Article Text

Abstract
Objectives The risk of suicide among UK military veterans remains unclear. Few recent studies have been undertaken, and most studies found no clear evidence of increased risk. We used data from the Trends in Scottish Veterans Health cohort to investigate suicides up to 2017 in order to examine whether there have been any changes in the long-term pattern of veteran suicides since our earlier study to 2012, and to compare trends in the risk of suicide among veterans with matched non-veterans.
Method Retrospective cohort study of 78 000 veterans and 253 000 non-veterans born between 1945 and 1995, matched for age, sex and area of residence, using survival analysis to examine the risk of suicide in veterans in comparison with non-veterans overall and by subgroup, and to investigate associations with specific mental health conditions.
Results Up to 37 years of follow-up, 388 (0.5%) veterans and 1531 (0.6%) non-veterans died from suicide. The risk of suicide among veterans did not differ from non-veterans overall. Increased risk among early service leavers was explained by differences in deprivation, and the previously reported increased risk in female veterans is now confined to older women. Suicide was most common in the fifth decade of life, and around 20 years postservice. A history of mood disorder or post-traumatic stress disorder was non-significantly more common in veterans.
Conclusions Veterans are not at increased risk of suicide overall. The highest risk for both men and women is in middle age, many years after leaving service.
- women
- military personnel
- veterans
- retrospective studies
- epidemiology
Data availability statement
No data are available. The study remains in progress and the data are not currently available for sharing.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
Key messages
What is already known about this subject?
There is no consensus as to whether military service increases the risk of suicide, although the majority of studies support the view that there is no clear evidence of increased risk.
What are the new findings?
This new study confirms that there is no overall increase in risk compared with the wider population, although older women veterans remain at increased risk. The interval between leaving service and suicide was around 20 years. The previously reported increase in early service leavers is explained by differences in socioeconomic status.
How might this impact on policy or clinical practice in the foreseeable future?
Strategies aimed at prevention of suicide in veterans should concentrate on support for middle-aged veterans, particularly those with known mental health problems, rather than those who have recently left service.
Introduction
Of all the health outcomes putatively associated with veteran status, none is more distressing than suicide. Despite extensive research, there remains no consensus as to whether military service, encompassing operational deployment or not, increases the risk of suicide, although the majority of studies support the view that there is no clear evidence of increased risk.1 2 We have previously published the findings of a 31-year retrospective cohort study examining the risk of suicide in a cohort of 57 000 veterans in Scotland between 1981 and 2012, in comparison with 173 000 non-veterans matched for age, sex and area of residence, and found no statistically significant difference between veterans and non-veterans overall, although there was a significantly higher risk in female veterans in comparison with non-veteran women.3 There have been few more recently published studies on the epidemiology of suicide in veterans, an exception being a Swedish study which reported similar risk in deployed and non-deployed veterans.4 The majority of other recent studies have focused on identification of risk factors for suicide, generally with the aim of developing or targeting preventive strategies.5 Nonetheless, monitoring the epidemiology of suicide remains important, in light of the potential impact of these strategies or changes in underlying risk factors.
Our original cohort, which provided data on veterans to the end of 2012, has now been refreshed to provide an additional ten year birth cohort, and updated outcome data to the end of 2017, equating to a further 22 000 veterans and 80 000 non-veterans and an additional 5 years of follow-up of the original subjects. This has enabled us to examine whether there have been any changes over time, and also to look at longer-term trends in the risk of suicide in veterans in comparison with matched non-veterans.
Methods
We examined data from the Trends in Scottish Veterans’ Health study, a retrospective cohort study of 78 385 military veterans resident in Scotland who met the eligibility criteria, and a comparison group of 252 637 individuals with no record of service matched 3:1 for age, sex and postcode sector of residence (mean population 5000).6 The method of selection of the study cohort and the comparison group has been fully described elsewhere.6 Veterans were eligible for inclusion if they were born between 1 January 1945 and 31 December 1995 and were registered with National Health Service (NHS) Scotland both before and after service. The study builds on the Scottish Veterans Health Study, using similar methodology which is described elsewhere.7 Demographic data obtained from electronic NHS registration records were linked at an individual level to death certificates to provide information on deaths by cause, and to routine hospital admissions data (Scottish Morbidity Record, SMR01) and psychiatric inpatient records (SMR04) for information on any antecedent mental health diagnoses, and on specific physical diagnoses reported to be associated with increased suicide risk. Dates of entering and leaving the Service, for veterans, were obtained from the Scottish NHS registration record. The maximum period of follow-up was 37 years, from 1 January 1981 (or date of leaving the Armed Forces, for veterans, if later) to 31 December 2017.8 9 As this study was a secondary data study, individual consent was not required.
Socioeconomic status
A measure of area-based socioeconomic status (SES) is provided by the Scottish Index of Multiple Deprivation (SIMD), which is based on 6505 datazones, derived from postcode of residence, with a mean population of 800. SIMD is calculated from information on income, employment, health, education (including skills and training), housing, crime and access to services. The SIMD was used to derive quintiles of SES for the Scottish population; ranging from 1 (most deprived) to 5 (least deprived).10 The cohort participants were categorised according to these quintiles using their postcode of residence.
Statistical methods
‘Suicide and fatal self-harm’ was defined as cause of death recorded as ICD10 codes X60–X84, Y87.0, Y10–Y34 or Y87.2 or ICD9 codes (used in Scotland prior to 1 January 1997) E950–E959 or E980–E989 at any position on the death certificate, in line with national coding guidelines.11 These codes encompassed death resulting from suicide, intentional self-harm or events of undetermined intent. For conciseness the term ‘suicide’ is used in this paper to encompass all such events whether legally determined to be suicide or not. We categorised the method of suicide as ‘non-violent’ if resulting from poisoning by solids, liquids or gases (ICD-10 X60-X69, Y10–Y19 or ICD-9 E950–E952), and ‘violent’ if due to hanging, strangulation, suffocation, drowning, falling or jumping from a height, firearms or explosives, cutting, or contact with a moving object (ICD-10 X70-X82, Y20–Y32 or ICD-9 E953–E957). Antecedent mental health diagnoses were defined as anxiety disorders including post-traumatic stress disorder (PTSD) (ICD-10 F40–F48 and ICD-9 300 and 308–309), mood disorders (ICD-10 F30–F39 and ICD-9 296) and psychosis (ICD-10 F20–F29 and ICD-9 295, 297 and 298). Physical diagnoses explored were cardiovascular disease (defined as acute myocardial infarction ICD-10 I21 or ICD-9 410, stroke ICD-10 I60–I64 or ICD-9 430–432, 436 and 436, or peripheral arterial disease ICD-10 I702 or I73–79, or ICD-9 443.9 or 440.2), cancer (ICD-10 C00-C97 and D00-D09 (less D069), ICD-9 140–209 and 230–234) and diabetes (ICD-10 E10–E14 or ICD-9 250, or an entry in the Scottish Diabetes Register).12–14 ‘Early Service Leavers’ (ESL) were defined as veterans who had left with 3 years’ service or less. Although shorter than the current 4-year minimum, this ensured correct classification of older veterans who had completed the pre-1999 minimum of 3 years’ service.15 Junior entrants were defined as personnel who entered service under 17.5 years of age, in a predominantly educational role.16 Cox proportional hazard models were used to examine the association between veteran status and cumulative risk of suicide, using age as the time-dependent variable, age at death from suicide as the failure time, and age at death (from causes other than suicide) as the censor time.17 Proportionality assumptions were tested using methodology based on Schoenfeld residuals.18 The log-likelihood test was used to test for interactions between veteran status, risk of suicide, and both sex and birth cohort separately. The a priori rejection level was set at 0.05. The models were run univariably and then repeated adjusting for the potential confounding effect of SES. The analyses were repeated stratifying by 5-year bands of birth year to examine potential birth cohort effects, and by length of service. Incidence was calculated as suicides per 100 000 person-years, based on time of follow-up from entry to the study, to death or censoring. Method of suicide was compared for veterans and non-veterans, by gender. Associations with specific antecedent diagnoses were explored using ORs. A sensitivity analysis was performed, examining HRs at notional earlier end points, in order to assess trends. All analyses were performed using Stata V.16.
Results
After data cleansing to remove incomplete or invalid records, 78 157 (99.7%) veterans and 252 637 (100%) non-veterans were included in the analyses. There were 70 581 (90.3%) male veterans and 7573 (9.7%) female, reflecting the gender balance of the UK Armed Forces. The mean period of follow-up was 32.5 years, and there was a total of 10.6 million person-years of follow-up among veterans and non-veterans combined.
Over the period of follow-up, there were 388 (0.5%) suicides among veterans (6.6% of all veteran deaths), and 1531 (0.6%) suicides in non-veterans (7.8% of all non-veteran deaths). This equated to a crude incidence of 22 per 100 000 person-years in veterans compared with 17 per 100 000 person-years in non-veterans, but direct comparison is misleading because of generally shorter follow-up in the veterans. Cox proportional hazard analysis, taking account of length of follow-up, demonstrated that there was no difference in risk of suicide overall between veterans and non-veterans, HR 1.01, 95% CIs 0.90 to 1.13, p=0.859 (figure 1). Testing for non-proportionality of the hazards was non-significant, p=0.330. The median elapsed time from leaving the Armed Forces to suicide was 18.9 years, IQR 9.7–25.2 years.
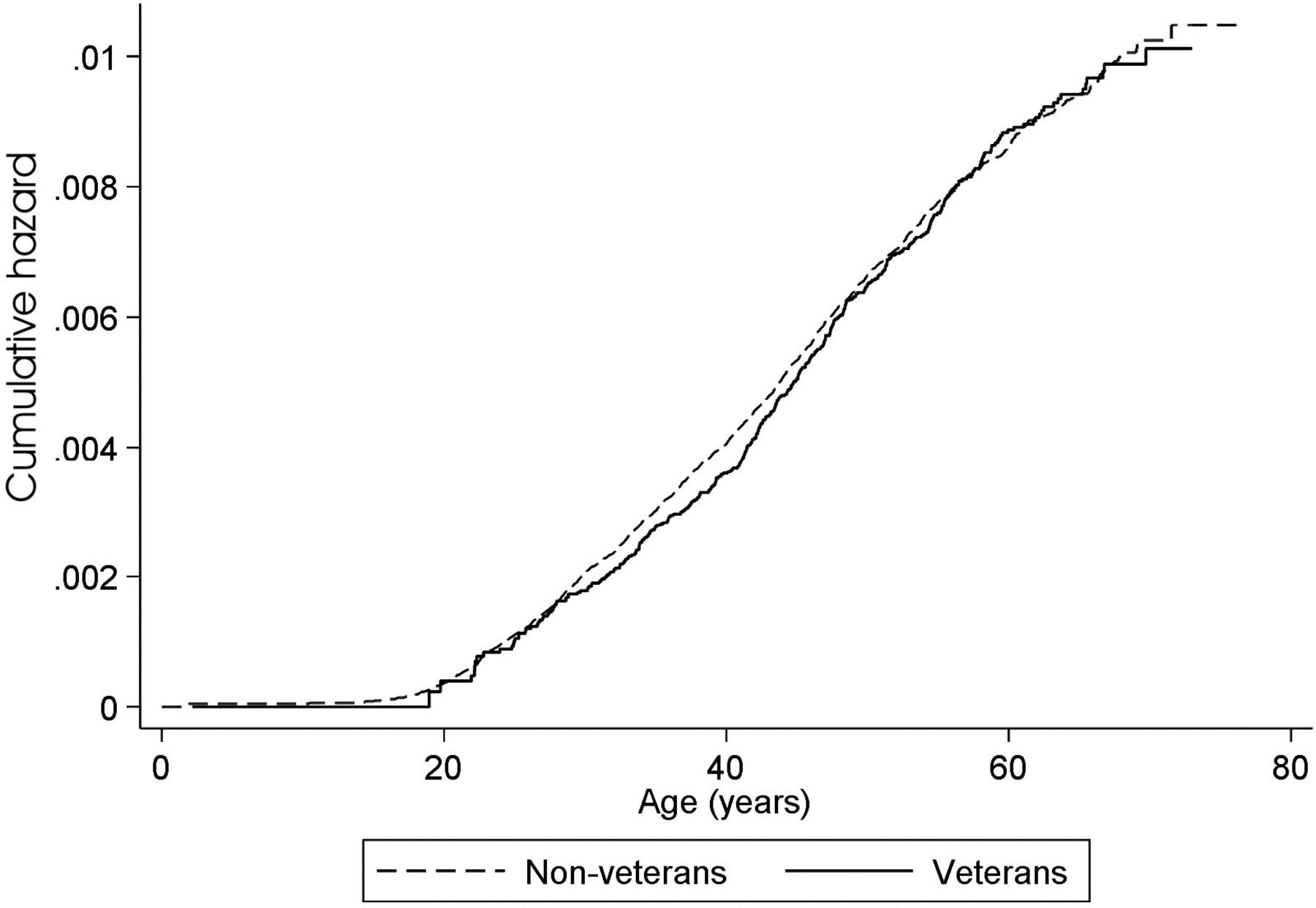
Nelson-Aalen plot of risk of suicide, veterans compared with non-veterans.
Sex, age and birth cohort effects
When stratified by sex, there was no difference in overall risk for male veterans in comparison with male non-veterans, HR 0.98, 95% CI 0.87 to 1.10, p=0.751, but there was an increase in overall risk for female veterans, HR 1.57, 95% CI 0.91 to 2.69, p=0.103, although this did not reach statistical significance. A landmark analysis from age 40 years demonstrated that older women veterans were at significantly increased risk, HR 2.65, 95% CI 1.41 to 4.99, p=0.003, whereas the risk in older male veterans reflected that in the wider community, HR 1.04, 95% CI 0.90 to 1.21, p=0.571. Non-veteran women were at greatly reduced risk of suicide compared with non-veteran men, HR 0.28, 95% CI 0.21 to 0.37, p<0.001; the difference between female and male veterans, HR 0.47, 95% CI 0.30 to 0.76, p=0.002, was less than in non-veterans.
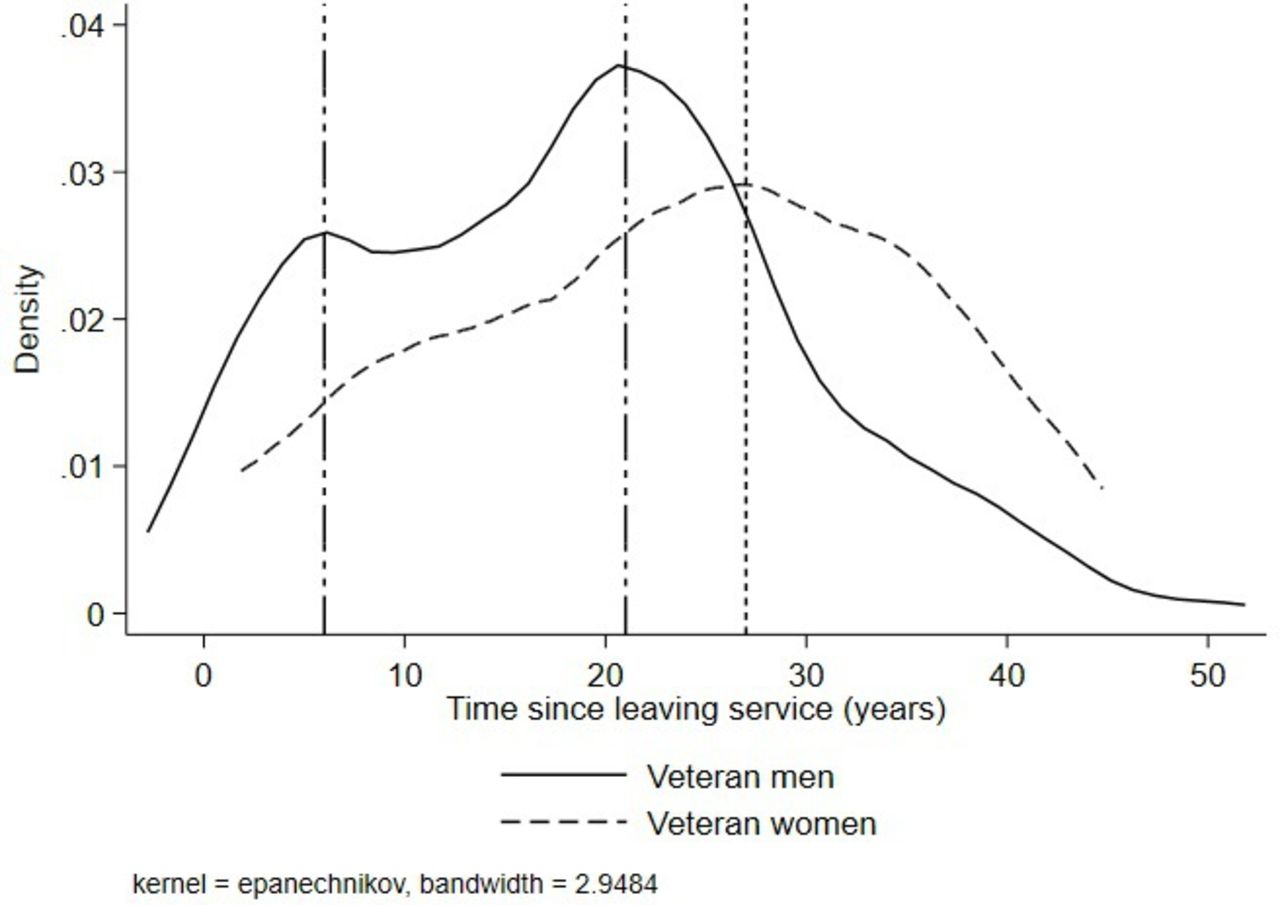
Veterans were generally older than non-veterans at the time of suicide (figure 2). The median age at suicide for veterans overall was 43.6 years (IQR 36.5–50.4) whereas for non-veterans it was 39.1 years (IQR 30.6–47.3). The difference was especially marked for women, with a median age of 50.0 years (IQR 42.6–55.2) for veteran women compared with 37.5 years (IQR 31.5–47.0) for non-veteran women. The elapsed time from leaving service to suicide was longer for women than men (median 25.9 years (IQR 15.4–32.1) for women, compared with 18.6 years (IQR 9.5–24.7) for men) (figure 3). The kernel density plot also shows a small peak for men around 6 years after leaving service although the absolute number of cases was low.
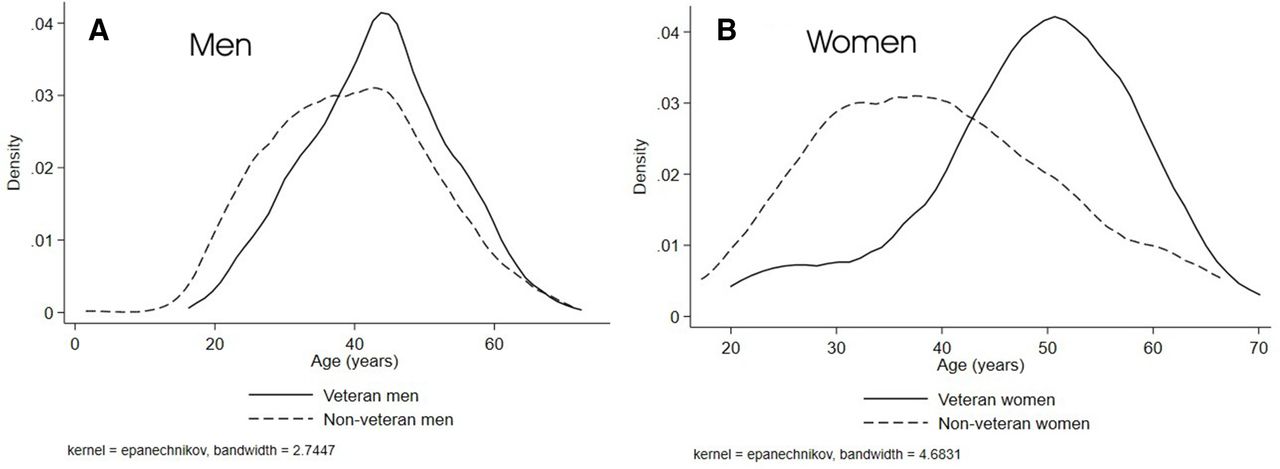
Kernel density plot of age at suicide, veterans and non-veterans. (A) men (B) women.
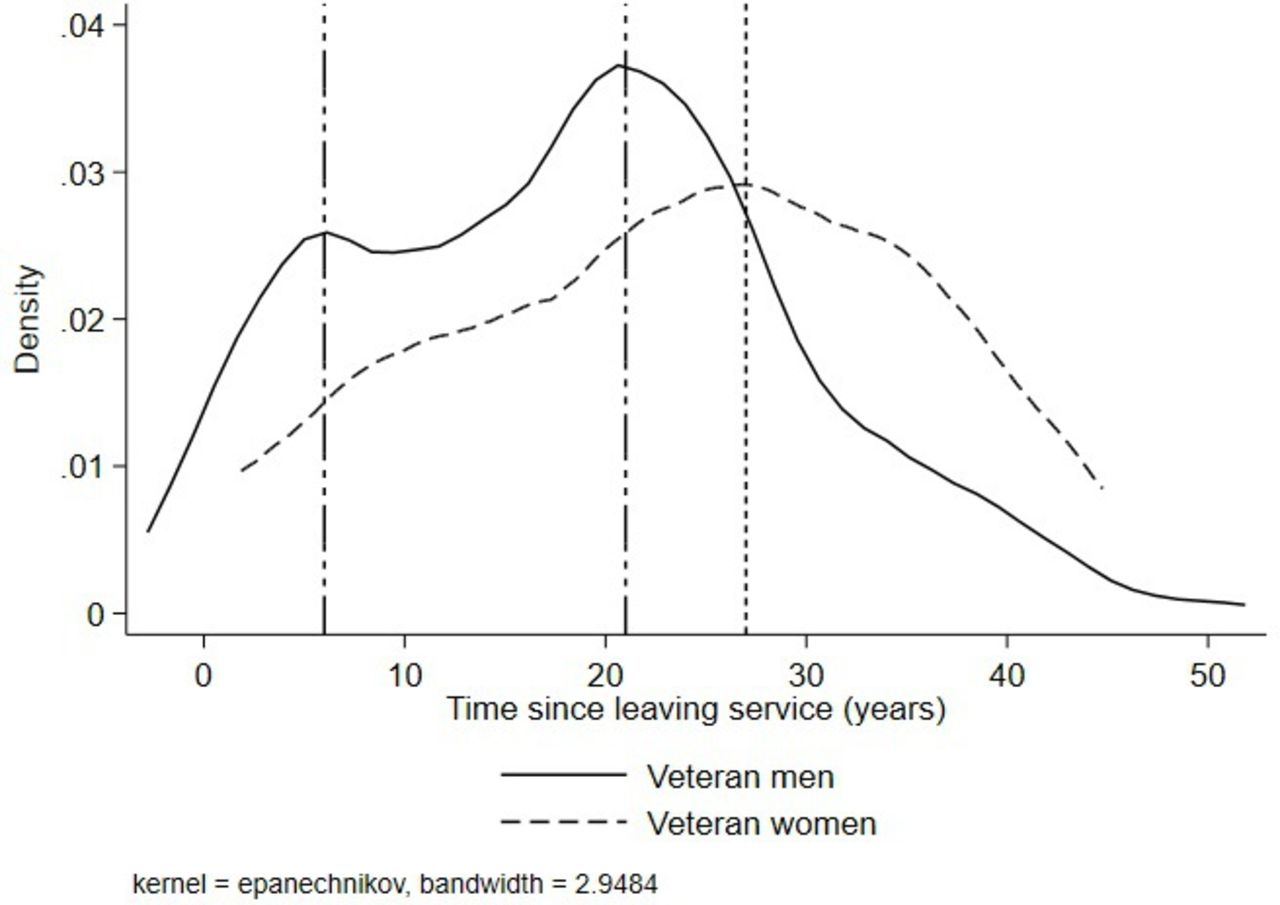
Kernel density plot of time since leaving service at suicide, male and female veterans. Reference lines at 6, 21 and 27 years.
Analysis by birth cohort demonstrated a statistically significant increased risk only in the 1950–1954 cohort. There was evidence of a non-significant increase in the most recent (1985–1995) birth cohort, but the absolute numbers were small and the confidence intervals very wide (figure 4). The majority of male veterans (86%) who died as a result of suicide were born before 1973; for women veterans, all were born before 1972, and none were recruited after 1990.

HRs for suicide by birth cohort, veterans compared with non-veterans. Error bars represent 95% CIs.
Length of service, junior entrants and young veterans
When stratified by length of service, two subgroups were at increased risk, ESL and veterans with 17–22 years’ service, although the latter was not statistically significant. The median age at suicide was 2.5 years earlier for ESL than for non-ESL, median age 42.2 years (IQR 33.8–48.5) for ESL veterans compared with 44.7 years (IQR 37.9–51.4) for all non-ESL. When ESL were compared with all non-veterans, there was a statistically significant increase in risk of suicide, HR 1.25, 95% CI 1.05 to 1.48. p=0.010, but the risk was attenuated and became non-significant after adjusting for SES, HR 1.14, 95% CI 0.96 to 1.35, p=0.138. The increased risk was only significant for ESL born prior to 1960; it became non-significant in later birth cohorts. Service personnel who completed at least the minimum engagement were at similar risk to non-veterans, univariable HR 0.91, 95% CI 0.79 to 1.04, p=0.161, which was unchanged after adjusting for SES. The median elapsed time from leaving the Armed Forces to suicide was 22.4 years (IQR 14.6–29.1) for ESL and 16.6 years (IQR 7.6–22.9) for veterans who completed at least the minimum term.
The HR for veterans with 17–22 years’ service was 1.29, 95% CI 0.86 to 1.91, p=0.218; by contrast, veterans with more than 22 years’ service were at non-significantly reduced risk, HR 0.57, 95% CI 0.30 to 1.06, p=0.076. The risk in the 17–22 years subgroup was increased after adjusting for SES, HR 1.37, 95% CI 0.92 to 2.05, p=0.120 although it remained non-significant.
Junior entrants were not at increased risk compared with non-veterans, HR 0.97, 95% CI 0.82 to 1.15, p=0.739. When compared with adult entrants, their risk of suicide was similar, HR 0.93, 95% CI 0.75 to 1.13, p=0.455.
No suicides have occurred in veterans in Scotland aged under 20 years since 2001, and none aged under 18 years since 1992. There were 13 deaths from suicide in veterans aged under 25 years over the period of follow-up (26.5% of all veteran deaths in this age group), compared with 170 (25.0%) non-veterans, a non-significant difference, OR 1.06, 95% CI 0.65 to 1.72, p=0.811.
Method of suicide
Among male veterans, 66.5% of suicides were classified as due to violent means, compared with 63.4% in male non-veterans, OR 1.06, 95% CI 0.98 to 1.15, p=0.165. Among women, 36.5% of veteran suicides were by violent means, compared with 40.8% in non-veteran women, OR 0.87, 95% CI 0.45 to 1.70, p=0.678.
Antecedent conditions
A history of mood disorder sufficient to require hospitalisation was recorded in 18.3% of veterans who died from suicide and 16.6% of non-veterans. The difference was not statistically significant, OR 1.10, 95% CI 0.87 to 1.40, p=0.423. PTSD was much less common, being recorded in 6.2% of veterans who died from suicide and 4.9% of non-veterans. The increase in risk of suicide in veterans with PTSD, compared with non-veterans, did not reach statistical significance, OR 1.26, 95% CI 0.81 to 1.97, p=0.306. Examining a range of physical antecedent conditions, there was no difference in risk between veterans and non-veterans for type 2 diabetes, OR 1.01, 95% CI 0.55 to 1.83, p=0.984, or cancer, OR 1.15, 95% CI 0.61 to 2.04, p=0.724. There was an increased risk of a history of cardiovascular disease although it did not reach statistical significance, OR 1.57, 95% CI 0.82 to 3.05, p=0.173, and veterans who died from suicide were at non-significantly lower risk than non-veterans of having a recorded diagnosis of alcoholic liver disease, OR 0.79, 95% CI 0.30 to 2.05, p=0.625.
Trends in suicide risk
We performed a sensitivity analysis to examine notional changes in the risk of suicide in veterans compared with non-veterans if the data had been examined at earlier points in time (figure 5). This demonstrated an increased risk in the 1990s, falling steadily over the following decade to achieve parity of risk between veterans and non-veterans by 2010.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Notional risk of suicide among veterans compared with non-veterans at earlier dates. Error bars represent 95% CIs.
Discussion
In this new study of a large national cohort of veterans followed up for up to 37 years, we confirm our earlier findings,3 which were based on a smaller veteran cohort and shorter follow-up, that veterans are at no overall increased risk of suicide. There was an increased risk in ESL which was explained by differences in deprivation, and the previous finding of an increased risk in female veterans is now confined to older women. Most veteran suicides occurred many years after leaving service, longer in women than men, consistent with the findings of a recent Canadian study.19 The pattern of methods of suicide in veterans reflects that in the wider community.
Our sensitivity analysis, examining the data at notional earlier end-points, indicates that concerns about an increased risk of suicide in young serving personnel in the 1990s and early 2000s20 21 may have pulled through into a real increased risk in young veterans at the same period.2 However, this excess risk has now disappeared. The reasons for this are likely to be multi-factorial. Whilst the Government’s 2010 report by Murrison22 made a clear commitment to improving mental health services for serving personnel and veterans, it is evident that the excess risk was already reducing by then. There had also been major changes to the provision of in-service support, with the establishment of a fully-integrated Defence Mental Health Service in 2004.23 Our finding of few suicides among young veterans in recent years suggests that improved in-service mental health advice and support may have been effective in reducing risk in this vulnerable group, although less so in ESL who by definition have a shorter period in service in which to benefit from it.
Our finding of evidence of an increased risk in veterans who left service at the 17–22 year point, who would generally have been senior Army non-commissioned officers and warrant officers, merits further study. There was no positive association with deprivation in this group and indeed the reverse may have been true. Those who served beyond 22 years are likely to have been commissioned officers in all three Services, or to have been senior non-commissioned officers in the Royal Navy or Royal Air Force who can serve to age 55 years. It is plausible that discharge at around age 40 years, as is the case for those serving a 22-year engagement in the Army, both coincides with a known period of vulnerability in early middle age,24 and renders it difficult to find worthwhile new employment. By contrast, those who retire and become veterans at age 55 years are largely past the high-risk age-group and, being older and in receipt of a full occupational pension, are less likely to have an expectation of moving to new full-time employment. Thus there may be grounds to re-examine the Army policy of the 22-year engagement in order to bring it into line with the engagement policies of the Royal Navy and Royal Air Force. Nonetheless it should be noted that in-service suicide rates were also high in men in the over 45-year age group, mirroring the pattern seen in civilians.21
In a study which profiled a treatment-seeking group of UK veterans, of whom over 80% reported PTSD symptoms and over 70% had common mental disorders, among those who responded to a questionnaire 68.2% were aged over 45 years, 39.2% were not in a relationship and 68.1% were not working. Nearly 60% had left service at least 15 years earlier. The majority had been in a combat role, mostly in Northern Ireland.25 We, therefore, suggest that although the popular image of mental health issues in veterans is dominated by young Iraq and Afghanistan veterans, there is an important hidden burden in older veterans who may have served elsewhere. This is supported by our finding that the median elapsed time between leaving service and completed suicide is around 20 years. The persistence of the increased risk of suicide in the 1950–1954 birth cohort which we first reported in our study to 20123 is consistent with service in Northern Ireland as a young soldier at the start of Operation BANNER in 1969, although a more detailed study of individual cases would be needed to confirm an association.
Developing predictive models for suicide which can accurately identify those at highest risk, and thereby maximise the benefit of targeting preventive interventions, presents major challenges. Large-scale studies by the US Veterans Health Administration have shown that these models fail to identify the majority of those who go on to die as a result of suicide; the best-performing, which used a Bayesian additive regression tree based on 61 predictive variables, predicted only 10.7% of the suicides which occurred in the veterans with the highest 1% of predicted risk scores. Furthermore, the model was most effective at identifying risk of suicide in the following 6 months; longer-term risk was much less likely to be detected by the model.26 27
Our finding that the risk of suicide in veterans is highest in the fifth decade of life, and that an average of 20 years elapsed between leaving service and suicide, suggests that interventions to identify suicide risk at the time of leaving service may not be effective. It also further emphasises that it is the middle-aged veterans whose need for support is greatest. However, this may not be a veteran-specific issue; it mirrors findings among middle-aged men in the wider community,1 as illustrated by our finding of no overall difference in risk between veterans and non-veterans. What may differ is the precipitating cause and therefore the approach needed to mitigate the risk. While issues such as unemployment and relationship breakdown are common to both veterans and non-veterans, a background of memories of combat-related incidents and perhaps moral injury are likely to require specialist veteran services.28 29 With the veterans of the early phases of the Iraq and Afghanistan conflicts now approaching middle age, suicide risk in these veterans should continue to be monitored for evidence of changing trends.
The major strength of this study is that it was based on a large cohort covering the whole of Scotland with up to 37 years follow-up. The International Classification of Diseases (ICD)-coded causes of death were taken from national vital records and acute and psychiatric hospital records, which are subject to regular quality assurance checks, and are therefore likely to be both accurate and complete in respect of those events occurring within Scotland.
Limitations of the study include possible lost to follow-up of subjects due to migration away from Scotland, which could not be quantified, and the lack of any follow-up data prior to 1981. As suicide is a comparatively rare outcome, the statistical power of the study was limited, even in this large cohort, and as a result, some of our findings did not achieve statistical significance. We have not considered it appropriate to dismiss these on that basis alone, especially where trend or other data supports the validity of the finding.30 We had no information on antecedent conditions managed solely as an outpatient or in primary care, however, we have made the assumption that the relative magnitude of hospital admissions reflects the relative magnitude of total cases. We had no information on the service to which a veteran had belonged (Army, Royal Navy or Royal Air Force), rank, deployment, combat exposure, lifestyle factors or adverse childhood events, so residual confounding may have been present. Veterans with reserve service only could not be identified and were included among the non-veterans; this may have reduced any observed differences between veterans and non-veterans although the number of suicides in reservists is likely to be insufficient to have had a major impact on our findings.
Data availability statement
No data are available. The study remains in progress and the data are not currently available for sharing.
Ethics statements
Patient consent for publication
Ethics approval
The data extract was pseudoanonymised and approval for the study was granted by the Public Benefit and Privacy Panel of the Information Services Division of NHS Scotland, approval number 1718-0133.
Acknowledgments
We thank the staff of the NHS Central Registry for extracting the dataset, the eDRIS Team (Public Health Scotland) for their involvement in obtaining approvals, provisioning and linking data and the use of the secure analytical platform within the National Safe Haven.
References
Footnotes
Contributors BPB conceived the idea and designed the study, with advice from JPP and DFM. BPB carried out the data analysis, which was overseen by DFM, and interpreted the findings. BPB wrote the first draft of the report, which was critically reviewed and edited by all authors. BPB revised the draft following peer review, and all authors approved the final article.
Funding ‘Trends in Scottish Veterans Health’ is funded by a grant from the Forces in Mind Trust, grant no. FiMT17/1101UG.
Disclaimer The views and opinions expressed are those of the authors and do not necessarily reflect those of the funders. The funding body had no role in the study design, analysis, interpretation of data or in writing the manuscript.
Competing interests BPB is a military veteran and Honorary Civilian Consultant Advisor (Army) in Veterans’ Health and Epidemiology. Neither the Army nor the Ministry of Defence had any input to this paper, and the views and opinions expressed are solely those of the authors. No other authors declare any interests.
Provenance and peer review Not commissioned; externally peer reviewed.
Linked Articles
- Commentary