Spanish, pilot tested in 144 persons (24 workers per country), fine-tuned to the local terminology of each country and designed so that it would not take more than 30 min to complete. The questionnaire included 78 items (a table with key dimensions and items is provided as annex 1 available online), grouped into demographics (12), employment conditions (25), working conditions (12) and health-related indicators (29). If workers had more than one job, they were asked to answer the questions related to the job in which they spent the greatest number of hours in the week prior to the survey.
The fieldwork was carried out between July and December 2011. In all countries, the survey was administered by trained interviewers of Borge and Associates (http://www.borgeya.com), a company with extensive survey experience in the region. The local research team in each country closely supervised the data collection for quality assurance.
Measures
For the purpose of this report, we selected the following measures: sex, age (<30, 30–50 and >50 years); educational level (illiterate, complete and incomplete primary, secondary school and university); economic activity sectors (primary, secondary and tertiary); and occupational categories according to the International Standard Classification of Occupations: professionals, technicians, administrative support, services and retail sales, farming and fishing, skilled manual workers and unskilled manual workers.22
Employment condition questions centred on type of labour relationships (employer with employees, self-employed, permanent and temporary employees), contracts (written, oral, no contract), social security (yes/no) and hours worked in a week (cut-off at 48 h per week). Working conditions addressed the presence of hazards during a usual working day and, if present, more than 50% of a work shift. Examples include working on a slippery or unstable surface, handling dangerous tools and machines, exposure to high temperatures, inhalation of chemicals, handling of toxic substances, handling of heavy loads and performing repetitive movements.
Self-reported health indicators consisted of self-perceived health (very good or good vs regular or bad health) and mental health (with a score of less than three points indicating good vs bad), occupational injury in the last 12 months resulting in at least 2 days of absence and back pain in the last 4 weeks.
Ethical issues
Participants were informed of the survey objectives, invited to participate and had their questions answered. Verbal informed consent was given before the interview administration. Participants were provided with a written statement of the purpose of the survey and contact numbers in the country for any further questions or concerns. The project protocol was reviewed and approved by the institutional review boards of the Universidad Nacional in Costa Rica and The University of Texas Health Science Center at Houston.
Results
Demographic and labour characteristics of the sample
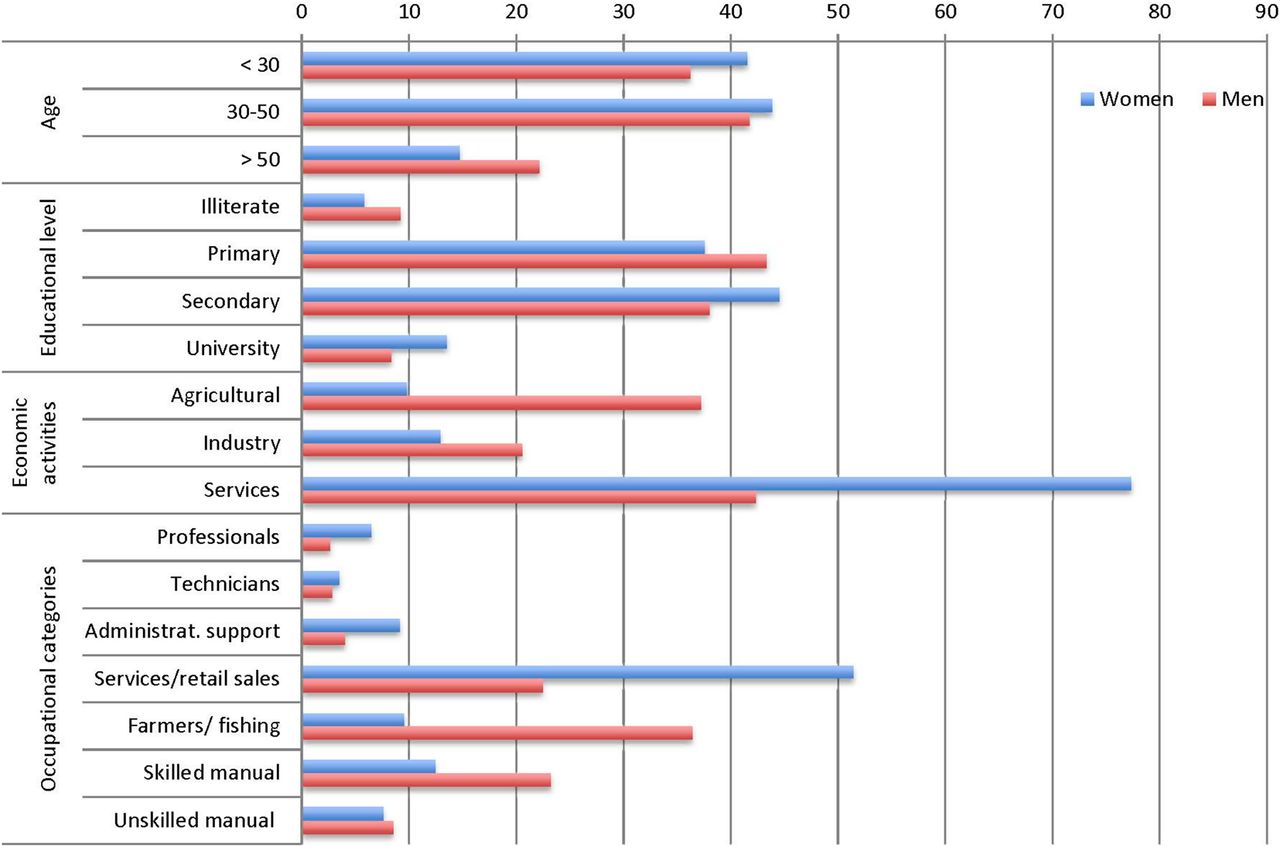
In the region (figure 1), workers were mostly young, with 85% of women and 79% of men under 50 years of age, and educational level was higher among women (13% university vs 6% illiterate level) than men (8% vs 9%, respectively), particularly in Panama, Costa Rica and Nicaragua. By economic activities sector, women worked mainly in the tertiary (service) sector (77%) and men in the secondary (service) sector (42%) and primary (agricultural) sector (37%), although on national levels, in Panama, Costa Rica and El Salvador a majority of men worked in the services sector (see online annex 2). Female occupations were mainly in retail sales and other services jobs (51%), whereas men were more frequently farmers (36%), with a lower proportion in retail sales (22%) and skilled manual jobs (23%).

Demographic and labour characteristics by sex at regional level. The First Central American Working Conditions and Health Survey, 2011 (n=12 024).
Employment and working conditions
Self-employment (around 37% among women and men) was the most frequent type of employment in the region (figure 2). Among employees, about 8% did not have a work contract, whether written or oral. These percentages were higher in Guatemala, Honduras and El Salvador. More than 70% of the region's workforce works without social security coverage, although there were large differences by country (between 33% of women and 35% of men in Costa Rica; and 85% and 91% in Honduras). Across all countries and both genders (see online annex 3), a third of the workforce worked more than 48 h per week.

Labour relationship and employment conditions by sex at regional level. The First Central American Working Conditions and Health Survey, 2011 (n=12 024).
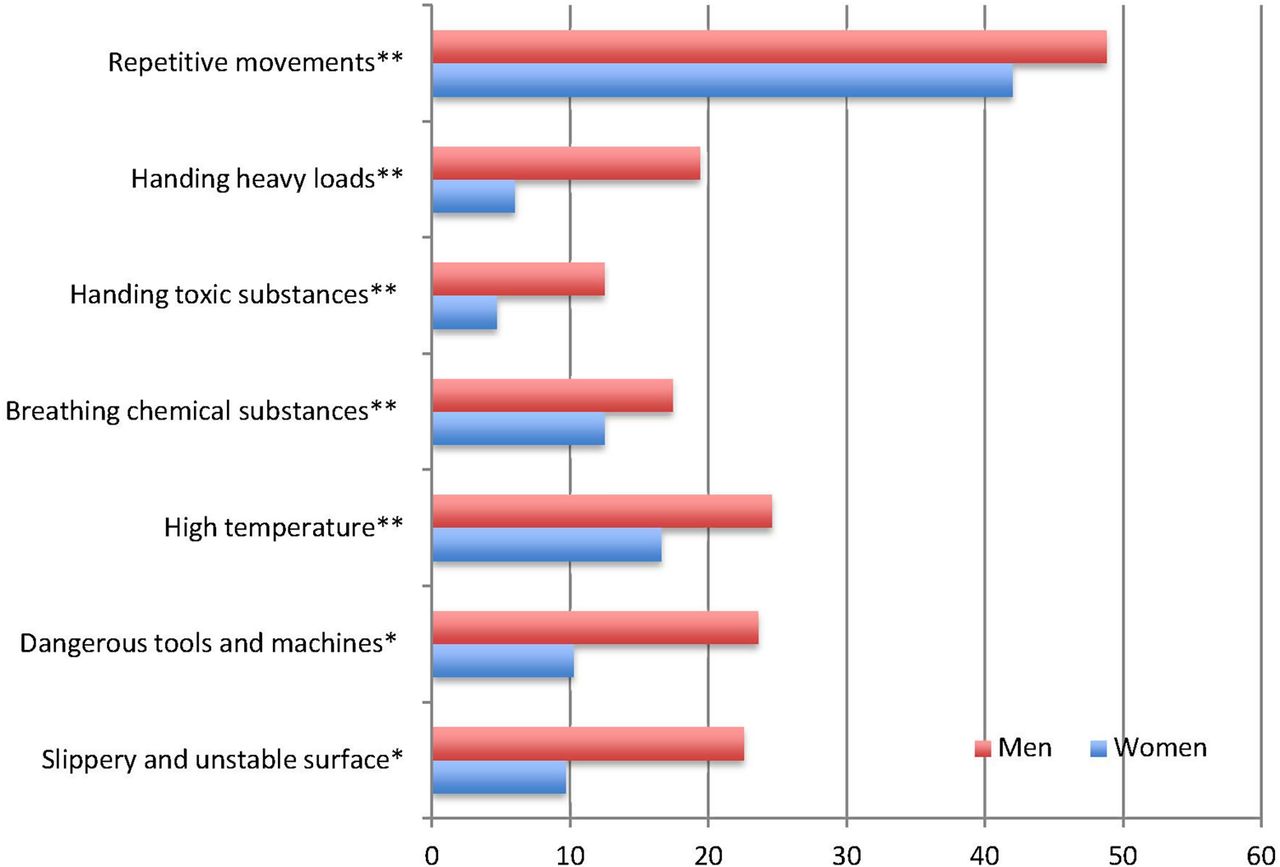
Regarding safety, ergonomic, hygiene and psychosocial working conditions (figure 3), one-fourth of men in the region and 16% of women reported being exposed to high ambient temperatures for more than half of a usual working day; 18% of men and 12% of women indicated exposure to inhalable chemicals for more than half a typical work shift; and 12% of men and 5% of women reported handling toxic substances. Handling heavy load at work was declared by 20% of men and 6% of women. These prevalences varied widely by country (see online annex 3).

Working conditions risk factors by sex at regional level. The First Central American Working conditions and Health Survey, 2011(n=12 024). *Always or very often; **more than half working day.
Health-related problems
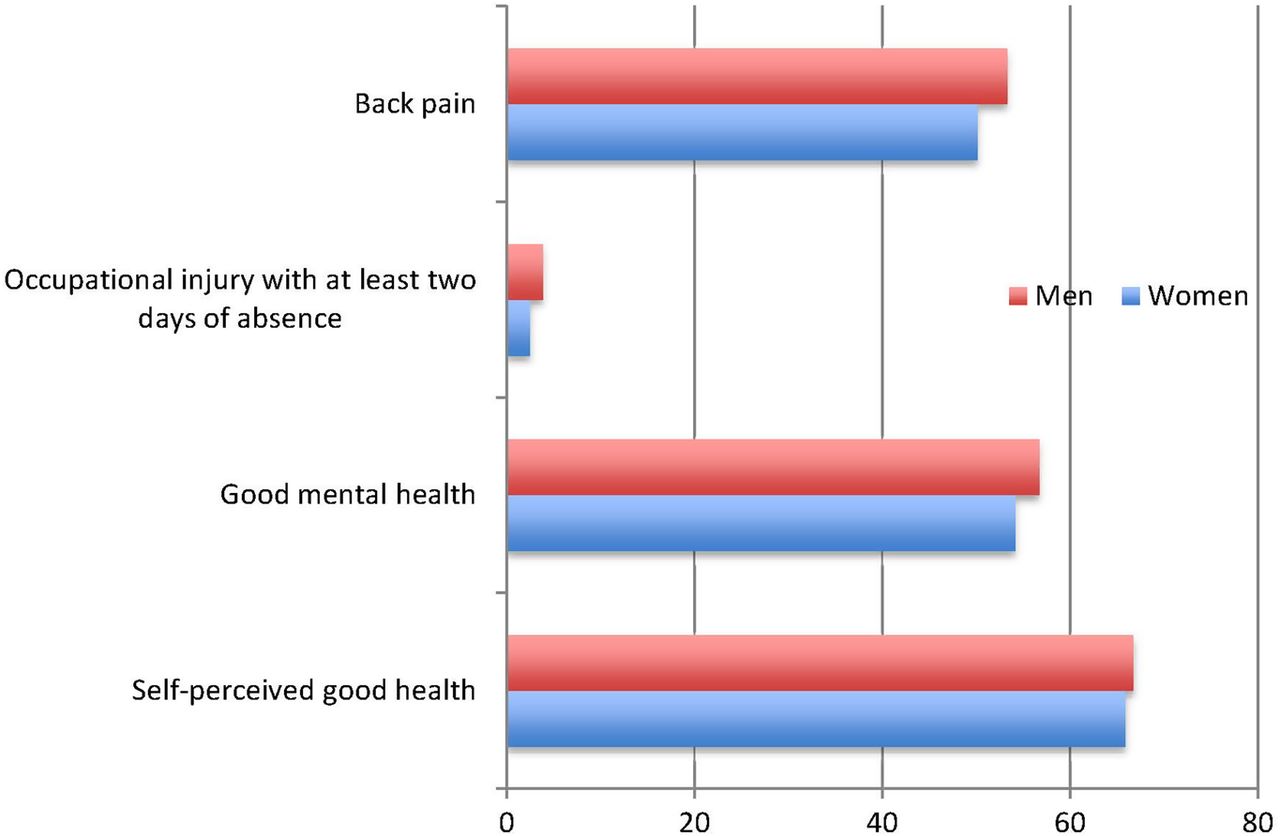
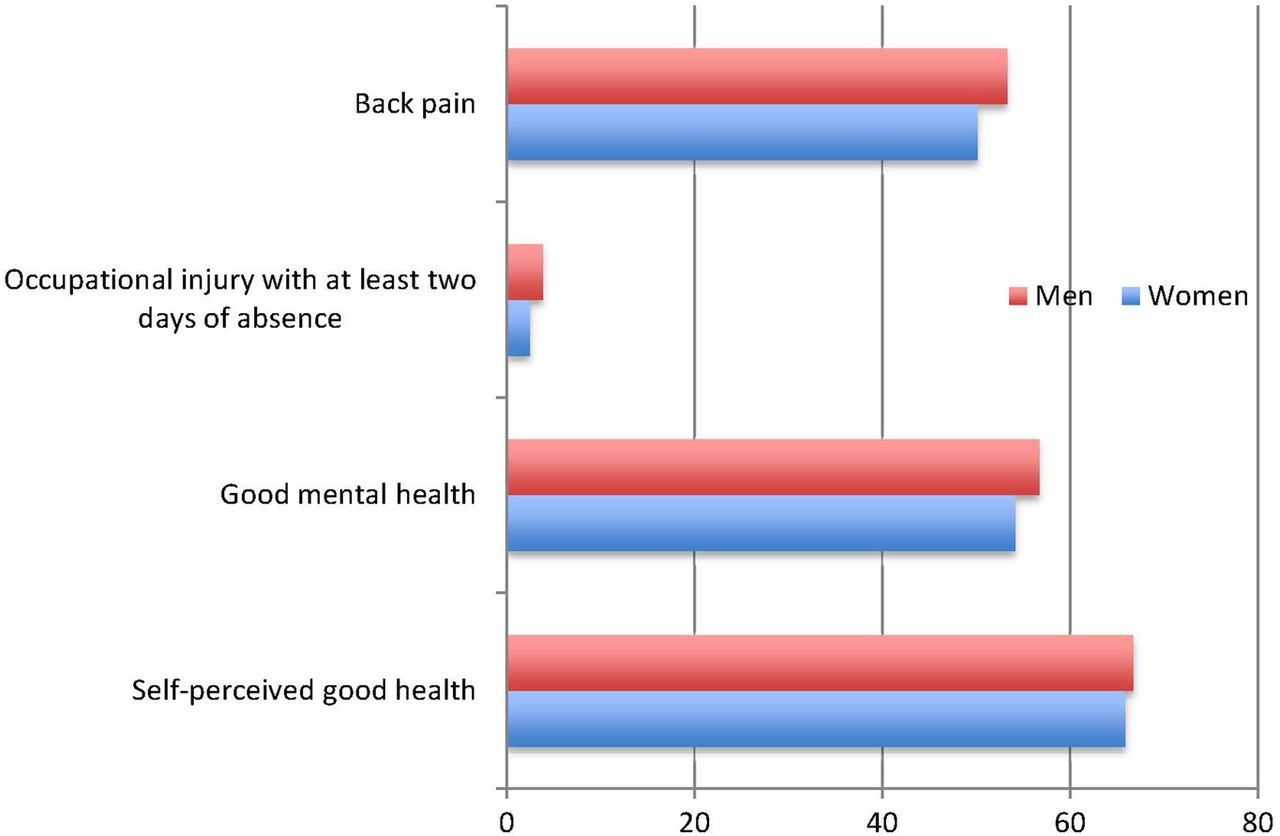
Two-thirds of the Central American workforce reported their health as being either good or very good (figure 4), and little more than half the workforce reported having good mental health (54% in women and 57% in men). Work-related injuries resulting in at least 2 days of absence in the previous year were reported by only 3% of Central American women and 4% of men, but on the other back pain in the previous 4 weeks was perceived by more than half the study population (50% of women and 53% of men). Prevalences by country are shown in online annex 4.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Health-related problems by sex at regional level. The First Central American Working conditions and Health Survey, 2011(n=12 024).
Discussion
The ECCTS offers, for the first time, comparable data on the work and health status of workers in the formal and informal economy in the six Spanish-speaking Central American countries, based on representative national samples. Among the initial findings, the survey underscores the low quality of a large part of employment in Central American countries, with three out of four members of the workforce lacking social security, a third being self-employed and almost 1 out of 10 salaried employees working without either a written or oral contract.
The ECCTS provides a reference measure for future monitoring of employment conditions across countries, as has been recently advocated.23 Thus, our findings highlight the magnitude of some characteristics related to informal employment in the region, such as the scarce extent of social security coverage, work without contract or work more than 48 h per week. As pointed out by the ILO, informal employment is a global problem, characterised basically by tasks performed outside of labour legislation and social protections.24 The ECCTS data suggest that there is a north–south division in Central America, with poorer employment conditions in the north of the region (Guatemala, El Salvador and Honduras), better ones in the south (Costa Rica and Panama) and Nicaragua somewhere in between. This south–north gradient could be explained by employment conditions (contract type, social protections, etc.), mostly related to a specific country's legal framework and its enforcement. In this sense, the southern part of Central America could be considered to be in transition towards a decent job agenda and social protection floor.25 Future studies are needed to assess this hypothesis.
Regarding working conditions, the high level of perceived exposure to repetitive movements is noteworthy among men and women. This percentage is similar to the recent findings in Finland (44.3%), France (44.2%) and Spain (40.9%).11 More in-depth analyses of the ECCTS will help elucidate this finding. Interestingly, the CUPID study (a study of musculoskeletal disorders in office workers and nurses in 18 countries) showed Costa Rica and Nicaragua to have some of the highest prevalences of musculoskeletal disorders.26 Another finding that merits highlighting is exposure to high temperatures at work, particularly in Guatemala, Honduras and El Salvador. Occupational heat exposure is becoming an increasingly important issue on the climate change agenda, and concerns about heat exposure among Central American workers have been raised.27 Notably, in Central America heat exposure has been identified as a possible causal factor in an ongoing occupational epidemic of chronic kidney disease of unknown etiology.28 ,29
In relation to health, the overall percentage of Central American workers who perceived themselves as being in good health was high, approximating that of OECD countries in 2009: 67% of women and 72% of men.30 However, the range was wide, from only 50% in Nicaragua to around 85% in Panama. Differences between countries were also large for perceived good mental health, ranging from 46% in Guatemala to 86% in Panama. More analyses of the ECCTS will help elucidate this finding. Future studies based on this survey will explore associations between self-reported health and working conditions,31 and also how social status models the self-reporting32 in the context of developing countries.
The low figures reported for occupational injuries are surprising: around 3% overall for injuries with at least 2 days of absence, which contrasts with an ILO estimation for the region including injury causing at least 3 days absence from work between 12.1% (Costa Rica) and 17.1% (Guatemala).33 This result also seems to be at odds with the high percentage (over 50%) of back pain in the previous 4 weeks, a health problem often attributed to overexertion at work. Although the wording for this questionnaire item was based on the ILO Manual of Occupational Injury Statistics,20 we believe that its interpretability among Central American workers needs to be re-examined. As Guiffrida and colleagues urged, Latin America needs more consistent and standardised occupational injury surveillance systems.34
Our survey could have been affected by selection bias. The response rate was lowest in Costa Rica, which was the first country surveyed. A lesson learned in Costa Rica was to time the interviews so that workers are home and have time and energy to respond. The appropriate time for interview depends on the type of labour, and this factor was more strictly taken into consideration in the countries surveyed subsequently. There were two incidents where the initially selected segment could not be reached due to severe climatic conditions. In these cases, the segments were substituted by a nearby similar segment and this likely had little impact on the overall sampling. The experience gained in the ECCTS will certainly allow for logistical improvements in future surveys, but we feel confident that the overall sampling design and randomisation process decreased selection bias and, together with the weighting performed (according to each country's population distribution), increased cross-country comparability. In fact, there were only small percentage differences when the last census data available were compared with the weighted sample for each country and Central America overall (see online annex 5). The few significant differences (p<0.05) by sex and economic sector in Costa Rica, Nicaragua, Honduras and Central America are mostly due to large sample sizes of the censuses.
Furthermore, the ECCTS includes only workers aged 18 years and older, which leaves youth workers out of the sample, many of whom work as informal employees. This criterion was adopted because 18 years is the official majority of age, and ethical issues limited our access to this subgroup for interviewing. Ideally, the age limit should be lowered in future surveys.
Misclassification bias could have occurred in relation to self-reported exposures and health status since both are determined by personal expectations and knowledge. Furthermore, except for the General Health Questionnaire,22 items included in our questionnaire are not validated. However, our pilot study allowed us to linguistically adapt the items to each Central American country. Also, having trained interviewers conduct the survey and doing so in the workers’ homes is a strength of the study avoiding information bias, as respondents would be more likely to respond openly than if the interview had been conducted at the workplace. In addition, direct data entry and online transmission to a central facility in San José, where data were checked, on a daily or more frequent basis guarded against significant data errors. Finally, in the context of informal employment, individuals may be engaged in various jobs, each with its own hazards, and this may not have been measured since questions only focused on the job in which individuals spent the greatest number of hours.
The limitations of this survey are counterbalanced by several strengths. Most importantly, the ECCTS is the first such study in this region using a solid sample design, the same questionnaire and same procedures in all six countries. The development and completion of a sound survey of working conditions and health in Central America represents a significant step towards the development of a permanent regional information system in working conditions and health that could provide reliable data for informed national and regional planning and assessment, and the creation of evidence-based policies directed at preventing occupational risks and promoting workers’ health. While national surveys like Argentina, Uruguay, Chile or Colombia have intrinsic value for specific countries, regional surveys like this have added value, permitting a broader view by allowing comparisons between countries within the region. In the context of the European surveys, both the general situation in Europe and the differences between member states are considered during evaluation of problems and achievements. In the context of Central American integration efforts, the advancement of regional tools and policies to improve working and health conditions is a priority.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online supplement
Footnotes
-
Collaborators Emily Felt, María López, Centro de Investigación en Salud Laboral (CISAL), Universitat Pompeu Fabra (Barcelona); Carlos Santos, Organización Iberoamericana de Seguridad Social (OISS); David Gimeno, The University of Texas School of Public Health (UT) in San Antonio, USA; Marianela Rojas, Freddy Briceño and Patricia Monge, Programa Salud y Trabajo en América Central (SALTRA), Universidad Nacional, Costa Rica; Norma Osiris, SALTRA, Universidad de El Salvador; Carlos Meléndez; Consultor para SALTRA, Universidad de San Carlos (USAC), Guatemala; Lino Carmenate, SALTRA, Facultad de Medicina, Universidad Nacional Autónoma de Honduras (UNAH); Indiana López and Aurora Aragón, SALTRA, Centro de Investigación en Salud, Trabajo y Ambiente (CISTA), Universidad Nacional Autónoma de Nicaragua (UNAN-León); Pedro Vinda, SALTRA, Universidad de las Américas y Caja del Seguro Social, Panamá; Nancy Piedra, Universidad de Costa Rica, San José, Costa Rica.
-
Contributors All coauthors conceptualised the survey and supervised fieldwork. FGB drafted the different versions of the article, and all coauthors critically revised the article for important intellectual content.
-
Funding This study was partially funded by a contract between the Organización Iberoamericana de Seguridad Social and the Universidad Nacional de Costa Rica (Heredia), and also by Fogarty International Center, U.S. National Institutes of Health grant (D4TW00064).
-
Competing interests None.
-
Ethics approval Institutional review boards of the Universidad Nacional in Costa Rica and The University of Texas Health Science Center at Houston..
-
Provenance and peer review Not commissioned; externally peer reviewed.
-
Data sharing statement Data set and questionnaire are available upon request.
-
↵i Encuesta Centroamericana de Condiciones de Trabajo y Salud.
Linked Articles
- Commentary