Article Text

Abstract
The objective was to provide a systematic literature review on associations between poor health and exit from paid employment through disability pension, unemployment and early retirement, and to estimate the magnitude of these associations using meta-analyses. Medline and Embase databases were searched for longitudinal studies on the relationship between health measures and exit from paid employment. Random-effects models were used to estimate the pooled effects. In total, 29 studies were included. Self-perceived poor health was a risk factor for transition into disability pension (relative risk (RR) 3.61; 95% CI 2.44 to 5.35), unemployment (RR 1.44; 95% CI 1.26 to 1.65) and early retirement (RR 1.27; 95% CI 1.17 to 1.38). Workers with mental health problems had an increased likelihood for transition into disability pension (RR 1.80; 95% CI 1.41 to 2.31) or unemployment (RR 1.61; 95% CI 1.29 to 2.01). Chronic disease was a risk factor for transition into disability pension (RR 2.11; 95% CI 1.90 to 2.33) or unemployment (RR 1.31; 95% CI 1.14 to 1.50), but not for early retirement. This meta-analysis showed that poor health, particularly self-perceived health, is a risk factor for exit from paid employment through disability pension, unemployment and, to a lesser extent, early retirement. To increase sustained employability it should be considered to implement workplace interventions that promote good health.
Statistics from Altmetric.com
Introduction
In most Western countries a higher and prolonged labour force participation throughout a worker's life is necessary to safeguard the social and economic realities of an aging society. In order to achieve this ambition, governments are developing policies to stimulate labour force participation, particularly to keep workers in the workforce till older age.1–4
The success of the developed policies depends on better understanding of the relationship between the impact of health on labour force participation.5 In the past few years several studies have demonstrated that health status may have a profound impact on the ability of workers to be actively engaged in paid employment and to prolong their meaningful contribution to a productive society. There is evidence from different longitudinal studies that poor health plays a role in exit from paid employment, due to disability pension,6–9 unemployment8 ,10 ,11 and early retirement.8 ,10 ,12 A community based survey in the UK found evidence for health related job loss, especially in relation to musculoskeletal disorders and mental illness.13 Pedersen et al6 demonstrated that the risk of transition (from employment, unemployment or sickness absence) into disability pension was increased in those with a chronic disease. However, the risk of transition from work into unemployment was lower in those with a chronic disease. A prospective register study, with 15 years follow-up, in a cohort of nurses’ aides found that risk factors for disability pension were mainly health related (eg, low back pain, sick leave spells), whereas economic factors (eg, income of spouse) influence the decision to retire early.14 A recent meta-analysis showed evidence for the association between important health behaviour factors and exit from paid employment. Obese, and to a lesser extent overweight, workers had an increased likelihood of exit from paid employment through disability benefit. Workers with lack of physical activity had an increased risk of disability benefit and unemployment.15
The impact of various health measures on exit from paid employment suggests that these measures differ between the main pathways of leaving the labour force, particularly between the involuntary (ie, disability pension, unemployment) and more voluntary routes (ie, early retirement) of exit from work. In order to understand and quantify the importance of different health measures on labour market exit pathways, the literature needs to be synthesised. Therefore, our aim was to provide a systematic literature review of the associations between different health measures and exit from paid employment through disability pension, unemployment and early retirement, and to estimate the magnitude of these associations using meta-analyses.
Materials and methods
Literature search
Comprehensive literature searches were conducted by the first author (RMvR) in Medline, Embase and Web of Science (inception of databases to July 2013). The following keywords were used: health, work related, early-retirement, unemployment, disability pension, study design. The full search strategy is presented in online supplementary appendix I.
Based on title and abstract one reviewer (RMvR) selected the articles for full text appraisal. Two reviewers (RMvR, SJWR) independently selected articles for final inclusion. Each article had to fulfil all of the following criteria: (1) a health measure was described, (2) exit from paid employment was defined as receiving disability pension, unemployment or early retirement, (3) the association between health and exit from paid employment was expressed in an OR, relative risk (RR) or HR, or sufficient raw data was available to calculate associations, (4) a longitudinal study design was used, (5) the study had to involve a non-patient population, and (6) the article was published in a peer reviewed scientific journal written in English. A consensus method was used to resolve disagreements.
Data extraction
Relevant information on study population (age, gender, sample size), health measures, exit routes from paid employment and measures of associations with corresponding CI were extracted from the included articles by the first author (RMvR). The core findings in each article were expressed by measures of associations (OR, RR or HR) with corresponding 95% CIs. Where possible, these associations were directly extracted from the original article. For articles in which this information was not presented, associations calculated using raw data were provided.
Data analysis
Heterogeneity of the included studies was determined using the I2 statistics, which indicates the percentage of total variation across studies that is due to heterogeneity rather than chance.16 Due to observed heterogeneity (I2>50% for disability pension) we conducted random-effects meta-analyses of the health effects on disability pension, unemployment and early retirement. Random-effects meta-analysis assumes that there are real differences between individual studies regarding the magnitude of the association between health determinants and exit from paid employment. It considers between-study and within-study variability.17 We used an Excel spreadsheet for pooling of RRs.18 In the meta-analysis we used measures of association that were adjusted for potential confounders, as presented in the original articles. An OR or HR was considered as approximation of RR when the frequency of outcome event was less than 10%. A higher frequency of events will lead to an OR that substantially overestimated the RR.19 ,20 Population attributable fractions (PAF) were calculated for significant determinants of exit from paid employment, using the formula PAF=Pe(RR−1)/(1+Pe(RR−1)) where Pe represents the prevalence of health problems in the study population.21
Results
Characteristics of the included studies
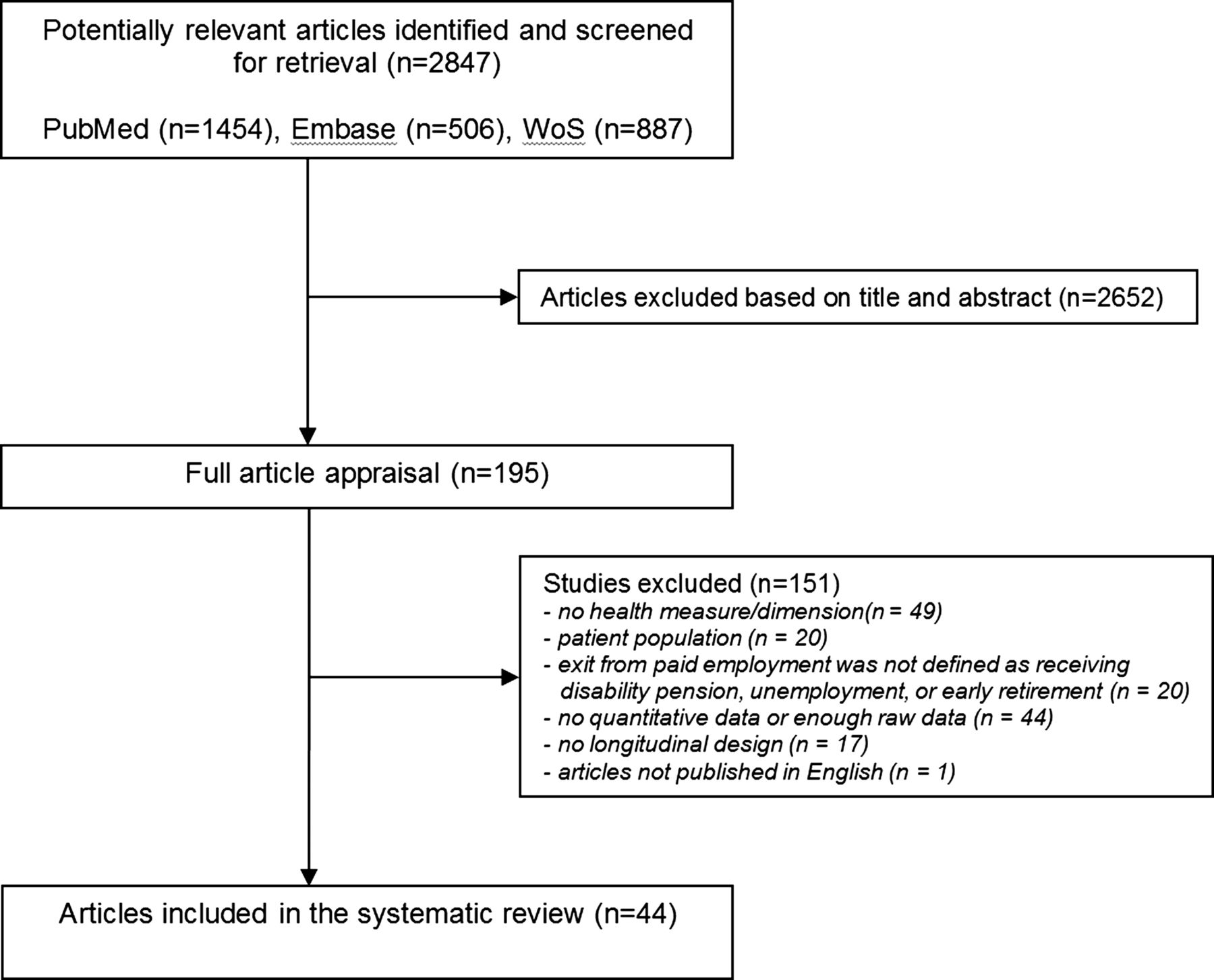
Our search of the literature resulted in 2847 potentially relevant articles (figure 1). After title and abstract screening, 195 articles were retrieved for full text appraisal. Finally, 44 articles were included describing the influence of health on the risk of disability pension (n=29), unemployment (n=17) and early retirement (n=9). Exclusion of articles was mainly due to lack of health measures (n=49), absence of quantitative data (n=44) or study population restricted to a specific patient group (n=20). Several studies provided more than one measure of association and thus the sum of associations presented exceeds the number of included articles, for disability pension (self-perceived health: n=13, mental health: n=29, chronic disease: n=42), unemployment (self-perceived health: n=14, mental health: n=15, chronic disease: n=25) and early-retirement (self-perceived health: n=6, chronic disease: n=22). No studies were found on the association between mental health problems and exit through early retirement. In 12 articles no measure of association was presented, therefore we used the available raw data to calculate an OR with 95% CI.9 ,11 ,22–31
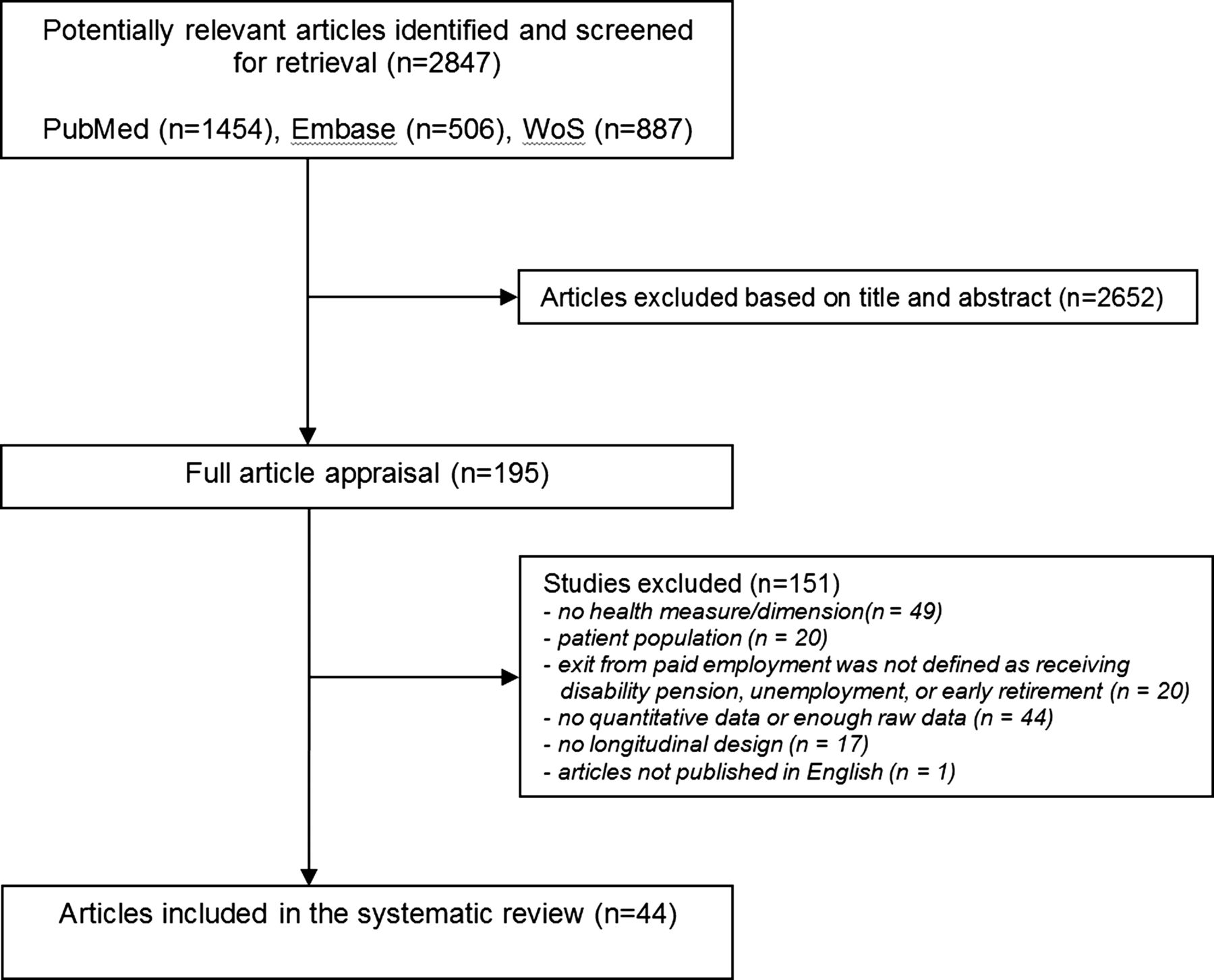
Flow chart of the included studies.
Disability pension
Twenty-nine studies reported on the impact of health on the risk of disability pension (see online supplementary appendix II).7–9 ,14 ,23–28 30–48 In 23 out of 29 studies the frequency of events was less than 10%, therefore OR and HR were considered as an approximation of RR.
Self-perceived health was evaluated in 12 studies,7–9 ,23 ,24 ,26 ,30 ,36 ,37 ,43 ,46 ,48 presenting 13 associations. In all 12 studies self-perceived poor health was a significant risk factor for transition into disability pension (table 1) with a pooled RR of 3.61 (95% CI 2.44 to 5.35), table 2 and figure 2. Poor health was measured on a 5-point Likert scale,7–9 ,26 ,43 ,46 a 4-point Likert scale23 ,24 ,48 or with the short-form health survey (SF-12 or SF-36).30 ,36 In eight studies poor health was defined as ‘less than good health’,7–9 ,24 ,30 ,43 ,46 ,48 whereas the other studies defined poor health as ‘less than fair health’,23 ‘less than moderate health’26 or as a cut-off value <40 on the SF-36.36 Explorative analysis showed no influence of different cut-off values on pooled estimates of self-perceived poor health (‘less than good health’: RR 3.08, 95% CI 1.94 to 4.88; ‘less than fair/moderate health’: RR 4.07, 95% CI 1.70 to 9.71).
Summary of associations between health measures and exit routes from paid employment as presented in the studies included in this systematic review
Pooled relative risks (RRs) of health measures for disability pension, unemployment and early retirement

Association between self-perceived poor health and disability pension, unemployment and early retirement.
Seventeen studies investigated the influence of mental health problems on the risk of disability pension, presenting 29 associations (table 1).23 ,24 ,26 ,28 ,30–38 ,40 ,44 ,45 ,47 In 18 out of 29 associations mental health problems were a significant risk factor resulting in a pooled RR of 1.80 (95% CI 1.41 to 2.31) across 29 associations (table 2).
In 13 studies the influence of chronic diseases on the risk of disability pension was evaluated, presenting 42 associations (table 1).14 ,23 ,24 ,26 ,27 ,34–36 ,38 ,39 ,41–43 In 35 out of 42 associations chronic disease was a significant risk factor with a pooled RR of 2.11 (95% CI 1.90 to 2.33) across the 42 associations. A large part of the associations reported on musculoskeletal disorders (25 out of 42), resulting in pooled RR of 2.23 (95% CI 1.93 to 2.59, table 2).
The PAF of self-perceived poor health, mental health problems and chronic diseases for transition into disability pension ranged from 3.9% to 76.8%, from 0% to 48.6% and from 1.6% to 69.9%, respectively (figure 3). Within the group of chronic diseases, we made a distinction between musculoskeletal disorders, respiratory diseases and other chronic disease, resulting in PAFs ranging from 1.2% to 69.9%, from 1.7% to 14.5% and from 0.7% to 40.1%, respectively.

{kind=link}
{kind=link}
{kind=link}
Relation between relative risk (RR) and population attributable fraction (PAF) for each health dimension and each pathway of leaving the labour force. Mean PAFs were calculated and reported with their range (error bars). ▪=disability pension, •=unemployment, Δ=early retirement.
Unemployment
Seventeen studies investigated the influence of health on the risk of unemployment (see online supplementary appendix III).7 ,8 ,10 ,11 ,22 ,29 ,36 ,39 ,43 ,49–56 In 14 out 17 studies the frequency of events was less than 10%, therefore OR and HR were considered as an approximation of RR.
Self-perceived health was evaluated in 10 studies, presenting 14 associations.7 ,8 ,11 ,22 ,29 ,36 ,43 ,48 ,53 ,55 In 9 out of 14 associations self-perceived poor health was a significant risk factor for unemployment (table 1). Three studies presented results for different subgroups. Jusot et al51 reported no differences between men and women, poor health was found to be a precursor of unemployment in both genders. Liira and Leino-Arjas53 reported that a self-perceived poor health was a statistically significant risk factor for unemployment in construction workers (OR 2.15, 95% CI 1.30 to 3.56), but not in forestry workers (OR 1.49, 95% CI 0.67 to 3.28). Schuring et al11 found that self-perceived poor health was a statistically significant risk factor for unemployment in low and intermediate educated people, but not in highly educated people. Pooling of all studies resulted in a RR of 1.44 (95% CI 1.26 to 1.65, table 2).
Seven studies described the influence of mental health problems on the risk of unemployment, within a total of 15 associations (table 1).29 ,36 ,46 ,52–54 ,56 In 10 out of 15 associations mental health problems were a significant risk factor of unemployment with a pooled RR of 1.61 (95% CI 1.29 to 2.01) across all 15 associations (table 2).
Seven studies investigated the influence of chronic diseases on unemployment presenting 25 associations with RR varying from 0.90 to 2.20 (table 1).22 ,36 ,39 ,43 ,49 ,52 ,53 In 4 out of 25 associations a chronic disease was a significant risk factor for unemployment. In the meta-analysis the association between chronic disease and unemployment was statistically significant (pooled RR of 1.31, 95% CI 1.14 to 1.50) (table 2).
The PAF of self-perceived poor health, mental health problems and chronic diseases for transition into unemployment ranged from 2.2% to 14.2%, from 0.0% to 32.7% and from 0.0% to 9.9%, respectively (figure 3).
Early retirement
Nine studies investigated the influence of health on the risk of early retirement (see online supplementary appendix IV).7 ,8 ,10 ,14 ,39 ,43 ,57–59 In six out of nine studies the frequency of events was less than 10%, therefore OR and HR were considered as an approximation of RR.
Self-perceived health was evaluated in five studies, presenting six associations (table 1). 7 ,8 ,43 ,58 ,59 In four out of six associations self-perceived poor health was a significant risk factor of early retirement, resulting in a pooled RR of 1.27 (95% CI 1.17 to 1.38) (table 2).
No studies reported on the association between mental health problems and exit through early retirement.
Five studies investigated the influence of chronic diseases on early retirement, presenting 22 associations (table 1).14 ,39 ,43 ,57 ,59 In 6 out of 22 associations a statistically significant association between chronic disease and early retirement was reported. Pooling of all five studies resulted in a RR of 1.10 (95% CI 0.99 to 1.21) (table 2).
The PAF of self-perceived poor health and chronic diseases for transition into early retirement ranged from 0.8% to 11.1% and from 0.0% to 7.5%, respectively (figure 3).
Discussion
This meta-analysis shows that poor health increases the risk of exit from paid employment due to disability pension, unemployment and early retirement. The relative importance differed by pathway of exit from paid employment. The strongest associations were found for exit from paid employment through disability pension, followed by unemployment and, to a lesser extent, early retirement. Self-perceived poor health had a stronger effect on displacement through disability pension than mental health problems and presence of a chronic disease. The PAFs were largest for self-perceived poor health on disability pension, and for chronic diseases on disability pension and unemployment, indicating that good health and not having a chronic disease are important factors in maintaining paid employment.
Poor health, particularly self-perceived poor health, is a risk factor for exit from paid employment, especially through disability pension. The strong relation between self-perceived poor health and disability pension is not surprising, since health problems are a requirement for receiving a disability pension. However, eligibility of a disability pension does not depend on health problems alone, but also on individual, social, economic and legal factors.60 ,61 For example, the relationship between poor health and unemployment is consistent across Europe, but seems to vary across the type of welfare state regime. A study by Van der Wel et al found that the likelihood of non-employment was consistently lower in the Scandinavian welfare state regime type. The protective effect of welfare regimes reducing the risk of non- employment among workers with longstanding illness was largest in Scandinavian countries.62 Alternative measures to express the influence of health problems on exit from paid employment are, for example, lost working years due to health problems or working life expectancy.63 ,64
Perceived health shows stronger associations than mental health and chronic diseases with regard to exit from paid employment. In the majority of the studies in this review, perceived health (19 out of 19), mental health problems (21 out of 23) and chronic diseases (14 out of 19) were self-reported. Thus, it is reasonable to assume that the differences in magnitude of the associations between health measures and exit from paid employment are not due to systematic differences in ascertainment of these health measures. Studies which have included a variety of different health measures in the same study population endorse this assumption. For example, Van den Berg et al demonstrated higher associations for self-perceived poor health with disability pension (OR 4.24), unemployment (OR 1.96) and early retirement (OR 1.32) compared with the associations found for chronic diseases with OR 2.62, OR 1.30 and OR 1.28, respectively.43 A study by Kuoppala et al showed that self-perceived poor health increased the risk of receiving a disability pension (OR 5.11, 95% CI 2.31 to 11.28). Whereas, in the same study, a lower association was found between poor mental well-being and disability pension (OR 2.77, 95% CI 1.32 to 5.80).26
The strong association between perceived health and exit from paid employment could be explained by the fact that self-perceived health partly reflects health-related quality of life, which is an integrated perception of health, including its biological, psychological and social dimensions.65 For example, important risk factors for poor health, like obesity and physical activity, are associated with exit from paid employment through disability benefit.15 In the majority of the studies perceived health was measured with a single question on a 4-point or a 5-point scale. This restriction could be seen as a disadvantage. However, the assessment of self-perceived health has been found to be useful in evaluating health status in large epidemiological studies and has been shown to be a strong predictor of mortality in high as well as low socioeconomic groups.66
The impact of self-perceived poor health, mental health problems and chronic diseases is higher for the involuntary pathways (disability pension, unemployment) than for a more voluntary pathway (early retirement). For example, Van den Berg et al demonstrated that self-perceived poor health was significantly associated with disability pension (OR 4.24, 95% CI 2.71 to 2.62) and unemployment (OR 1.96; 95% CI 1.32 to 2.92), but was borderline significant with early retirement (OR 1.32; 95% CI 1.01 to 1.32).43 A study by Kirchhoff et al36 showed that self-perceived poor health significantly increased the risk of receiving disability pension (RR 7.83; 95% CI 6.11 to 10.04). However, no association was found between poor health and exit from paid employment due to unemployment (RR 0.94; 95% CI 0.65 to 1.37).
The mean PAFs of self-perceived poor health, mental health problems and chronic diseases for transition into disability pension were 36.9%, 11.1% and 20.6%, respectively. The PAFs of chronic diseases ranged from 1.6% to 69.9% and, in general, larger PAF values were observed for studies with a higher prevalence of receiving disability pension.
The mean PAF of poor health for transition into unemployment varied between 4.0% for chronic diseases to 10.6% for mental health. For transition into early retirement, the mean PAF of self-perceived poor health and chronic diseases was 4.7% and 1.7%, respectively. These findings suggest that poor health is a major risk factor for exit from paid employment, especially through disability pension. Thus, policies to promote sustainability of paid employment should incorporate health promotion.
The observational studies in this systematic review suggest that interventions aimed at promoting good health in the workplace may have an important contribution to increase sustained employability. There are indications that workplace health promotion improves self-perceived health and worker productivity, and will also lead to a decline in sick days.67–69 Besides, unhealthy lifestyle behaviours, physical and psychosocial work demands as well as organisational level factors play a role in exit from paid employment.38 ,70–72 Therefore, it should be considered to integrate health promotion activities with activities aimed at occupational health and safety to maintain a productive workforce.
A strength of this systematic review is the availability of enough studies of good quality (large sample size, longitudinal design) on the association between health measures and disability pension, unemployment and early retirement to conduct informative meta-analyses to estimate the magnitude of these associations. However, this study also has some limitations. First, the literature search may not be comprehensive enough, because publications in languages other than English were not included, and the search was limited to two computer-based bibliographical databases. Therefore, it might be possible that some useful studies were missed. Second, there is substantial variation between studies according to definitions of outcome and risk factor, follow-up period, and sex and age of the study population. However, in an explorative meta-regression analysis no determinants of heterogeneity were found. Third, the majority of studies are from Scandinavian countries, hampering the generalisability of findings to other countries. Consequently, the influence of type of welfare regime on the relationship between poor health and different pathways of leaving the labour market cannot be determined. Fourth, the calculation of exit from paid employment attributable to poor health was based on the methodology of PAF.21 This method may yield biased estimates when used with RR estimates adjusted for confounding. When the crude RR is greater than the adjusted risk, as was observed in the current review, the PAF may be underestimated.73 Last, although publication bias cannot be ruled out, there was no relation between the magnitude of risk estimates and their CIs of self-perceived health and mental health and the risk of exit from paid employment due to disability benefit, unemployment and early retirement. For chronic diseases larger risk estimates had larger CIs concerning exit from paid employment due to disability benefit, but not for unemployment and early retirement. Therefore, results about the influence of chronic diseases on the risk of disability benefit should be interpreted with some caution.
After summarising the literature it can be concluded that self-perceived poor health is a risk factor for exit from paid employment due to disability pension, unemployment and early retirement. The proportions of persons leaving the labour market that could be attributed to self-perceived poor health were 36.9%, 7.0% and 4.7%, respectively for disability pension, unemployment and early retirement. Having mental health problems or a chronic disease was related with an increased risk of receiving disability pension or becoming unemployed, but not with early retirement. Primary preventive interventions focusing on promoting good health may contribute to sustained employability. Therefore, in order to maintain a productive workforce, it should be considered to integrate health promotion activities with activities aimed at occupational health and safety.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Files in this Data Supplement:
- Data supplement 1 - Online supplement
Footnotes
-
Correction notice This article has been corrected since it was published Online First. The relative risk values in the abstract have been updated.
-
Contributors RMvR: executed the systematic review, conducted the literature search, selected relevant articles for inclusion, performed the data extraction, analysed the data and wrote the manuscript. SJWR: helped conduct the literature search, selected relevant articles for inclusion and contributed to the content of the manuscript. SB and AB initiated the study and contributed to the content of the article. All four authors made a substantial contribution to the information and material submitted and have read and approved the final version.
-
Funding This work was supported by the Netherlands Organisation for Health Research and Development (ZonMW, grant 208030012).
-
Competing interests None.
-
Provenance and peer review Not commissioned; externally peer reviewed.