Article Text

Abstract
Objective Evaluate the effectiveness of two active interventions, aimed at secondary prevention of low back pain (LBP), in occupational health.
Methods We performed a survey of LBP (n=2480; response rate 71%) and randomized 143 employees (66% males, 45 years) with LBP over 34 mm on VAS into Rehabilitation (n=43), Exercise (n=43) or self-care (n=40) groups. Primary outcomes were LBP, physical impairment (PI) and health-related quality of life (HRQoL) for two years and sickness absence (SA) days during four years (LBP specific, total).
Results Compared to self-care, exercise reduced LBP at 12 months (mean difference (MD) −12 mm; 95% CI −21 to −2) and improved HRQoL at 12 and 24 months (0.03; 0.00 to 0.05), but did not reduce PI. The MDs of SA days in four years were −17 (−70 to 35, total) and −15 (−47 to 13, LBP specific). Exercise reduced the probability of LBP specific SA during the third and fourth year. Compared to self-care, Rehabilitation reduced LBP at 3 months (−10 mm; −19 to −1) and 6 months (−10 mm; −20 to − 1), but was not effective in HRQoL or PI. The MDs of SA days in four years were −41 (−93 to 8; total) and 5 (−30 to 47; LBP specific). Rehabilitation reduced the probability of total SA during first and second year and amount of total SA days in the fourth year.
Conclusions Among employees with relatively mild LBP, both interventions reduced pain, but the effects on SA and PI were minor. Exercise improved HRQoL. The effect sizes were rather small.
Trial registration Number ClinicalTrials.gov NCT00908102.
- low back pain
- secondary prevention
- occupational health
- randomised controlled trial
- comparative effectiveness research
- sick leave
- intervention studies
- occupational health practice
- back disorders
- intervention studies
- longitudinal studies
- sickness absence
Statistics from Altmetric.com
- low back pain
- secondary prevention
- occupational health
- randomised controlled trial
- comparative effectiveness research
- sick leave
- intervention studies
- occupational health practice
- back disorders
- intervention studies
- longitudinal studies
- sickness absence
What this paper adds
In the occupational health setting, the effectiveness of active low back pain (LBP) interventions in preventing chronic LBP and work disability is not fully known.
Progressive exercises improved health related quality of life and reduced the probability of LBP specific sickness absence in employees with LBP.
Multidisciplinary, hospital outpatient rehabilitation reduced the probability and length of any sickness absence but not those due to LBP.
Progressive exercises and outpatient rehabilitation had some effect on pain, disability and pain-related fear.
It seems possible to screen non-sick-listed employees with LBP symptoms into preventive intervention, although the optimal strategies need to be determined and further studies are required.
Introduction
Low back pain (LBP) and consequent physical impairment at work have a significant socio-economic impact as a result of temporary and permanent work disability. In industrialised countries, the lifetime cumulative incidence of LBP can be as high as 70% or more, and approximately 10% of cases become chronic. The rates of recurrent LBP are probably higher than those of chronic LBP.1
Occupational health (OH) services, which are located close to workplaces, can be used to promote healthy practices to large groups of adults. Generally, OH services manage the work-related health and safety of employees. In Finland, OH physicians also take care of workers' general health (like family doctors or general practitioners) in addition to issues related to work and work ability, thus acting as an essential part of the national primary care system.
Most prior randomised controlled trials (RCTs) concerning LBP in the OH setting have focused on LBP patients already off work.2–6 In such groups, graded activity programmes (gradual but progressive increases in exercise)7 8 and coordinated (multidisciplinary) care9 10 are known to enhance return to work. Some effect on pain and a decrease in negative work expectations was found in one RCT comparing the effectiveness of physical and behavioural modelling with no intervention among non-sick-listed male railroad workers.11 However, we are not aware of other previous RCTs that have evaluated the effectiveness of multidisciplinary or graded activity interventions among non-sick-listed workers in the OH setting.
At the time of designing the present study, a Cochrane systematic review12 recommended at least 100 h of multidisciplinary rehabilitation for chronic LBP. On the other hand, there was also evidence supporting the use of graded activity or other exercise programmes13 14 for LBP. Moreover, it was already recognised that carefully selected and presented information and advice about LBP can have a positive effect on patients' beliefs and clinical outcomes.15
In the present pragmatic trial we analysed the effectiveness of two active secondary prevention interventions (hospital outpatient rehabilitation and progressive back exercises, i.e., a graded exercise programme) compared to self-care advice. Our study was implemented in the occupational setting and self-care advice was provided by an occupational physician (OP). Primary outcomes were pain, physical impairment and health-related quality of life (HRQoL) at 2-year follow-up, and sickness absence (SA) over a 4-year follow-up.
Methods
Study design and ethics
This was a longitudinal cohort study with two embedded RCTs. All employees in a forestry company were invited to respond to a postal questionnaire on LBP and back-related physical impairment. Based on the responses, the employees were divided into three main categories: ‘no’ low back (LB) symptoms, ‘some’ LB symptoms and ‘LB symptoms potentially hampering work’. Two RCTs were performed in the subjects with some LB symptoms and with LB symptoms potentially hampering work, respectively. The present study describes the results of a trial with three arms after screening for employees with LB symptoms potentially hampering work. The South Karelian Central Hospital Research Ethics Board approved the study, and it was performed according to the Declaration of Helsinki.
Participants
The study was performed within one forestry company production unit in the city of Lappeenranta, Finland. The production unit includes a chemical mill, a pulp mill, a paper mill, a plywood mill, a saw mill and a planing plant. A structured questionnaire on LBP and related items was sent to the entire workforce (n=2480) listed in the company registers in September 2001.
The mean (SD) age of the 1754 respondents (71% response rate) was 45 years (18–64 years), 70% were blue-collar workers and 28% were female. Some 20% reported heavy, 36% moderate and 44% light work strain.
Inclusion criteria were age, presence of LBP and pain intensity. Based on the responses to the screening questionnaire, a group of 193 employees under the age of 57 were identified as having LBP symptoms ‘potentially hampering work’. They had to fulfil at least one of the following criteria:
LBP lasting 2 weeks or more in the past 12 months
Radiating LBP at the time of responding to the questionnaire
Recurrent LBP (two or more episodes irrespective of their duration during the past 12 months)
Self-reported work absence because of LBP during the past 12 months.
In addition, they had to report an LBP intensity of 35 mm or more on a 100 mm visual analogue scale (VAS) during the past week.
Of these 193 employees, a random sample of 50 individuals formed a control group representing the natural course of LBP without any intervention. Data for the natural course group are not given in this paper.
The remaining 143 employees with LBP were invited to visit an OP (the first author) for a clinical examination. Exclusion criteria for the study were retirement, pregnancy, presence of acute nerve root entrapment, suspicion of malignancy, recent fracture, severe osteoporosis or other specific diseases preventing participation in the follow-up.
The study design, implications of the trial and alternative options were explained in the informed consent form, which emphasised that taking part in the trial was voluntary: employees would still get the best treatment and the full attention of the OP even if they did not participate and participants were free to withdraw from the trial at any point, and it would not prejudice their treatment.
Of the eligible subjects, 17 refused to participate. As none were excluded due to exclusion criteria, the remaining 126 subjects formed the study group for randomisation. The intervention groups were comparable regarding most basic characteristics (table 1).
Baseline characteristics of study subjects
Randomisation and blinding
An independent biostatistician prepared the randomisation scheme using a computer-generated randomisation table. To prevent unequal randomisation of subjects by age and gender in the treatment arms, scripted four-digit identification codes (ID) were sorted by gender and age (≤45 years, >45 years), resulting in four strata. Block randomisation (with blocks of 15) was applied to ensure equal group sizes within each stratum. Based on the randomisation scheme, before the start of the study a research assistant prepared sealed envelopes containing either a referral to the outpatient rehabilitation at the hospital group, the progressive back exercise group or the self-care advice group. After signing the informed consent form, each employee opened a sealed envelope. The research personnel were not able to identify the IDs or the group assignments before randomisation. Due to the nature of the interventions, the participants and OH professionals were not blinded for the group assignment after randomisation. SA data were extracted from the electronic records of the OH services and self-reported data were entered into the computer by a research assistant, which ensured blinded analysis of the data by the researchers.
Interventions
All subjects had access to OH care as usual during the study period. At the first study visit to the OP, subjects were randomised into the intervention groups (described below) and all received information about LBP, the trial and the follow-up.
Information about the study was also provided regularly in the company magazine and intranet; at the time of the study, no other specific OH or other health interventions were being carried out in the company. The OH unit of the company operated as usual during the study period.
Outpatient rehabilitation at the hospital physical medicine unit (PMU)
Intensive, bio-psychosocial and multidisciplinary LBP rehabilitation was carried out at the physical medicine outpatient unit of the South Karelian Central Hospital in the city of Lappeenranta, Finland.16 The rehabilitation team consisted of a specialist doctor in physical medicine and rehabilitation, a psychologist, a social worker and several physiotherapists. The program included a 3-week pre-course of 1.5 h light mobilisation and exercise sessions for 3 days each week, followed by an intensive 3-week course that included progressive exercises and multidisciplinary information about LB syndrome and pain management. The rehabilitation program lasted for 6.5 h each day for 5 days each week, that is 15 days altogether. Finally, a personal maintenance exercise program was designed for the subjects and they were later invited to a follow-up visit within 6 months of the initial course. The subjects were not sick-listed during the 3-week intensive period, but were effectively out of work and received compensation from the Social Insurance Institution of Finland. The costs of the course were covered by the public health care budget. Outpatient rehabilitation at a hospital PMU is a widely used method to treat persistent LBP in Finland.
Progressive back specific exercises (DBC)
A graded activity program was carried out in a physiotherapy outpatient clinic.13 17 It consisted of a 1 h session twice or three times a week, over a period of 12 weeks, supervised by a specially trained physiotherapist. The treatment included exercises targeted at the trunk muscles using specific equipment together with stretching and relaxation. The physiotherapists emphasised the ‘good prognosis’ for LBP during the treatment sessions and the subjects were instructed in performing LB exercises at home. The importance of home exercises was emphasised during the exercises.
Self-care advice by an OP based on the Back Book (BB)
During the visit to the OP, the findings of the clinical examination were explained to the subject. The employee was given a copy of the Back Book15 and the OP explained the contents of the booklet, emphasising the benign nature of and good prognosis for LBP. The Back Book focuses on patients' beliefs and pain management and encourages staying active in spite of LBP. The booklet also offers practical advice for patients suffering from an acute or subacute LBP episode. We implemented the self-care advice as a low-cost control intervention.
Outcome measures and data collection
After randomisation, participants were followed up for 24 months for the questionnaire data and for 48 months for the SA data.
Primary outcome measures
Pain intensity, physical impairment, HRQoL and SA days were the primary outcomes of this study. The follow-up questionnaires included the following previously validated and widely used items: intensity of LBP (VAS18) during the preceding week, physical impairment measured using the Roland–Morris 18-item scale (RM-18)19 and Health related quality of life, HRQoL (15D).20
SA data were obtained from the electronic medical records of the OH services. Records were carefully checked for inconsistencies and maternity or paternity leave and absence to care for a sick child were not included. SA days were analysed in two ways, according to (1) LBP specific SA days with no time limit or (2) any (=total) SA days, that is the sum of ‘LB specific’ and ‘other’ SA days. Among non-LB specific SAs, periods longer than 30 days were omitted from the category in order to prevent severe diseases and the consequences of injury confounding the analyses. The cut-off limit of 30 days per SA period was chosen arbitrarily before conducting any analyses.
Secondary outcome measures
Disability (ODI, Oswestry Disability Index),21 depressive symptoms (Depression Scale, DEPS),22 fear avoidance (Fear-Avoidance Beliefs Questionnaire, FABQ)23 and SA periods were the secondary outcomes of this study. ODI, DEPS and FABQ scores were collected from the follow-up questionnaires. The data for the SA periods were calculated in the same way as for the SA days above (see ‘Primary outcome measures’ section).
Power calculations
A power calculation for the difference in LBP intensity (VAS) was carried out. The SD was expected to be 15 units (mm). Calculations showed that differences in LBP intensity of 10 mm between groups would be detectable with 80% power in two-tailed tests with a significance level of 0.05 for a sample of 40 employees in each group.
Statistical analyses
All statistical analyses were performed at employee level, according to the intention-to-treat principle. Missing questionnaire data were imputed using the last observation carried forward principle. Baseline characteristics were compared using descriptive statistics. The effectiveness of the interventions was primarily estimated by the difference in the outcome variables between the two active interventions and the control group (PMU vs BB; DBC vs BB) at 3, 6, 12 and 24 months for the questionnaire variables and at 12, 24, 36 and 48 months for the SAs. The 95% CIs for the mean differences between groups were computed using the generalised linear model where the respective baseline values were used as covariates (when appropriate). We used the statistical package SPSS 17.0 for Windows.23
As regards the SA variables, we tested different observational models and hierarchical latent regression models. Count data are commonly modelled using Poisson, negative binomial and corresponding zero inflated models. For all SA variables there was great overdispersion in relation the Poisson model and an excess of zeros in relation to the non-inflated models. We therefore used a two-component hurdle model24 where the first process determines whether a person has any SAs and the second determines the number of SA periods or days. In the zero component, the latent function models the logit of the probability that SA days or periods are larger than zero. In the count component, the latent function models the log of the mean parameter of the zero truncated negative binomial. We tested both linear and non-linear models with different hierarchical structures. The final choice for both latent models was a hierarchical Gaussian process model with a neural network covariance function.25 26 The constructed hierarchical model27 included a common effect, an effect for the baseline, effects for each intervention group and effects for each person (also called ‘random effects’). For the logistic model, we report the probabilities of SAs and the odds ratios. For the zero truncated negative binomial model, we report mean SA days or periods and mean ratios. The Gaussian process models were implemented using the GPstuff toolbox (http://www.lce.hut.fi/research/mm/gpstuff/).26 Additional details are provided in the online statistical appendix.
Results
Employee flow
Figure 1 shows the flow of participants in this trial. A total of 126 employees were randomised to outpatient rehabilitation at the hospital (PMU, n=43), progressive back specific exercises (DBC, n=43) or self-care advice (BB, n=40).

Flow diagram of the course of the study showing the number of subjects at different phases of the trial. BB, Back Book intervention group; DBC, progressive back specific exercises group; PMU, hospital physical medicine unit group.
Primary outcomes
The results are shown in table 2.
Results of primary and secondary outcomes (questionnaire variables) and comparisons between the active intervention groups and the control group (BB) at the 2-year follow-up
Pain and physical impairment
At 3 and 6 months, PMU was more effective compared to BB regarding pain (mean difference (MD) at 3 months: −10 mm (95% CI −19 to −1); MD at 6 months: −10 mm (95% CI −20 to −1)), but was no longer effective at 12 months (MD: −7 mm (95% CI −21 to 2)).
At 3 months, MD for DBC versus BB regarding pain was −6 mm (95% CI −16 to 3) and at 6 months −4 mm (95% CI −14 to 5). At 12 months, DBC was more effective regarding pain (MD for DBC vs BB −12 mm (95% CI −21 to −2)) than BB.
The active interventions were not effective in reducing physical impairment (RM-18) during follow-up from 3 to 24 months compared to self-care advice (MDs at 3 months: PMU vs BB −1 (95% CI −2 to 1); DBC vs BB 0 (95% CI −1 to 2)).
At 24 months, no relevant differences were seen between the treatment arms regarding pain (MDs for PMU vs BB −5 mm (95% CI −13 to 4); DBC vs BB −5 mm (95% CI −13 to 4)) or MD regarding physical impairment (PMU vs BB −1 (95% CI −3 to 0); DBC vs BB −1 (95% CI −3 to 1)).
HRQoL
HRQoL (15D) improved in the DBC group towards the end of the follow-up period (MDs of DBC vs BB were 0.03 (95% CI 0.00 to 0.05) at 12 and 24 months).
Sickness absence
The results are shown in figures 2 and 3.

Total sickness absence (SA) by years: a hurdle model where the first (logistic) component determines whether a person has any SA and the second (zero truncated Negbin) component determines the total number of SA days or periods over the 4-year follow-up period. (A) Probability and 95% CI of any SA by groups; (B) comparisons of the probability of any SA between the intervention groups (PMU and DBC) and the control group (BB) (OR and 95% CI); (C) total number of SA days by groups (mean and 95% CI); (D) comparisons of the total number of SA days between the intervention groups and the control group (mean ratio with 95% CI); (E) total number of SA periods by groups (mean and 95% CI); (F) comparisons of the total number of SA periods between the intervention groups and the control group (mean ratio with 95% CI). BB, Back Book intervention group; DBC, progressive back specific exercises group; PMU, hospital physical medicine unit group.

{kind=link}
{kind=link}
{kind=link}
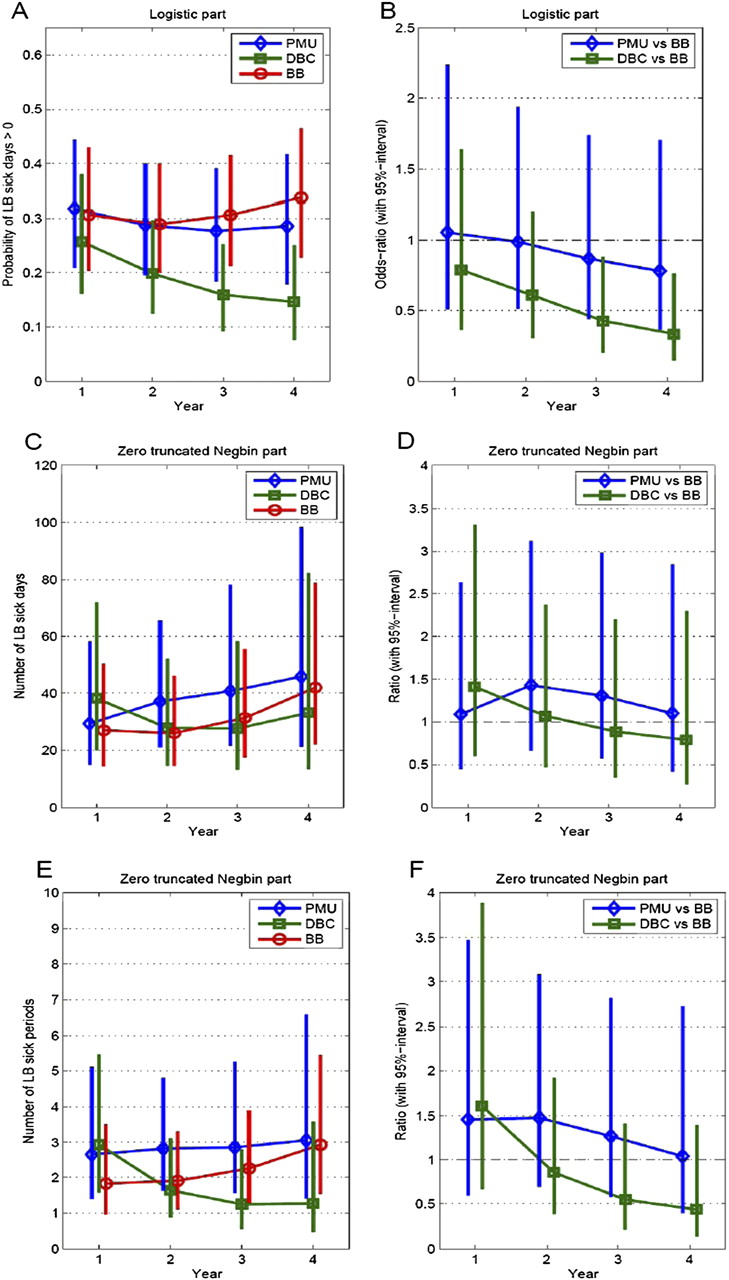
Low back pain (LBP) specific sickness absence (SA) by years: a hurdle model where the first (logistic) component determines whether a person has any LBP specific SA and the second (zero truncated Negbin) component determines the number of LBP specific SA days or periods over the 4-year follow-up period. (A) Probability and 95% CI of LBP specific SA by groups; (B) comparisons of the probability of LBP specific SA between the intervention groups (PMU and DBC) and the control group (BB) (OR and 95% CI); (C) number of LBP specific SA days by groups (mean and 95% CI); (D) comparisons of the number of LBP specific SA days between the intervention groups and the control group (mean ratio with 95% CI); (E) number of LBP specific SA periods by groups (mean and 95% CI); (F) comparisons of the number of LBP specific SA periods between the intervention groups and the control group (mean ratio with 95% CI). BB, Back Book intervention group; DBC, progressive back specific exercises group; PMU, hospital physical medicine unit group.
The MD between PMU and BB in total SA days over 4 years was −41 (95% CI −93 to 8). In comparison to BB, PMU reduced the probability of total SA during the first (OR 0.34 (95% CI 0.14 to 0.81)) and second (OR 0.41 (95% CI 0.19 to 0.88)) follow-up years (figure 2B). Among those who had had any SA, the number of SA days was lower in PMU than BB during the fourth year (mean ratio (MR) 0.53 (95% CI 0.31 to 0.92)) (figure 2D).
The MD between DBC and BB in total SA days over 4 years was −17 (95% CI −70 to 35). No difference in the probability or total number of SA days was found between DBC and BB (figure 2).
The MD between DBC and BB in LBP specific SA days over 4 years was −15 (95% CI −47 to 13). In comparison to BB, DBC reduced the probability of LBP specific SA during the third (OR 0.24 (95% CI 0.07 to 0.81)) and fourth (OR 0.16 (95% CI 0.04 to 0.62)) follow-up years (figure 3B). Among those who had had any LBP specific SA, no difference was found in the number of LBP specific SA days between DBC and BB (MRs from 0.78 to 1.42).
The MD between PMU and BB regarding LBP specific SA days over 4 years was 5 (95% CI −30 to 47). No difference in the probability or the number of LB specific SA days was found between PMU and BB (figure 3).
Secondary outcomes
Questionnaire variables
The results are presented in table 2.
Disability (ODI) was lower in the PMU group compared to the BB group at 3 and 24 months (3 months: −4% (95% CI −8% to 0%); 24 months: −5% (95% CI −10% to −1%)).
Pain related fear (FABQ) was lower in both active treatment arms compared to self-care information towards the end of the 24-month follow-up period.
Depression score (DEPS) was lower in the DBC group at 24 months compared to the BB group (−2 (95% CI −4 to 0)).
Sickness absence (SA) periods
Among those who had had any SA, PMU reduced the number of SA periods during the third (MR 0.6 (95% CI 0.41 to 0.89)) and fourth (MR 0.44 (95% CI 0.27 to 0.71)) years in comparison to BB (figure 2F). No such difference was found between DBC and BB.
Among those who had had any LB specific SA, no difference was found in the number of SA periods between either of the active interventions and BB (figure 3F).
Adverse effects
No adverse events were reported during the interventions.
Discussion
Main findings
Progressive back specific exercises improved HRQoL at the 12-month and 24-month follow-up time points, reduced the probability of LB specific SA during the third and fourth follow-up years, and were more effective for pain than self-care at 12 months. Outpatient rehabilitation at the hospital reduced the probability of any SA days during the first 2 years, reduced the number of SA days in the fourth year, the number of SA periods in the third and fourth year and was more effective for pain at 3 and 6 months than self-care advice. Disability and pain related fear decreased in both active groups and depression in the Progressive back exercises group, as compared to self-care information over 2 years.
The effect sizes were rather small, which is partly explained by the low baseline levels of the outcome variables in our trial.
Strengths and weaknesses of the study
The main strength of the study lies in the pragmatic approach of this RCT. All permanent employees in the target cohort were initially offered the opportunity to participate in the questionnaire survey. The response rate was reasonably high at 71%. Selection of eligible employees for the trial was based on straightforward criteria: LBP frequency, duration and intensity of pain and self-reported SA due to LBP. Our intention was to include subjects who had periodic or chronic LBP potentially hampering work but not yet preventing it. The study population was somewhat heterogeneous concerning LBP severity, although symptoms were generally mild.
Only 17 (12%) of the 143 eligible participants refused to take part. Randomisation was successful and the treatment arms were comparable regarding the relevant demographic factors.
The employees' own OP carried out the baseline clinical examination and provided advice about the self-care intervention. Adherence to the trial was reasonably high, although loss to follow-up was somewhat unequal between the treatment arms (figure 1). All interventions were based on existing clinical practice, and experimental methodologies were not introduced. We selected a representative sample of some 10–15% of the employees with the most severe LB symptoms in the cohort; however, most participants in our study had only relatively mild symptoms.
The questionnaire variables were based on previously validated and widely used techniques but have been primarily used in patients with more severe symptoms.
One of the primary outcomes was based on recorded SAs. This has several advantages: good coverage, accuracy and consistency.28 As salaries and other employee benefits in this company are based on the same absence data that we used in our study, SA records are very accurate and consistent. However, the fact that our study is somewhat underpowered as regards SA variables can, for example, be seen from the broad confidence intervals in the differences between the treatment arms.
During the study follow-up period (2002–2005), the number of LB specific SA was stable or slowly increasing at the national level in Finland.29 At the same time, according to company registers, the total SA rate remained stable at approximately 5–5.5% of the theoretical working hours per year. There were no major job losses or other threats facing personnel or the financial performance of the company during the study follow-up period. The turmoil that affected the entire Finnish forestry industry effectively started shortly after our data collection ended. Nevertheless, any potential external confounding factors would have influenced the treatment arms equally.
Some differences compared with previous studies
The majority of previous RCTs in OH settings concerning LBP have been performed with selected groups of employees already on sick leave. In a Finnish RCT, male railroad employees with LBP were invited into a trial on the basis of OH registers.11 The subjects were randomised into physical training or usual care. The baseline pain and disability levels were even lower than in our study. The main results were a slight decrease in pain at 12 months and an increase in subjective future work ability.11 The inclusion criteria in that study were somewhat comparable to those in our study, and the results in both studies indicate some effectiveness of active interventions regarding symptoms in moderately symptomatic subjects.
In a 12-month follow-up study, a graded activity intervention (comparable to DBC in our study) improved the return to work rate but was ineffective in improving functional status or reducing pain among workers who had been on full or partial sick leave because of LBP for at least 4 weeks prior to inclusion in the study.7 There was a substantial reduction in the total number of sick leave days compared to the usual care group, but the difference was statistically insignificant. The authors suggest that this may be because the trial was underpowered for the inherently skewed nature of length of sick leave distributions or cost savings.5 In another study with a 6-month follow-up, a low-intensity back school was more effective in reducing work absence than a high-intensity back school or usual care, among workers sick-listed due to subacute LBP.30 The effects of treatment on functional status and kinesiophobia were borderline significant, a result which also favours low-intensity intervention. Pain relief did not differ between the groups. Some previous studies have shown the effectiveness of a coordinated return-to-work programme for sick-listed employees with LBP.6 31 However, as these programmes also include a workplace intervention for employees already sick-listed, they are not directly comparable with our study.
Numerous other studies31–37 and a Cochrane review38 on the (secondary) prevention of LBP with various designs and settings other than OH have resulted in decreases in pain, fewer recurrent LB episodes, less disability, etc, after physical activity, psycho-educational or multidisciplinary interventions or combinations of these.
In a recently published RCT, a targeted OH intervention was found to be effective regarding SA among workers at high risk of SA, defined by self-rated symptoms irrespective of baseline SA, when compared to usual care.39 The targeted OH intervention was also cheaper.40 Exploratory analyses in the trial indicated that the targeted intervention was especially effective for those workers who were certain that they would be unable to continue working in their current job for health reasons and had co-morbidities or severe physical impairment at work.41
In summary, only a few RCTs in the OH setting have attempted to identify non-sick-listed employees at risk of LBP-related disability and then set up an intervention for these individuals. These studies all show some effectiveness, but the effect sizes have been rather small. The optimal strategies for secondary prevention of LBP related disability need to be determined.
Conclusions and implications for future trials
Two active interventions focused on non-sick-listed employees selected from their workplace, resulted in improved HRQoL and less LBP, disability and pain related fear. However, the small decrease in pain was not sustained over the 2-year follow-up period, the borderline improvement in quality of life was only realised after 1-year of follow-up and the effects on SA were minor. The small decrease in the probability and number of any SA days with multidisciplinary rehabilitation at the hospital was not reflected in LB specific sick leave. Although the included subjects were drawn from among the 10% most symptomatic respondents, they still experienced relatively mild LB symptoms. One reason for the modest effect sizes may be related to the inclusion in the study of non-sick-listed employees with low baseline values.
Although outpatient rehabilitation at the hospital showed the best results in reducing SA, its cost-effectiveness must be further evaluated before it is recommended for widespread use in similar populations. Further research on this topic is warranted. In order to identify the most suitable subjects for secondary prevention, patient selection criteria and the optimal intervention strategy need to be determined.
References
Supplementary materials
Web Only Data oem.2009.054312
Files in this Data Supplement:
Footnotes
See Editorial, p 1
Funding Centenary Foundation of Kymi Corporation, Yrjo Jahnsson Foundation, Juho Vainio Foundation and Finnish Cultural Foundation funded the research at the beginning of this study. The authors' work is independent of the funders.
Competing interests JR, SL, JK, AV and AM have no competing interests to declare. During physical medicine unit (PMU) interventions, MH was the head physician of the PMU. ST is the Medical Director of DBC International.
Ethics approval The South Karelian Central Hospital Research Ethics Board approved this study (record number (Dnr) A18/01).
Provenance and peer review Not commissioned; externally peer reviewed.