Article Text

Abstract
Objectives Mesothelioma is a rare, aggressive cancer caused by exposure to asbestos fibres. Mesothelioma patients who receive trimodal therapy (chemotherapy, surgical resection and radiation) survive longer than those who receive two or fewer therapy modalities. This study analyses the 2016–2019 Medicare claims data to estimate the burden of malignant mesothelioma and describe therapy patterns (when available) among continuously enrolled fee-for-service (FFS; Medicare parts A and B) beneficiaries.
Methods We analysed claims and enrolment information from 42 529 117 FFS Medicare beneficiaries using three mesothelioma case definitions (broad, intermediate and narrow) with varying levels of diagnostic requirements. Results are presented as ranges of values for the three definitions.
Results Among FFS beneficiaries, 8213–19 036 beneficiaries with mesothelioma were identified depending on the case definition. The annual prevalence per 100 000 beneficiaries ranged from 8.8 in 2016 (narrow) to 31.3 in 2019 (broad) and annual incidence per 100 000 beneficiaries ranged from 4.5 in 2019 (narrow) to 12.6 in 2017 (broad). Depending on the mesothelioma case definition, 41.8%–81.5% had available therapy claim information indicating that 7.6%–11.3% received chemotherapy alone, 1.3%–1.5% received radiation alone, and 14.3%–27.0% underwent surgery only, with 4.6%–10.5% receiving all three therapy modalities.
Conclusions Mesothelioma was a prevalent disease among FFS Medicare beneficiaries during 2016–2019, and a limited proportion of beneficiaries received all three therapy modalities. Medicare data build on findings from cancer registry data to enhance our understanding of the mesothelioma burden and therapy patterns.
- Asbestos
- Mesothelioma
- Public Health Surveillance
- Occupational Health
- Health services research
Data availability statement
CMS data are available on approved request through the Research Data Assistance Center https://resdac.org/research-identifiable-files-rif-requests.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
Cancer registry data have been used to previously report mesothelioma incidence and prevalence, but treatment information in registry data are limited.
WHAT THIS STUDY ADDS
Up-to-date estimates of the burden and treatment patterns of malignant mesothelioma among Medicare beneficiaries are reported.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
Medicare data are a component of mesothelioma surveillance. These findings complement other studies of mesothelioma morbidity that are not population based or include limited therapy information.
Introduction
Malignant mesothelioma is a rare, aggressive cancer arising from the tissue lining of the lungs (pleura), heart (pericardium), abdomen (peritoneum) or testes (tunica vaginalis). Pleural mesothelioma accounts for approximately 90% of cases and is the focus of most clinical trials.1 2 Most cases of malignant mesothelioma are caused by exposure to asbestos fibres, and the latency from initial exposure to diagnosis is generally 20–50 years.2 A high proportion of mesothelioma cases are associated with occupational exposures to asbestos fibres in industries such as construction and manufacturing, and mesothelioma incidence and mortality are approximately fourfold and sixfold higher among men compared with women, respectively.3 4 Although asbestos production and use declined sharply in the USA since the 1970s, the overall incidence of mesothelioma remained mostly flat for decades with the annual number of incident cases beginning to consistently decline only in the last decade, from 3312 cases (0.9 per 100 000 standard population) in 2013 to 2911 cases (0.7 per 100,000) in 2019.3 5 6
Median survival for patients diagnosed with mesothelioma is approximately 1 year, and 5-year survival is less than 10%.2 7 Treatment therapy decisions including chemotherapy, surgical resection and radiation therapy for mesothelioma are informed by tumour stage and histological subtype as well as patient symptoms, functional status, presence and severity of chronic conditions, and other factors.2 7 The American Society of Clinical Oncology recommends chemotherapy be offered to all patients with mesothelioma to improve survival and quality of life.7 While not all mesothelioma patients are candidates for surgical resection, this therapy option may be recommended for select patients with early-stage disease in conjunction with additional therapy (ie, chemotherapy and radiation therapy). However, many patients do not receive recommended therapy.2 8 In a study of mesothelioma patients in the National Cancer Data Base (NCDB), those who received trimodal therapy (chemotherapy, surgical resection and radiation therapy) had longer survival than those who received fewer therapy modalities.9 More often, malignant pleural mesothelioma patients in the NCDB received chemotherapy alone (32%).9 Due to a variety of factors related to tumour, patient and/or medical care access characteristics, an estimated 40% of malignant pleural mesothelioma patients received no treatment.9
Cancer is a reportable condition in all U.S. states and is one of the only chronic diseases for which complete national incidence data are available.8 10 Cancer registries report all incident cases of invasive cancer and are a gold standard for public health surveillance, collecting information on patient demographics, tumour site, initial treatment course and survival.10 However, because a patient’s cancer therapy can span months or years and the regimen often changes over time, obtaining complete treatment information is challenging for cancer registries given the need to balance completeness of data collection with timeliness of reporting.8–11
Medicare is the primary federal health insurance for most persons (94% in 2019) aged ≥65 years in the USA as well as younger individuals receiving disability insurance benefits or those diagnosed with end-stage renal disease.12 13 In 2019, 18% of the US population were Medicare beneficiaries (61.5 million people) and approximately 50% of Medicare beneficiaries were continuously enrolled fee-for-service (FFS; also known as Medicare parts A and B) beneficiaries with available Medicare claims data.14 15 Since most mesothelioma cases are identified in older adults, Medicare claims data could provide important insight into mesothelioma morbidity and therapy patterns in the USA. In this study, we analyse Medicare data from 2016 to 2019 to estimate the burden of malignant mesothelioma among continuously enrolled FFS beneficiaries and describe the mesothelioma therapy they received.
Methods
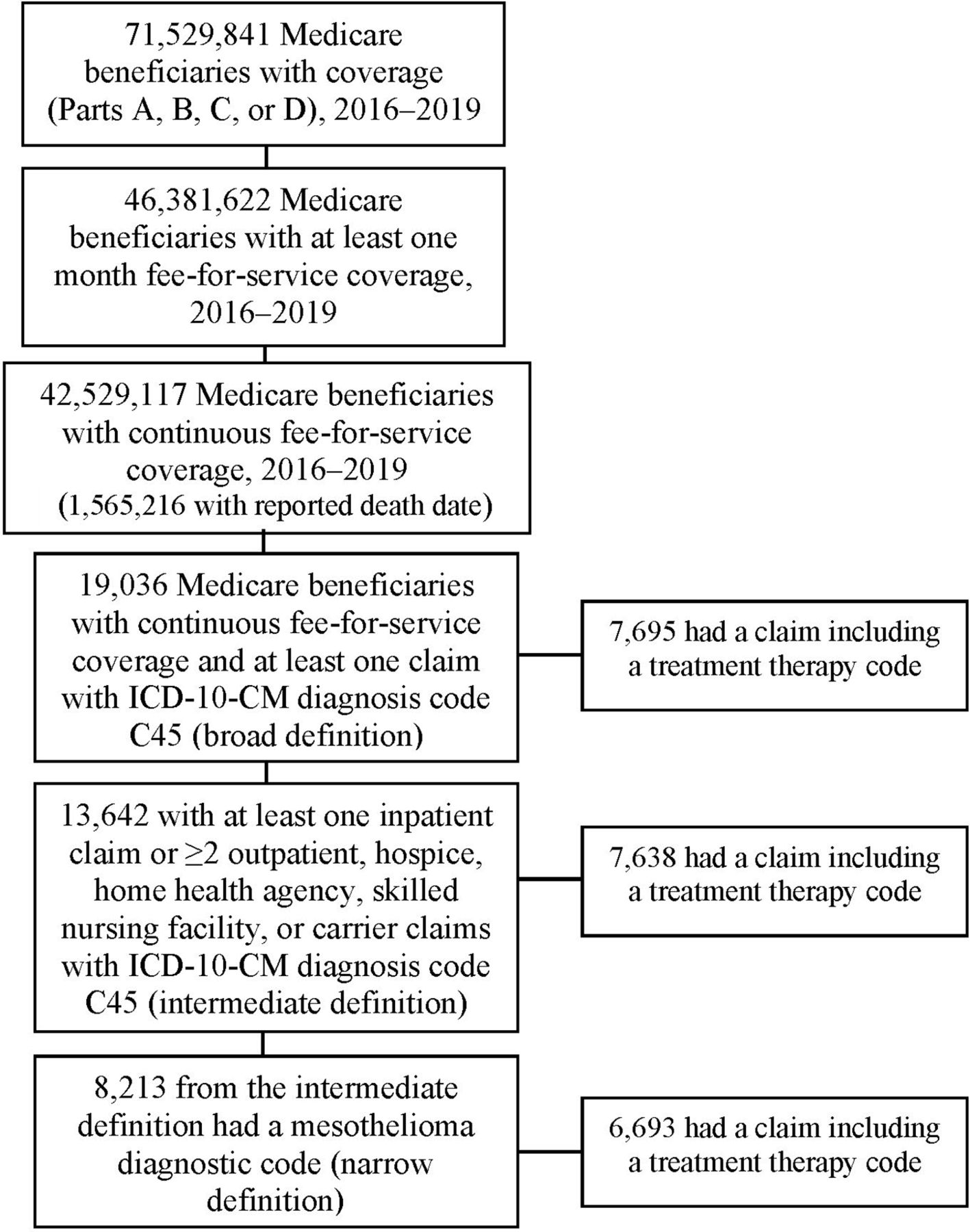
We accessed FFS Medicare claims and Medicare beneficiary data files through the Centers for Medicare & Medicaid Services (CMS) Virtual Research Data Center.16–18 From 2016 to 2019 Medicare claims files, we extracted final action institutional inpatient hospital, outpatient, hospice, home health agency (HHA) and skilled nursing facility (SNF) claims and non-institutional carrier claims (submitted by non-institutional professional providers, for example, physicians, nurse practitioners) for Medicare beneficiaries with continuous FFS Medicare coverage (figure 1).12 18 Medicare claims starting in 2016 were selected because 2016 was the first full year 10th Revision International Classification of Diseases, Clinical Modification (ICD-10-CM) diagnostic codes C45.0 (mesothelioma of pleura), C45.1 (mesothelioma of peritoneum), C45.2 (mesothelioma of pericardium), C45.7 (mesothelioma of other sites) and C45.9 (mesothelioma, unspecified) were used on Medicare claims. Ninth Revision (ICD-9-CM) codes were used on Medicare claims through September 2015 but specific ICD-9-CM codes for malignant mesothelioma were not available.19 20 Claims include ICD-10-CM diagnosis codes (up to 25 codes for institutional and up to 12 codes for non-institutional claims including a principal diagnosis code identifying the diagnosis chiefly responsible for the services provided) and may include additional healthcare procedure codes.12 21

{kind=link}
Sample selection process for fee-for-service Medicare beneficiaries meeting Mesothelioma case definitions. ICD-10-CM, 10th Revision International Classification of Diseases, Clinical Modification.
For this analysis, three case definitions were used to identify FFS beneficiaries with malignant mesothelioma and to calculate mesothelioma prevalence and incidence during 2016–2019 as was done in previous studies of chronic respiratory disease among Medicare beneficiaries.22 23 These definitions were largely based on patterns of diagnosis codes used by the CMS Chronic Conditions Warehouse to define lung cancer and previous studies estimating the prevalence of chronic respiratory disease in this population.22–24 A broad malignant mesothelioma definition identified beneficiaries with an FFS claim including the ICD-10-CM code C45, mesothelioma (figure 1). A subset of beneficiaries meeting the broad mesothelioma case definition fulfilled the intermediate malignant mesothelioma case definition criteria of having at least one inpatient claim listing the ICD-10-CM mesothelioma code or having ≥2 other claims (outpatient, hospice, HHA, SNF or carrier claim) including the ICD-10-CM mesothelioma code. An alternative narrow malignant mesothelioma case definition required beneficiaries meeting the intermediate case definition to also have a Healthcare Common Procedure Coding System (HCPCS) code or an ICD-10 Procedure Coding System (ICD-10-PCS) code for a mesothelioma diagnostic procedure (ie, biopsy, imaging).7 25 A complete list of HCPCS codes and ICD-10-PCS codes for the mesothelioma narrow case definition are presented in the supplement although results of diagnostic procedures are unavailable in Medicare claims (see online supplemental file 1). Due to the limitations associated with accurately identifying malignant mesothelioma among health insurance claims using ICD-10-CM diagnosis codes and the limited availability of procedure codes on Medicare claims, the application of three case definitions helps address these challenges by providing a range of values for mesothelioma prevalence and incidence.
Supplemental material
A beneficiary meeting one or more of the mesothelioma case definitions was considered prevalent from the first day of their first claim listing mesothelioma during 2016–2019 until they died or were otherwise not continuously enrolled in FFS Medicare.22 Multiday claims where the first claim day was in 2015 and the claim carried into 2016 (n=167) were recorded as 2016. Cumulative prevalence of mesothelioma from 2016 to 2019 was calculated as the sum of all unique prevalent cases divided by the total number of FFS Medicare beneficiaries enrolled from 2016 to 2019. Annual prevalence per 100 000 FFS Medicare beneficiaries was calculated using the number of prevalent mesothelioma cases each year as the numerator and total number of continuously enrolled FFS Medicare beneficiaries for that year as the denominator.
Incident mesothelioma cases were identified among prevalent cases who were (1) continuously enrolled in Medicare the year prior to their first mesothelioma claim and (2) without a claim including the mesothelioma diagnosis code (ICD-10-CM C45) prior to their first mesothelioma claim. We limited the ‘clean’ continuous enrolment period to 1 year due to mesothelioma’s typically rapid progression and low survival rate as well as the limited period for which data were available. Annual incidence per 100 000 FFS Medicare beneficiaries was defined as the total number of FFS Medicare beneficiaries with an initial mesothelioma claim for a given year divided by the total number of FFS Medicare beneficiaries continuously enrolled in the previous year. Total incidence is the sum of all incident cases from 2017 to 2019 divided by all FFS Medicare beneficiaries with at least 1 year of continuous enrolment from 2016 to 2018.
Additional procedure information was available for some claims with HCPCS and ICD-10-PCS codes and was used to describe therapy received including chemotherapy, radiation therapy or surgical resection (See online supplemental file 1).21 Some inpatient, outpatient, hospice, HHA, SNF and carrier claims include HCPCS codes and some inpatient, outpatient and SNF claims include ICD-10-PCS codes to bill for care. Unlike the ICD-10-CM diagnosis codes, the HCPCS and ICD-10-PCS codes are incomplete when they are not the basis for payment, so not all claims had available therapy information. All FFS claims for beneficiaries meeting each case definition were searched for available therapy information, not just claims fitting the criteria for the case definition of interest (figure 1).
Medicare claims were linked to Master Beneficiary Summary File (MBSF) base segments using the beneficiary identification number.17 From MBSF base segment data, we extracted information on a beneficiary’s age, date of birth, sex, race, state of residence and original reason for Medicare entitlement from the year of their first broad, intermediate or narrow mesothelioma claim depending on the case definition starting in 2016.12 17 Race groupings included white, black, Hispanic, other (Asian, North American Native or other race), and unknown. A beneficiary’s original reason for Medicare entitlement included aged ≥65 years, aged <65 years and receiving Social Security Administration disability insurance benefits for 24 consecutive months or any beneficiary with end-stage renal disease/end-stage renal disease and disability insurance benefits.12 17 Groups were compared using the χ2 test and differences at p<0.05 were considered significant. Analyses were conducted in SAS Enterprise Guide V.7.1 (SAS Institute). Support for this work was obtained from the National Occupational Research Agenda Intramural Research Competition, National Institute for Occupational Safety and Health, Centers for Disease Control and Prevention (CDC).
Results
Among 42 529 117 Medicare beneficiaries with continuous FFS coverage during 2016–2019, a total of 19 036 (4-year prevalence 44.8 per 100 000 beneficiaries), 13 642 (32.1) and 8213 (19.3) beneficiaries met the broad, intermediate and narrow malignant mesothelioma case definitions, respectively. Selected demographic characteristics of beneficiaries at the time of their first prevalent claim during the study period are presented by case definition in table 1. Compared with the entire Medicare FFS population, Medicare FFS beneficiaries with mesothelioma were more likely to be ≥75 years of age, male, white and originally enrolled in Medicare due to age ≥65 (p<0.05) for all three case definitions. At the time of their first prevalent mesothelioma claim, most beneficiaries were ≥65 years, male, white and were originally entitled to Medicare coverage due to age. Still, mesothelioma was also prevalent among the smaller subpopulations of beneficiaries <65 years of age enrolled in Medicare due to disability (n=3555) and due to ESRD (n=108).
Demographic and claim characteristics of fee-for-service Medicare beneficiaries with prevalent mesothelioma by case definition, 2016–2019
The 472 580 claims among beneficiaries meeting the intermediate case definition included the mesothelioma principal diagnosis codes for (1) mesothelioma of the pleura (n=1 63 444); (2) mesothelioma unspecified (n=86 429); 3) mesothelioma of the peritoneum (n=34 796); 4) mesothelioma of other sites (n=27 496); and mesothelioma of pericardium (n=732). Other common principal diagnosis codes for claims among beneficiaries meeting the intermediate mesothelioma case definition were encounter for antineoplastic chemotherapy and immunotherapy (n=23 534) and pleural effusion (n=7298). Healthcare claims were most often from a carrier (68.5%) or outpatient (23.9%) setting.
The 4-year prevalence of mesothelioma ranged from 19.3 (narrow case definition) to 44.8 (broad case definition) cases per 100 000 beneficiaries with an annual prevalence ranging from 8.8 (2016 narrow case definition) to 31.3 (2019 broad case definition) cases per 100 000 beneficiaries. Using the intermediate case definition, the estimated annual mesothelioma prevalence was 15.8 per 100 000 beneficiaries in 2016 and 20.7 per 100 000 beneficiaries in 2019 (table 2).
Annual mesothelioma prevalence and incidence by case definition, fee-for-service Medicare beneficiaries 2016–2019
During 2017–2019, 12.4 (narrow case definition) to 28.6 (broad case definition) cases per 100 000 beneficiaries were identified for a 3-year cumulative incidence rate. The annual incidence rate ranged from 4.5 (2019 narrow case definition) to 12.6 (2016 broad case definition) cases per 100 000 beneficiaries (table 2). Using the intermediate case definition, the estimated annual mesothelioma incidence was 8.8 per 100 000 beneficiaries in 2017 and 6.8 per 100 000 beneficiaries in 2019 (table 2).
Among 13 642 beneficiaries meeting the intermediate mesothelioma case definition, 56.0% (n=7638) had available claim information indicating therapy including (1) chemotherapy (33.8%), (2) radiation therapy (11.9%) or (3) surgery (42.8%) code. Chemotherapy alone was received by 9.1%, 1.5% received radiation alone, and 19.3% underwent surgery only, with 6.4% receiving all three therapy modalities (table 1). More than half (53.5%) of the 7638 beneficiaries meeting the intermediate mesothelioma case definition with available therapy information received one type of therapy, 35.1% received two types of therapy and 11.4% received three types of therapy.
Discussion
We analysed a population-based administrative database of US adults primarily ≥65 years of age to estimate the prevalence and incidence of malignant mesothelioma using tiered case definitions and evaluated available therapy codes to characterise therapy patterns. To our knowledge, complete Medicare data have not previously been used for mesothelioma surveillance and this study builds on algorithms developed to facilitate claims-based case definitions for the prevalence and incidence of other chronic conditions among Medicare beneficiaries.22 23
The intermediate case definition excluded beneficiaries meeting the broad case definition with only one non-inpatient claim and was intended to identify beneficiaries with multiple mesothelioma claims or an inpatient hospitalisation, which could be potential indicators of disease severity. Thus, the intermediate case definition retained 98.8% of the broad case definition claims but only 71.7% of the broad case definition beneficiaries. Proportionally, there were more inpatient and outpatient claims among the 53 782 claims associated with patients meeting the narrow case definition, underscoring differences in care settings for these patients.
During 2017–2019, the overall incidence ranged by case definition from 12.4 to 28.6 per 100 000 beneficiaries with an annual incidence ranging from 4.5 to 12.6 per 100 000 beneficiaries and a decline from 2017 to 2019. The decline in incidence could be explained in part by methodological factors that artificially inflate the incidence at the beginning of the study period since those with disease onset prior to 2017 are included as incident cases. However, a decline or stable mesothelioma incidence trend over the past decade in the USA is also reported by prior studies of cancer registry data.3 6
Previous studies reported mesothelioma incidence using population-based cancer registry data covering 97% of the US population (the National Cancer Institute’s Surveillance, Epidemiology and End Results (SEER)-affiliated registries in combination with the CDC National Program of Cancer Registries).6 It is important to note that US Cancer Statistics are based on more rigorous diagnostic criteria and 94% of mesothelioma diagnoses are confirmed with a biopsy, unlike case definitions in the current study which are exclusively claims-based.6 In 2017, there were 3196 new cases of mesothelioma, declining to 2948 in 2018 and 2911 in 2019.3 The broad case definition in our study includes more individuals than the number of registry-reported incident cases, but the intermediate case definition appears to better represent the true number of cases in the Medicare population. Among FFS Medicare beneficiaries, the intermediate case definition identified 2721 incident cases in 2017, 2299 in 2018, and 2067 in 2019. While these case counts are slightly lower than US Cancer Statistics registry-reported cases in the US population, this was expected because Medicare beneficiaries who were enrolled in a managed care plan (Medicare part C) during the study period were excluded as were younger patients not enrolled in Medicare but with mesothelioma. The 1540 beneficiaries <65 years of age meeting the broad mesothelioma case definition are primarily disabled and receiving disability insurance benefits after having worked a qualifying number of years, although it is unknown if mesothelioma is the cause of their disability. According to CDC’s 2019 cancer statistics, most mesothelioma cases occurred in males (73.5%) and whites (90.7%) and the numbers of new mesothelioma cases by state were highest in California, Texas, Florida, New York, Pennsylvania, Illinois, New Jersey, Ohio and Michigan.3 These demographic characteristics are similar to those of FFS Medicare beneficiaries meeting the mesothelioma case definitions.
We found a higher prevalence of mesothelioma among males compared with females for all three case definitions. Incidence data from 1999 to 2018 show the rate of all (pleural and peritoneal) malignant mesothelioma cases and pleural mesothelioma declined for males and females combined, for males only and for females only, but the incidence rate of peritoneal malignant mesothelioma has increased among females and among males and females combined during this time.6 An additional analysis of our mesothelioma prevalence and incidence by sex (data not shown) reflected similar findings for males and females separately as the overall results presented in table 2. The increase in incidence among females with peritoneal mesothelioma was not evident in our analysis likely due to the limited proportion of claims with mesothelioma of the peritoneum (C45.1) listed as the ICD-10-CM principal diagnosis (7.4%).
A study of pleural mesothelioma survival and treatment patterns in adults using the 2004–2013 NCDB, which included approximately 70% of all incident cancer cases in the United States, identified 19 134 malignant pleural mesothelioma cases. Among these patients, 47.6% received chemotherapy, 6.6% received radiation and 22.6% received surgery as a part of their treatment.9 Results from the NCDB study were similar to a study of chemotherapy and surgery treatment patterns from 2005 to 2009 SEER-Medicare linked data, including about 25% of US patients with cancer ≥65 years of age, which identified 1625 pleural or peritoneal mesothelioma patients. Of these patients, 44.7% received chemotherapy and 29.9% received surgery as a part of their treatment.11 In our study, of those meeting the intermediate case definition with any type of mesothelioma (pleural, peritoneal, pericardial, other sites or unspecified), only 33.7% had any chemotherapy code but 42.7% had any surgery code and 11.9% had any radiation code. Furthermore, in our study of Medicare beneficiaries meeting the intermediate mesothelioma case definition, 19.3% of patients received a combination of two modalities and 6.4% received trimodal therapy during 2016–2019. Trimodal therapy in our study of Medicare beneficiaries with any type of mesothelioma (pleural, peritoneal, pericardial, other sites or unspecified) was higher than the 3% reported previously in a 2004–2013 national study of adults (>18 years of age) with malignant pleural mesothelioma.9
Differences in the proportions of patients receiving therapies in our study compared with prior studies may be due to differences in the patient population (eg, functional status, presence and severity of chronic conditions and other factors)2 7 Furthermore, our study includes all types of mesothelioma, not just pleural mesothelioma which is commonly treated with chemotherapy. Pleural mesothelioma accounts for most (90%) cases of mesothelioma but only 46.6% of beneficiaries meeting the broad case definition had any mention of mesothelioma of pleura (C45.0) on their Medicare claims (data not shown).2 However, mesothelioma of pleura cases could have been reported as mesothelioma ‘unspecified’ or of other sites on Medicare claims. Our study found a similar proportion of FFS Medicare beneficiaries meeting the intermediate case definition did not have available information for therapy (44%) when compared with patients included in the NCDB study (44.0%).9
Because specific ICD-CM codes for malignant mesothelioma were not available prior to 2016 and ICD-9-CM surrogate codes for malignant mesothelioma substantially underestimate the mortality burden of mesothelioma, we began analysing claims starting in 2016.19 20 Therefore, annual calculations for the earlier years of this study period (ie, 2016 and 2017) are likely incomplete and may underestimate incidence and prevalence. For example, prevalent cases were not counted as such until they sought medical care for mesothelioma starting in 2016. Incident cases were calculated after a 1-year clean continuous enrolment period, which was selected due to mesothelioma’s typically rapid progression and low survival rate as well as limited available data and might be overestimated in later study years. Patients with disease onset prior to 2016 may have erroneously been counted as new (incident) cases despite the 1-year clean enrolment period. However, additional years of data would allow for a longer clean period, which may provide a better estimate of true incidence.
Furthermore, receipt of therapy is likely underestimated in this study. Therapy claims prior to 2016 were not included in this analysis and complete therapy-related information was not always available on claims. Additional treatment information (ie, therapy offered, therapy offered but refused, therapy offered but inaccessible) and information on the therapy modes for which a patient qualifies would enhance our understanding of how mesothelioma is treated. We also used a claims-based definition to identify therapy based on common therapy codes for chemotherapy, radiation therapy and surgery (to identify surgical resection). Therapy codes used in this study may not be inclusive of all multidisciplinary therapy options for mesothelioma since treatment options are continuing to evolve and develop.2 7
To access all available Medicare claims, this analysis was restricted to Medicare beneficiaries with continuous FFS Medicare coverage which ranged annually from 54% of all Medicare beneficiaries in 2016 to 49% in 2019.15 It may not be representative of the Medicare population because Medicare beneficiaries ever enrolled in a managed care plan from 2016 to 2019 were not included due to the proprietary nature of part C claims. Furthermore, results may not represent the Medicare FFS population since continuous enrolment until death was required.
Conclusions
The findings of this population-based study complement other studies of mesothelioma morbidity that are not population based or include limited therapy information. They help enhance our understanding of the burden of mesothelioma and therapy patterns among the Medicare FFS population. In addition, they provide insight into mesothelioma surveillance among those aged ≥65 years to help monitor disease burden over time in other populations. Medical claims data collected for administrative purposes can be an important complement to cancer registry data, which usually contain limited treatment-related information.
Data availability statement
CMS data are available on approved request through the Research Data Assistance Center https://resdac.org/research-identifiable-files-rif-requests.
Ethics statements
Patient consent for publication
Acknowledgments
The authors would like to acknowledge Megan Casey and David Weissman (NIOSH/CDC) and Jane Henley (DDNID/CDC) for providing helpful comments and critique of the manuscript.
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Contributors LK and DJB participated in the conception and design of the work; LK participated in the analysis of data and drafted the work; LK, JMM and DJB participated in the interpretation of data for the work, revised drafts of the work, and provided the final approval of this article to be published and agree to be accountable for all aspects of the work. LK is responsible for the overall content as the guarantor.
Funding Support for this work was obtained from the National Occupational Research Agenda Intramural Research Competition, NIOSH, CDC. Award/grant number not applicable. All authors are employees of the Federal Government and all work was performed as part of their official duties.
Disclaimer The findings and conclusions of this report are those of the authors and do not necessarily represent the view of the National Institute for Occupational Safety and Health.
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.