Article Text

Abstract
Objectives The aim was to investigate the variation in risk of breast cancer between occupational groups with a focus on white-collar and blue-collar workers and to investigate to what extent the differences were explained by risk factors related to reproduction and lifestyle.
Methods Between 1991 and 1996, 14 119 women born between 1923 and 1950 and residents of Malmö, Sweden, were included in this cohort study. Individual data on risk factors (eg, age, parity, age at first child, months of breast feeding per child, hormonal replacement therapy, physical activity, alcohol consumption, smoking, height and body mass index) and occupational history were assessed using a questionnaire. First-time diagnoses of invasive breast cancer were identified through the Swedish Cancer Registry up until 31 December 2013.
Results A total of 897 women were diagnosed with breast cancer. Analyses adjusted for age showed an increased risk for white-collar workers compared with blue-collar workers and indicated higher risks in the occupational categories: professionals, administrative and bookkeeping than among women in sales, transportation, production and service work. This difference was only marginally attenuated after adjustment for an extensive set of risk factors related to reproduction and lifestyle.
Conclusion Reproductive and lifestyle factors explain only a minor part of the increased risk of breast cancer in white-collar workers. Further studies are needed to investigate the remaining factors for the difference in risk between occupational groups.
- breast cancer
- occupation
- reproduction
- lifestyle
This is an Open Access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/
Statistics from Altmetric.com
What this paper adds
Previous studies show an increased risk of breast cancer in women in white-collar occupations and a reduced risk in manual and service occupations.
It has been assumed that differences in reproductive pattern and lifestyle habits may explain this contrast in risk.
After adjustments for individual data on an extensive set of risk factors related to reproduction and lifestyle, this contrast still persisted and was only marginally attenuated in this large prospective cohort study.
Further studies are needed to identify additional occupational risk factors for breast cancer in women.
Introduction
Breast cancer is the most common cancer in women and accounts for 12% of all cancers worldwide.1 With 522 000 deaths yearly, it is ranked as the leading cause of death from cancer in women.1 Many established risk factors for breast cancer in women are associated with hormonal factors related to reproduction.2 Hormonal risk factors include early menarche, late menopause, hormone replacement therapy (HRT) and oral contraceptive use, while protective factors are breast feeding, early first-time pregnancy and giving birth to many children.2 3 It has been hypothesised that the risk is proportional to the endogenous and exogenous exposures to oestrogen, although it is not known if this is the sole mechanism.2 The influence of reproductive risk factors, possibly mediated via oestrogen exposure, can partly be explained by the remodelling of the breast tissue that occurs during pregnancy and makes the breast more resistant to carcinogenic influence.4 Family history of breast cancer and especially carriers of breast cancer genes 1 and 2 (BRCA1 and BRCA2) is an important risk factor, and around 10% of all breast cancers are caused by genetic factors.5 Lifestyle factors such as alcohol consumption are strongly associated with an increased risk of breast cancer, and physical activity has shown a protective effect in some studies.6 7 High body mass index (BMI) is a risk factor for postmenopausal breast cancer which could potentially explain some of the protective effect from physical activity.2 Height is positively correlated to breast cancer risk, possibly through increased insulin growth hormone (IGF-1) in the body.8
Several studies have shown differences in breast cancer risk between occupational groups. Ramazzini 9 noted as early as 18th century that nuns seemed to be at an increased risk of breast cancer. Recent studies on occupation and cancer have found an increased risk in white-collar workers such as teachers, librarians and administrative workers, while the risk in blue-collar occupations such as manual and service occupations is usually somewhat lower than the national average.10–17 The Nordic Occupational Cancer study (NOCCA), which included 15 million people, showed a clear trend of higher risk of breast cancer in occupations with a higher socioeconomic position.18
It has been speculated that the increased risk among white-collar workers could be due to reproductive factors associated with a long education such as late first-time pregnancy, low parity and use of HRT.10 Unfortunately, many of the existing studies have not been able to fully adjust for these factors. The NOCCA study, Danø et al and the study by Pollán et al only adjusted for age,12 13 18 and the review by Goldberg et al was based on administrative data where other risk factors could not be taken into account.10 A few studies have been able to adjust for some of the important reproductive and lifestyle factors when investigating occupational differences. All of them found that the reproductive and lifestyle factors explained only a minor part or no part of the difference between occupational groups.11 14–17 19 However, one study only looked at premenopausal breast cancer,19 some studies did not adjust for alcohol consumption14–16 or physical activity,14–17 and two studies lacked data on breast feeding14 16 and HRT.14 17 In addition, several studies had a case–control design, which increased the risk of biases such as recall bias.10 11 14 15 17 There is a need for a prospective study that could investigate differences in breast cancer risk between occupations and also control for all known reproductive and lifestyle confounders.
The aim was to investigate the variation in risk of breast cancer between occupational groups with a focus on white-collar and blue-collar workers and to investigate to what extent the differences were explained by risk factors related to reproduction and lifestyle.
Methods
This study was based on the Malmö Diet and Cancer Study (MDCS), a prospective population-based cohort study described in detail elsewhere.20 Between 1991 and 1996, all women and men born between 1923 and 1950 and living in Malmö, Sweden, were invited to participate in the study. Active recruitment (personal letter invitation) and passive recruitment (posters and pamphlets in public areas, advertisements, etc) were used. Of 74 138 eligible persons, 24 851 did not respond or had an unknown address, 16 942 declined to participate and 4247 were excluded due to language problems. A total of 28 098 persons participated in MDCS, of which 17 035 were women. Those who were eligible for this study were women with no previous breast cancer (n=16 459). Women who had worked for less than 10 years were excluded from the study (n=2222), as were women who remained premenopausal until end of the follow-up period (n=118). Premenopausal women were excluded due to the low numbers of breast cancers among premenopausal women in the cohort. In addition, risk factor patterns differ for premenopausal and postmenopausal breast cancer.2 Menopausal status was assessed using both medical records and questionnaire data. A woman was considered postmenopausal if: (1) she had undergone bilateral oophorectomy, (2) she had undergone hysterectomy and was 55 years of age or older, (3) the above criteria were absent and she confirmed that her menstruation had ceased 2 years prior to baseline or (4) the above criteria were absent and she was 55 years of age or older. A total of 14 119 women were included in this study.
First-time diagnoses of invasive breast cancer between 1991 and 2013 were identified through the Swedish Cancer Registry. By law in Sweden, all malignant tumours must be reported, and the registry has a very high coverage for breast cancer of 99%.21 Breast cancer cases were identified as ICD7-code=170 (International Classification of Diseases, Seventh Revision), coded by the Swedish Cancer Registry. Death and migration status were retrieved from the Swedish National Tax Board.
Information on the three most recent occupations and specific work tasks were reported by the participants in the baseline questionnaire in free text and was later categorised into occupational codes according to FOB-80 (Population and Housing Census 1980) which is based on NYK, the Nordic version of the International Standard Classification of Occupations.22 In the present study we used the first three digits of FOB-80 including a total of 349 occupations. The FOB-80 classification scheme is organised so that main groups of occupations are ordered according to socioeconomic position, where low codes are associated with a high socioeconomic position. A participant was considered exposed based on any of her three most recent occupations.
Confounding risk factors accounted for were age (45–49, 50–54, 55–59, 60–64, 65–69, 70–74 years), parity (0, 1, 2, 3, ≥4), age at first child (<20, 20–24, 25–29, 30–34, 35+ years), months of breast feeding per child (0, 1–5, 6–12, ≥13), HRT (no treatment, oestrogen, progesterone, combined treatment), physical activity (percentiles), alcohol consumption (0, 1–14, 15–30, >30 g/day), height (<160, 160–169, ≥170 cm) and BMI (<18.5, 18.5–24.9, 25.0–29.9, ≥30).2 Confounding variables were selected based on a priori knowledge from literature and statistical analysis. Variables considered but not included in the final model were heredity, age at menarche, oral contraceptive use, education and smoking. Heredity was defined as a close relative with any form of cancer, which made the variable too general and not suitable for these analyses. Oral contraceptive use, education and smoking were run in a univariate and multivariate model with breast cancer as outcome (see online supplementary appendix 1). Since none of the variables were significant in the univariate model or had estimates which changed more than 10% in the multivariate analysis, they were rejected from the final model.
Most of the risk factors were self-reported through an extensive questionnaire answered at recruitment, while height and weight were measured by healthcare personnel. Months of breast feeding were reported for each child and a mean number was calculated. Imputations were made on breastfeeding data for women who had data for at least one child but no data for another. The mean number of months was used as imputation. Questions on alcohol consumption were asked with regard to the last 30 days using the validated questionnaire AUDIT.23 BMI was calculated as kg/m2 and categorisation was carried out according to the WHO standard.24 Physical activity was measured with several questions estimating the time of physical activity performed outside of work and multiplied by an intensity factor for each activity. The questionnaire measured the physical activity the year before baseline, taking seasonal changes into account.
Statistical analyses
χ2 tests were used to compare the distribution of risk factors for breast cancer among participants with breast cancer and in the total sample as well as between white-collar and blue-collar workers. The Cox proportional hazard model was used to estimate the HR for breast cancer in each individual occupation versus all other groups. Crude estimates were adjusted for age only, while the adjusted model also included parity, age at first child, months of breast feeding per child, HRT, physical activity, alcohol consumption, height and BMI. A log-likelihood test was performed to test the fit of the full model against the crude model. The cohort was open and women were considered to be under risk of breast cancer at baseline if postmenopausal. If premenopausal at baseline she was under risk at the time she became postmenopausal according to the above specified criteria for postmenopause. All women were followed up until a breast cancer incidence, death, migration or end of follow-up on 31 December 2013, whichever occurred first. Women who lacked any of the confounders were excluded from the adjusted analysis. Statistical analyses were performed with STATA version 13.0, and the α-level for significance tests was set at 0.05.
The MDCS main study was approved by Lund Ethical Review Board (LU 51–90). Ethical approval for the present study was obtained from the Stockholm Ethical Review Board (Ref. 2014/233-31/4).
Results
The cohort comprised 14 119 women, of which 897 were diagnosed with breast cancer during the study period. The age at baseline ranged from 45 to 74 years, with a mean age of 58.
Table 1 shows the distribution of risk factors in the total cohort, among breast cancer cases and among white-collar and blue-collar workers. Women with breast cancer had fewer children, received HRT to a higher extent, were less physically active, had a higher consumption of alcohol, were taller and had a higher BMI compared with all women in the cohort. Online supplementary appendix 1 shows that women with breast cancer received oral contraceptive to a higher extent and were higher educated compared with all women in the cohort. White-collar and blue-collar workers differed significantly in all aspects. White-collar workers had fewer children, were older at the time of having their first child, received HRT to a higher extent, were more physically active, had a higher consumption of alcohol and had a lower BMI compared with blue-collar workers.
Distribution of potential and established risk factors for breast cancer among cases and white-collar workers and blue-collar workers
The HRs for all occupational sectors (1-digit level), occupational groups (2-digit level) larger than 100 persons and occupational subgroups (3-digit level) larger than 100 persons that showed over or under risk are presented and visualised using colours in table 2. Light yellow represents a low HR, and dark red represents a high HR. In the unadjusted model, higher HRs were detected in occupational sectors with a higher socioeconomic position and were thus in the upper part of the table, while lower HRs were detected in the occupational sectors with a low socioeconomic position in the lower part of the table. It is evident that this trend is also consistent after adjusting for the risk factors related to reproduction and lifestyle. The model used for adjustments was tested with a log-likelihood test, which showed that the full model presented a significantly better fit than the crude model, χ2 (25)=136.7, p <0.001.
HR for invasive breast cancer for women who had ever worked for at least 10 years in an occupation
Differences in unadjusted HRs for breast cancer were detected between the main groups, white-collar workers (occupational sectors 0, 1, 2, 3) and blue-collar workers (occupational sectors 4, 5, 6, 7–8, 90–94, 98), where white-collar workers had a significantly elevated risk of breast cancer (HR=1.27, 95% CI=1.09 to 1.47) compared with blue-collar workers. Differences were also noted within occupational sectors and occupational groups. The occupational sectors 0–2, professionals, administrative and bookkeeping all presented elevated HRs, while sectors 3, 6, 7–8, 90–94 comprising sales, transportation, production and service showed lower HRs.
Adjustment for factors related to lifestyle and reproduction changed the risk estimates to some extent. After adjustment, white-collar workers were at a slightly lower HR (HR=1.25, 95% CI=1.06 to 1.47), although still at a significantly increased risk. The majority of the occupational sectors were attenuated towards a HR of 1, and none of the sectors had significantly elevated or decreased risk after adjustments. However, registered nurses (HR=1.48, 95% CI=1.07 to 2.05) and teachers of theoretical subjects (subjects that do not demand physical involvement, for example, natural and social sciences, languages and maths) (HR=1.57, 95% CI=1.06 to 2.32), which are subgroups of professionals, both had significantly elevated unadjusted risk estimates for breast cancer. Registered nurses remained at a significantly elevated risk after adjustments (HR=1.51, 95% CI=1.08 to 2.08), while teachers of theoretical subjects did not (HR=1.37, 95% CI=0.90 to 2.05).
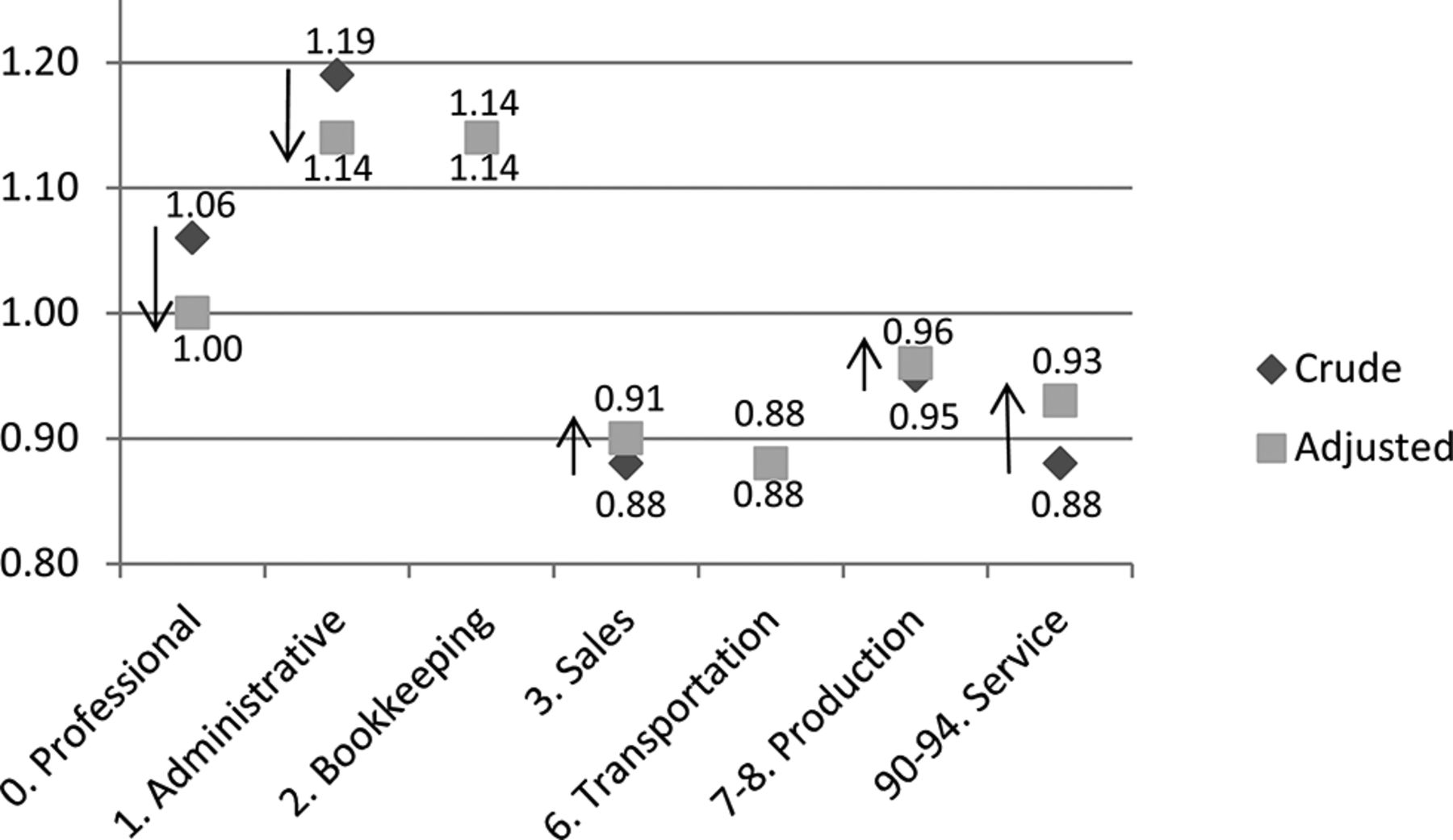
Figure 1 illustrates how much of breast cancer risk in different occupational sectors can be explained by risk factors related to reproduction and lifestyle. The figure includes occupational sectors with more than 100 women and more than 10 cases of breast cancer. The HRs for the professional and administrative occupational sectors diminished, while the HRs for sales, production and service occupations increased by adjusting for the set of confounding risk factors. All occupational sectors which were affected by the adjustment were adjusted towards a HR of 1.00.
{kind=link}
Change in HR for invasive breast cancer per main occupational sector by adjustment for risk factors related to reproduction and lifestyle.
DISCUSSION
This study indicated that the risk of breast cancer differed between occupational sectors in a way that was consistent with the earlier observations of higher risk among women in white-collar occupations such as professional and administrative occupations, and lower risk among women in blue-collar occupations such as manual and service occupations. This difference in risk was only partially attenuated when adjusting for risk factors related to reproduction and lifestyle. The results confirmed previous studies showing that reproductive and lifestyle factors do not explain the difference in breast cancer risk between occupational groups.11 14–17 19
The gradient of high risk of breast cancer in occupational sectors with a high socioeconomic position (white collar) and low risk in low socioeconomic occupations (blue collar) has been reported in several previous studies.10–18 Even if some of the excess risk is due to reproductive and lifestyle factors as the adjustments show, many studies, like ours, still detect a high risk for this group even after adjustments. A potential alternative explanation has been put forward by Pudrovska et al who discussed the life-course stress approach, where occupations with a high socioeconomic position have a higher level of job authority and are therefore more stressful.16 This stress could cause chronically elevated cortisol levels, increasing the risk of breast cancer, and might therefore be one of the remaining explanations for the increased risk seen in this group.16 Another possible explanation for the increased risk among women with a high socioeconomic position is the increased participation in mammography screening and therefore increased detection of breast cancer in this group.25 A third possible explanation might be the difference in physical activity at work between white-collar and blue-collar workers. However, very little is known about physical activity at work and breast cancer risk.
Registered nurses presented elevated HRs in unadjusted as well as adjusted analysis. These results indicate that the increased risk in registered nurses as a group was not due to reproductive or lifestyle factors and contradicts the ‘long education’ hypothesis. Several previous studies have also shown an excess risk for nurses.11 15 Nurses are exposed to various potential carcinogens such as ionising radiation, chemotherapeutic agents and ethylene oxide which could possibly explain the excess risk. Most nurses also work night shifts, which disrupt the hormone levels in the body and could potentially increase the risk of breast cancer.26 27 A study of Icelandic nurses showed the highest risk for nurses handling cytotoxic drugs and among paediatric nurses, while nurses in primary healthcare had a significant lower risk of breast cancer.28 A possible explanation is that a combination of these occupation-specific exposures that nurses are exposed to is contributing to their elevated risk of breast cancer.
Teachers of theoretical subjects had a significant excess risk of breast cancer in the unadjusted analysis. However, when adjusting for the risk factors related to reproduction and lifestyle, the risk dropped slightly and was no longer statistically significantly elevated. This indicated that teachers’ increased breast cancer risks are probably due to reproductive and lifestyle factors. Previous studies have also found an increased risk for teachers, although they have had difficulties explaining the mechanism.12 29 30 High socioeconomic status has been part of the explanation, together with speculation that the sedentary work situation of teachers could increase the risk of breast cancer.12
This study has some weaknesses and strengths that need to be considered. Even though we had access to extensive individual data, data on night work was not available. Night work is a possible risk factor for breast cancer, and many nurses frequently work at night.26 Night work may contribute to the elevated risk among nurses after adjustment for lifestyle and reproductive factors, but there is no explanation for the general trend of higher risk in occupations associated with higher socioeconomic position, noted in both this and other studies.
This study had a participation rate of 39%. According to a dropout analysis, non-participants had higher mortality and overall poorer health than the participants, although the socio-demographic structure was equal in the groups.20 A selection of a somewhat healthier cohort could affect the external generalisability regarding the distribution of risk factors in the population, but does not affect the generalisability of findings regarding risks and effects of adjustment to the same extent. This is a prospective study where all exposures were registered before the outcome was known, thus eliminating the possibility that the outcome could have influenced participation. The exposures are measured at baseline and therefore do not vary with time, which increases the risk of misclassification of exposure. However, since the potential misclassification is non-differential, it will generally lead to an attenuation of the risk ratios. In addition, since the participants were 45 years or older at inclusion, most reproductive data did not change over time for the participants. A potential weakness is the possibility of detection bias. Women with a higher socioeconomic status are known to attend mammography screening more often than women with a low socioeconomic status, and therefore smaller and additional tumours would be detected among these women.25 However, in the confounding model (see online supplementary appendix 1) it is clear that adjusting for education, which is a strong predictor for socioeconomic status, did not affect the breast cancer risk, and the increased risk in the professionals and administrative categories is therefore not likely to be due to detection bias. The strengths of this study include the extensive individual data and the coverage of the Swedish Cancer Registry, which is close to 100%. Another strength is the study design, using a prospective cohort with a follow-up of more than 20 years allowing for cancer outcomes to be studied.
A trend of high risk of breast cancer for women in white-collar occupations and low risk for women in blue-collar occupations was noted. These differences were attenuated after adjusting for risk factors related to reproduction and lifestyle, although a considerable difference in risk still remained, indicating that there may be other factors not yet accounted for.
Conclusion
There was a difference in breast cancer risk between occupational groups. White-collar workers like professionals, administrators and bookkeepers showed a tendency for a high risk of breast cancer, and blue-collar workers in sales, production, transportation and service workers showed a tendency for a low risk. After adjustment for individual data on an extensive set of risk factors related to reproduction and lifestyle, this contrast still persisted and was only marginally attenuated. Thus, differences in reproductive pattern and lifestyle habits seem to explain only a minor part of the difference in risk between occupational groups and between white-collar and blue-collar workers. Further studies to determine occupational risk factors for breast cancer are needed.
References
Footnotes
Acknowledgements The authors thank Håkan Andersson, IT coordinator at Skåne University Hospital, for data management. We also thank the occupational hygienists Pernilla Wiebert and Nils Plato for valuable input on the study design.
Contributors All authors participated in the conception and study design. CK, JS, JM, SB and PG took part in data collection. CK performed the analysis and CK, JS and PG prepared the first draft of the paper, while all authors took part in the discussion, interpretation and revision of the manuscript. All authors have read and approved the final version of the manuscript.
Funding Financial support was given by the Swedish Research Council for Health, Working Life and Welfare (FORTE).
Competing interests None declared.
Ethics approval Stockholm Ethical Review Board (Ref. 2014/233-31/4).
Provenance and peer review Not commissioned; externally peer reviewed.