Article Text

Abstract
Objectives Previous research has suggested that women firefighters may have a greater risk of adverse reproductive outcomes compared with non-firefighting women. In this study, we investigated the association between firefighter occupational factors and risk of preterm birth.
Methods This cross-sectional analysis of US firefighters surveyed in 2017 compared preterm birth among firefighters to non-firefighters using age-at-pregnancy-standardised prevalence ratios. Generalised estimating equations estimated relative risks and 95% CIs between firefighter occupational factors (career or volunteer, wildland status, shift schedule, fire responses, work restriction) and preterm birth risk. We adjusted for age-at-pregnancy, education, gravidity, BMI, and smoking and considered effect modification by age-at-pregnancy and career versus volunteer status.
Results Among 934 women who reported 1356 live births, 12% were preterm (n=161). Preterm birth prevalence among firefighters was 1.41 times greater than non-firefighters (95% CI 1.18 to 1.68). Among wildland and combination wildland/structural firefighters, volunteers had 2.82 times the risk of preterm birth (95% CI 1.19 to 6.67) compared with career firefighters. Firefighters who started restricting their work in the 2nd trimester had a nonsignificant 0.67 times lower risk of preterm birth than those who started in the 3rd trimester or did not restrict work at all (95% CI 0.43 to 1.03).
Conclusions Firefighters may have greater risk of preterm birth than non-firefighters, which could be influenced by roles in the fire service and work restrictions taken.
- Firefighters
- Pregnancy Outcome
- Occupational Health
Data availability statement
Data are available on reasonable request. The data generated or analysed during the current study are not publicly available due to restrictions based on the consent forms and IRB application for this study but are available from the authors on reasonable request.
This is an open access article distributed in accordance with the Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which permits others to distribute, remix, adapt, build upon this work non-commercially, and license their derivative works on different terms, provided the original work is properly cited, appropriate credit is given, any changes made indicated, and the use is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
Statistics from Altmetric.com
WHAT IS ALREADY KNOWN ON THIS TOPIC
Women firefighters may be at greater risk of adverse pregnancy outcomes, including pregnancy loss, and potentially, preterm births.
WHAT THIS STUDY ADDS
The prevalence of preterm birth is elevated among firefighters compared with non-firefighters.
Compared with career firefighters (full-time, salaried), volunteer firefighters are a particularly vulnerable subgroup within the fire service.
HOW THIS STUDY MIGHT AFFECT RESEARCH, PRACTICE OR POLICY
This research suggests that women firefighters may benefit from increased occupational protections to reduce the risk of preterm birth.
Introduction
Firefighting exposes firefighters to a variety of toxic substances and physical hazards. However, research concerning the health of women firefighters is limited, and reproductive health topics remain understudied. Previous observational studies suggest that women firefighters experience more adverse reproductive outcomes, such as pregnancy loss, preterm birth and hospital admissions for adverse pregnancy, childbirth and postpartum outcomes compared with non-firefighters.1–3 Some potential occupational exposures (air pollutants, perfluoroalkyl and polyfluoroalkyl substances (PFAS), and high temperatures) have also been associated with adverse reproductive outcomes among non-firefighters.4–7 Firefighters could be particularly vulnerable to these exposures, given their high level of exposures.8–10
Research among career (full-time, salaried) firefighters in the USA has shown that pregnancies to working firefighters were more than twice as likely to result in self-reported pregnancy loss compared with non-firefighters.1 However, exposures vary by firefighter type because of differences in time at fires, combustion products, activities and equipment used.11 12 US firefighters can be categorised by employment status (career or volunteer (part-time or on-call) or by wildland firefighter status (wildland only, combination of wildland and structural firefighting, or structural only). Firefighters may have increased risk for miscarriage which varies by both employment and wildland fire response.3 However, it is unclear whether there are similar patterns of risk regarding preterm births. Therefore, we analysed data from a cohort of US women firefighters to determine (1) the prevalence of preterm births for firefighters compared with a general population of non-firefighters and (2) potential occupational factors among firefighters that contributed to risk of preterm birth.
Methods
Study participants
The Health and Wellness of Women Firefighters Study, a cohort of women firefighters from the USA and Canada, was conducted by the Center for Fire, Rescue & EMS Health Research of NDRI-USA to examine the work environment, health and perceived experiences of women firefighters. Recruitment and methodology have been previously reported.3 13 Women firefighters are hard to recruit using traditional methods, so the study used snowball sampling, non-probability sampling where current participants recruit additional participants.14 Participants were initially identified using affinity group email lists1 13 and asked to complete surveys in 2017 and 2019. Data used in the current analysis were self-reported during the 2017 survey.
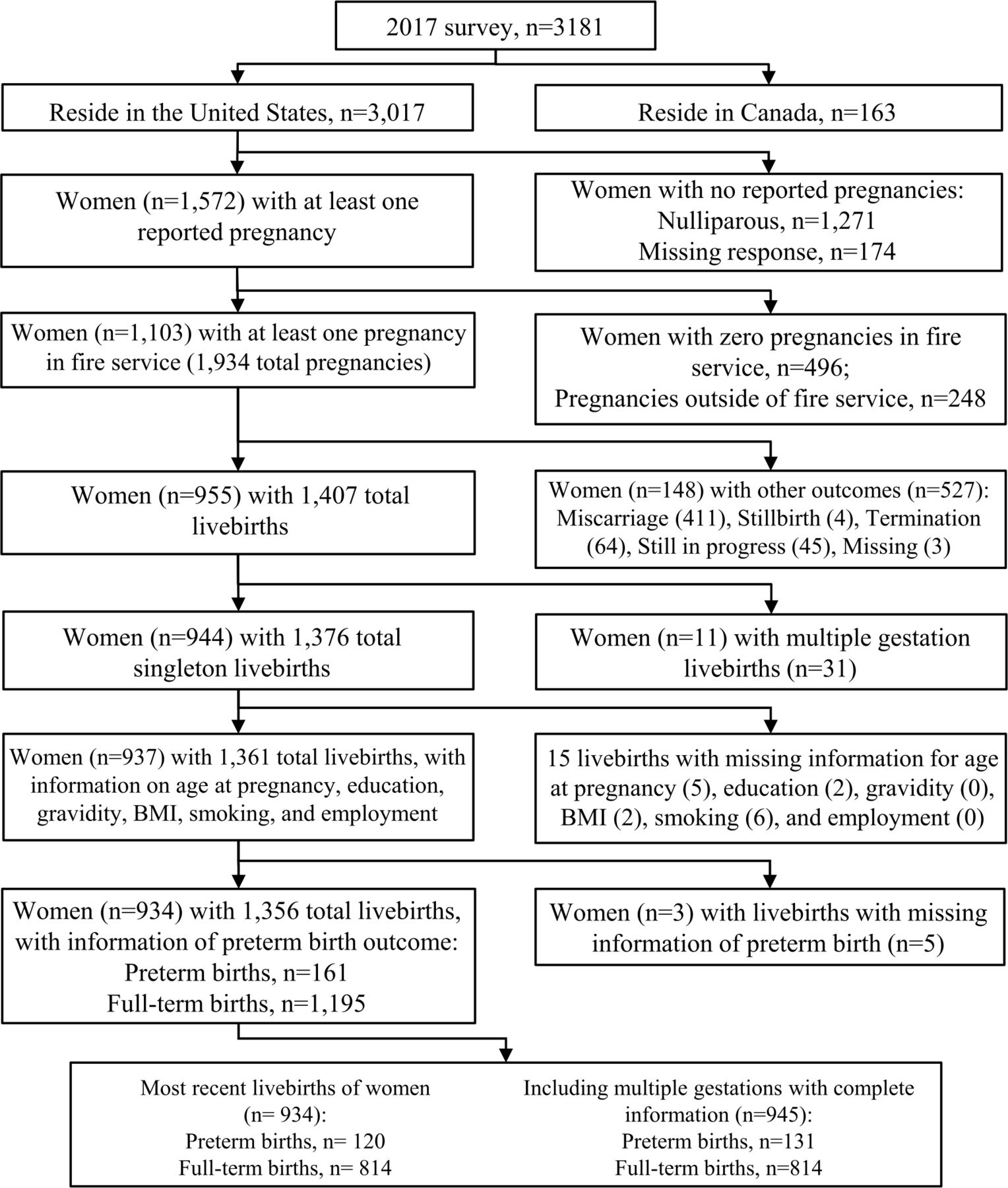
Among firefighters who completed the survey in 2017 (n=3181), we excluded Canadian firefighters (n=163) because strategies, tactics and protective equipment may vary by country (figure 1). Women who had never been pregnant (n=1271), were missing parity information (n=174) or had no pregnancies while working in the fire service (n=496) were excluded. We also excluded pregnancies that occurred while not working in the fire service (n=248). Singleton, live birth pregnancies (n=1376) were considered for our main analysis; miscarriages (n=411), stillbirths (n=4), terminations (n=64), pregnancies ongoing at the time of survey (n=45), multiple gestations (n=31), or pregnancies with missing outcomes (n=3) were excluded. Pregnancies with missing responses to whether the birth was preterm or full-term (n=5) were also removed. Missing responses for age-at-pregnancy, education, gravidity, BMI and smoking were excluded from our main analysis, which included a total of 934 women and 1356 pregnancies.
{kind=link}
Women from the health and wellness of women firefighters study included in analysis of preterm births (934 firefighters and 1356 total live births).
Data collection
Outcome measurement
Firefighters answered questions for a maximum of 10 pregnancies (<1% reported 10 pregnancies). For each live birth pregnancy, participants were asked ‘Was your baby from pregnancy X born more than 3 weeks before his/her due date?’ (yes, no, don’t know/don’t remember). A preterm birth was defined as a live birth born more than 3 weeks before the expected due date. ‘Don’t know/don’t remember’ responses were defined as missing.
Occupational factor measurement
Exposures of interest included employment status, wildland firefighter status and shift schedule (among career firefighters) based on report in 2017. Employment was categorised as either career or volunteer firefighter (‘Are you primarily a career or volunteer firefighter?’). For wildland firefighter status (‘Are you a wildland firefighter?’), wildland firefighters reported they only respond to wildland fires, combination firefighters that they were wildland firefighters in addition to working for a career or volunteer fire department (Yes, I do wildland firefighting in addition to working for a career/volunteer department), and structural firefighters reported not being wildland firefighters. Participants were categorised as wildland/combination firefighter or structural firefighter. Shift schedule among career firefighters was categorised as working at least 24 consecutive hours at a time or working less than 24 consecutive hours at a time (online supplemental file 1). We also examined pregnancy-specific exposures (online supplemental file 1): working fire/rescue calls at pregnancy start (‘Were you actively running fire or rescue calls when you found out you were pregnant for your pregnancy?’ yes or no); fire responses during pregnancy (‘Approximately how many working fires did you fight during your pregnancy?’, 0, 1–4, >4 fires); work restriction due to pregnancy (‘Were your duties restricted during your pregnancy?’, yes or no); and start of work restriction during pregnancy (‘Approximately how many weeks into your pregnancy were you when your duties were restricted?’, weeks 0–12, 13–26 or 27+ which includes no restrictions taken).
Supplemental material
Other variables of interest
All variables mentioned here are further described in online supplemental file 1. Individual-level variables of interest included highest education (some college or less, or college and above), BMI (<30 kg/m2 or ≥30 kg/m2) at the time of the survey, and Hispanic, Latina or Spanish origin (yes or no). Descriptive race categories included white, Black, Asian, Native Hawaiian or other Pacific Islander, American Indian or Alaska Native, or other. Analytical race categories were white or other racial minority. Smoking was categorised as current/former or never-smoker at the time of the survey. Current smokers smoked more than 100 lifetime cigarettes and smoking in the past 30 days. Former smokers smoked more than 100 lifetime cigarettes but not in the past 30 days. Never-smokers smoked less than 100 cigarettes. Pregnancy-level variables of interest included age-at-pregnancy, gravidity (previously pregnant or not), previous preterm birth (nulligravid, yes, no), gestational hypertension (yes or not reported). Additional descriptive variables included presence of pregnancy/maternity policies, annual household income, menopausal status, current rank, and who restricted work during most recent pregnancy (doctor, department or self).
Statistical analysis
Prevalence of preterm birth compared with US general population
To compare firefighters in our analysis to non-firefighters, we calculated age-at-pregnancy standardised prevalence ratios (aSPRs) and 95% CIs of preterm birth for most recent live births while working in the fire service. aSPRs were calculated using indirect age-standardisation methods and two US studies as the comparison groups.15 16 The first comparison group was the US general population, consisting of data on almost 3.8 million US births recorded in 2018 collected via birth certificates.16 This report by Martin et al, published by the US Centers for Disease Control and Prevention, described birth trends using birth certificate data and included pregnancies with multiple gestations in their analysis. Because we could not obtain data excluding multiple gestations, we added firefighters to our analysis group who had been previously excluded because of multiple gestation pregnancies (n=11), for this analysis only.
Prevalence of preterm birth compared with Nurses’ Health Study II
Using the methods described above, we also compared preterm births during most recent live birth while in the fire service to the Nurses’ Health Study II (NHSII).15 The NHSII is a prospective cohort study of 116 608 US female nurses aged 25–42 at enrolment.17 The study, by Lawson et al, examined a subset of NHSII participants who retrospectively self-reported details about their most recent pregnancy including outcome and occupational exposures.15
Firefighter occupational factors associated with risk of preterm birth
Statistical models
Analyses of firefighter occupational factors were restricted to women in the fire service. We used generalised estimating equations (GEE) with a Poisson distribution, log link function, exchangeable working correlation matrix and sandwich variance estimators, allowing us to directly estimate relative risks (RR) of preterm births, and 95% CIs.18 A log-binomial distribution was initially considered; however, non-convergence in our models resulted in the selection of a Poisson distribution as a more numerically stable method.18 19 GEE accounted for correlation between multiple potential pregnancies per firefighter, allowing us to consider all live births to firefighters that occurred while working in the fire service in our models.
A priori confounders
All variables selected for adjustment in models were specified a priori. We adjusted for age-at-pregnancy (model 1), a risk factor for preterm birth,20 modelled as age-at-pregnancy and age-at-pregnancy-squared since its association with preterm birth risk has been reported to be non-linear.16 20 We also included education, gravidity, BMI and smoking in model 2 as categorical variables because they have been previously associated with increased risk for preterm birth21–24 and a priori hypothesised to be associated with occupational factors. For models examining pregnancy-specific exposures (worked fire/rescue calls, number of fire responses, work restrictions (yes or no), and timing of start of work restrictions), we additionally adjusted for employment status (model 3). Call volumes and policies generally vary between career and volunteer departments, and could impact occupational exposures.3
Effect modification assessment
We considered effect modification for the risk of preterm birth by age-at-pregnancy (<35 years or≥35 years) as women≥35 during pregnancy have increased risk of preterm birth compared with women who are <35,20 and age-at-pregnancy may modify the association of potential firefighter occupational exposures and preterm birth. We also considered if associations varied by employment status (career or volunteer firefighter), because of overlap between employment and wildland firefighter statuses and that annual call volumes differ between career and volunteer fire departments.25 We tested for effect modification by creating an interaction term for the occupational factor and potential modifying factor. We presented stratified results when effect modification was present.
Sensitivity analyses
Sensitivity analyses were performed to test the robustness of our findings. Models used in sensitivity analyses were based on main analysis models. We evaluated associations between occupational factors and risk of preterm birth in two scenarios to assess if length of recall affected results: (1) restricted to the most recent pregnancy and (2) restricted to the first pregnancy. Second, we used multiple imputation with chained equations to assess whether the exclusion of pregnancies with missing responses of confounders (age-at-pregnancy, gravidity, BMI, smoking and education) influenced the results.26 We included factors from the main analytical model, the outcome, factors associated with missingness and auxiliary factors correlated with predictors to be imputed (Kendall’s t>0.20).27 Twenty complete datasets were imputed and analysed. Estimates were pooled using Rubin’s Rules.28 Third, we adjusted for additional known risk factors for preterm birth which were not included in our main models, such as previous preterm birth (nulligravid, no, yes; including those that may have occurred while not working in the fire service),22 and gestational hypertension (yes, not reported)23 using write-in responses from participants who reported experiencing medical complications during pregnancy, specifically relating to gestational hypertension/preeclampsia. We performed statistical analyses using SAS V.9.4 software.
Results
Our analysis included 934 firefighters and 1356 total live births, 12% of which were preterm (n=161) (figure 1). Among most recent live births, 13% were preterm (n=120). Participants had a median age of 38 (IQR=34–45), were mostly white (93%), non-Hispanic (95%) and married or in a partnership (81%) (table 1). About 17% of firefighters were obese, 4% were current smokers and 17% were former smokers. Median lifetime pregnancies was 2 (IQR 1–3), and only 6% (n=53) reported three or more live births while working in the fire service.
Characteristics of firefighters at survey in 2017 with at least one live birth, stratified by employment and wildland firefighter status, n=934*
Participants were mostly career (88%) and structural firefighters (64%). Only 74% reported that their departments had policies related to pregnancy or maternity. Median time between most recent pregnancy and survey was 6 years (IQR 2–12) and median number of fires during pregnancy was three (IQR 0–8). Most restricted their duties during their most recent pregnancy (23% did not restrict).
Prevalence of preterm birth compared with US general population and NHSII
The prevalence of preterm births among all firefighters was 1.41 times greater (95% CI 1.18 to 1.68) than US women in 2018, and also elevated among volunteers (aSPR 2.29, 95% CI 1.51 to 3.34) and career firefighters (aSPR 1.28, 95% CI 1.05 to 1.56) (table 2).16 Preterm birth among structural firefighters was also greater than US women (aSPR 1.77, 95% CI 1.45 to 2.13). We observed no difference in preterm birth comparing wildland/combination firefighters to US women (aSPR 0.72, 95% CI 0.46 to 1.08). Similar patterns were observed when we compared preterm births among firefighters to US nurses (table 2).15
Age-standardised prevalence ratios comparing preterm births among most recent live birth of firefighters with non-firefighting US populations
Firefighter occupational factors and risk of preterm birth
Among firefighters, volunteer status was associated with increased risk of preterm birth but varied by wildland firefighter status (model 2 interaction p=0.09) (table 3). Among wildland/combination firefighters, volunteer firefighters had 2.82 times greater risk of preterm birth compared with career firefighters (95% CI 1.19 to 6.67), but this association attenuated and lost statistical significance among structural firefighters (RR 1.47, 95% CI 0.92 to 2.33). The association between shift schedule (>24 hours vs less than 24 hours) and risk of preterm birth was negligible (RR 0.88, 95% CI 0.58 to 1.32).
Associations between occupational factors in 2017 and risk of preterm birth among 934 firefighters and 1356 pregnancies*†
Firefighters who started restricting work during the second trimester had 0.67 times the risk of preterm birth in the fully adjusted model (model 3) compared with firefighters who did not restrict their work or did so during the third trimester (95% CI 0.43 to 1.03), though this association was not statistically significant (table 4). Starting work restriction during the first trimester was not associated with risk of preterm birth (RR 1.13, 95% CI 0.77 to 1.64). Working fire/rescue calls at pregnancy start, number of fire responses during pregnancy and work restriction during pregnancy (yes or no) were not associated with the risk of preterm birth (tables 3–4).
Associations between pregnancy-specific occupational factors and risk of preterm birth among 934 firefighters and 1356 pregnancies*†
Our sensitivity analyses generally supported our main analyses (online supplemental file 2). We did observe that when restricted to the first pregnancy in the fire service, the association between employment and risk of preterm birth among wildland/combination firefighters attenuated and was no longer statistically significant (online supplemental file).
Supplemental material
Discussion
The prevalence of preterm birth was greater among firefighters than non-firefighters and the risk of preterm birth varied based on employment, and wildland firefighter status. Among wildland/combination firefighters, volunteers had greater risk of preterm birth than career firefighters. This supports our previous analysis of risk of miscarriage among firefighters,3 and other studies suggesting that firefighters may be at increased risk of adverse reproductive health outcomes.1 2
The prevalence of preterm birth among firefighters was greater compared with two groups of non-firefighters, US women who had a live birth in 2018 and US nurses from the NHSII.15 16 These groups varied regarding data source and study design. Martin et al’s study used birth certificate data to evaluate almost 3.8 million US births in 2018, compared with our use of self-reported survey data. The women in Martin et al were slightly younger (29.0 vs 32 years old) and more racially diverse (52% non-Hispanic white, 23% Hispanic white) than our sample, who were majority non-Hispanic (95%) and white (93%).16 The second comparison group consisted of a subset of nurses from the NHS II (6977 singleton live births).15 Similar to our study, Lawson et al analysed retrospectively self-reported data on pregnancy outcomes and occupational exposures for the most recent pregnancy. Nurses were slightly older compared with firefighters (36 vs 32 years old), but a similar BMI (prepregnancy BMI 24.2 kg/m2 vs 51% of firefighters reporting current BMI ≤24.9 kg/m2).15 However, we were unable to account for different occupational exposures of these occupations that could influence risk for preterm birth.
We used age-at-pregnancy to standardise our prevalence estimates between populations but were unable to account for other population-level differences, a limitation for all standardisation methods.29 For example, wildland and combination firefighters are located mostly within the Western USA, but we were unable to obtain geographically specific preterm birth rates. Interpretations of our findings should consider that though efforts were made to identify reasonably similar comparison populations, population-level differences that were present, aside from age-at-pregnancy, could not be accounted for and may have influenced our results. Based on our study design, data sources and sample characteristics, our analysis of firefighters may be more similar to Lawson et al (nurses) than Martin et al (US general population), however, a comparison to the US general population is valuable to consider for generalisability. Overall, we did observe consistent patterns, supporting previous studies that used indirect comparison methods to demonstrate that adverse reproductive outcomes may be greater in firefighters compared with non-firefighters.1–3
Occupational exposures could help explain why firefighters may experience elevated risk for adverse reproductive outcomes. Systematic reviews and meta-analyses have shown a positive association between air pollution and high environmental temperatures with adverse birth outcomes, including preterm birth, low birth weight and stillbirth.5 30 PFAS are of concern in the fire service because they are used to manufacture turnout gear and some firefighting foams.31 High prenatal PFAS exposures have been associated with increased risk of preterm birth,32 and reducing PFAS exposures may decrease the risk of preterm birth and increase overall fertility.7 Studies should investigate if they contribute to the potential excess of adverse reproductive outcomes among firefighters.
Our results suggest that among wildland and combination firefighters, volunteers have a greater risk of preterm birth compared with career firefighters, contrary to assumptions that volunteers, who generally respond to fewer annual calls, have fewer occupational exposures and lower risk of occupational diseases.25 Mechanisms that may contribute to this difference include access to protective equipment and resources, work schedules (most volunteers are on-call all the time), and exposures related to their full-time jobs. Despite advancements in technologies to prevent or minimise firefighter occupational exposures, financial barriers may make these items less accessible to volunteers. Revenue for such expenses may be largely generated from local taxes, which may be dependent on community size and volunteers generally serve smaller communities. Volunteer departments may also have reduced access to other resources (eg, trained firefighters, department support, training, occupational health providers) compared with career departments. Our findings are consistent with our previous study that observed that volunteer firefighters had greater risk of miscarriage compared with career firefighters.3
We observed that wildland firefighter status modified risk of preterm birth. Wildland and structural firefighters may differ from each other in their cumulative fireground exposures, physical exertion and physiological strain, and mental strain. Wildland firefighters participate in activities not shared by structural firefighters (eg, hiking, constructing fire-lines, prescribed burning) and spend more time at fires compared with structural firefighters, concentrated over a shorter wildland fire season.11 This differences may be exacerbated by the increased frequency and duration of wildland fires in recent years.33 Communities affected by wildland fires have also reported increased respiratory events, cardiovascular diseases, mortality and adverse pregnancy outcomes,4 34 35 highlighting the importance of understanding the impact of these exposures in both environmental and occupational settings.
We did not observe an association between any work restriction during pregnancy (yes or no) and risk of preterm birth. However, our results suggest that when work restrictions begin could potentially be important. Firefighters who started work restrictions during the 2nd trimester may have had lower risk of preterm birth than those who did not restrict work or restricted during the 3rd trimester. However, this association was not statistically significant, therefore additional research is warranted. This aligns with previous research that gestational weeks during the second trimester fall within a critical exposure period where exposure to PM2.5 was associated with increased risk of preterm birth.36 Moreover, non-occupational prenatal wildfire exposure during the 2nd trimester was positively associated with risk of preterm birth, but exposures during the 1st or 3rd trimesters were not.4 Because we lacked information on how work was restricted (eg, move to light duty roles, reduced hours) or the restriction reason (eg, underlying medical condition, high risk pregnancy), future research should collect information on type of work restrictions and investigate the temporality between exposures and restrictions during pregnancy to better inform departmental policies.
We did not observe associations between reported fire responses during pregnancy (working fire/rescue calls at pregnancy start or the number of fire responses during pregnancy) and risk of preterm birth. However, we lacked information on details of fireground exposures (eg, time at fire, role at fire, type of fire) and cumulative history of fire exposure. Collection of this information could help clarify these associations.
This was a large, novel investigation of occupational factors and preterm birth among firefighters. This timely study adds to a sparse body of literature highlighting the need to consider additional occupational protections for women firefighters. In addition, this study provides initial evidence of a potential period of vulnerability during a firefighter’s pregnancy that warrants further investigation.4 36 Importantly, our results were robust across both references samples (US birth certificates and US nurses) and for sensitivity analyses performed.15 16
Still, there are important limitations to consider. First, our results may not be generalisable to the entire fire service, an acknowledged limitation of snowball sampling recruitment.14 Firefighters identified were more likely to be well connected, or receptive towards research, which may be influenced by health status. Women who experience preterm births may be at greater risk for mental health conditions which could affect their sociability.37 In addition, while study promotion did not emphasise reproductive health topics, firefighters who were concerned about or who had experienced adverse reproductive outcomes may have been more likely to participate. These factors may have contributed to selection bias in our study and affected the results. Future research should consider how to increase enrollment from volunteers, wildland and combination firefighters, and firefighters from smaller departments. The relatively low numbers of wildland/combination firefighters and volunteer firefighters in our analysis likely contributed to the limited statistical power.
Another limitation is misclassification; employment, wildland firefighter status, shift schedule, BMI and smoking were measured at survey in 2017 and assumed to be valid proxies for each pregnancy. However, mothers who experience adverse pregnancy outcomes are more likely to experience mental health changes,37 which could impact behavioural and lifestyle characteristics. These potential behavioural and lifestyle changes could have even greater impact if the pregnancy occurred more recently. In sensitivity analyses adjusted for BMI and smoking status (among other variables), we observed that the association between volunteers and risk of preterm birth in wildland or combination firefighters attenuated and was no longer statistically significant when we restricted to first pregnancies. This may suggest that earlier pregnancies have a greater probability of exposure misclassification, that misclassification of confounders are affecting estimates, or both. Future studies can address this issue by collecting pregnancy-level measures of all variables of interest. In addition, identifying as a wildland or combination firefighter during an index pregnancy may not equate to participating in wildland fire suppression during that pregnancy, which would have attenuated the observed association. Finally, our understanding of the effects of cumulative wildfire exposure on reproductive outcomes is limited, so it is possible that pregnancies that occurred outside of wildfire season could still be impacted by previous work.
Our findings contribute to growing evidence suggesting that women firefighters may have an excess risk of adverse reproductive outcomes compared with non-firefighters which varies by occupational factors. Women firefighters may benefit from increased occupational protections to reduce the risk of preterm birth. Research replicating these novel associations is needed to inform future policy development and personal decision-making.
Data availability statement
Data are available on reasonable request. The data generated or analysed during the current study are not publicly available due to restrictions based on the consent forms and IRB application for this study but are available from the authors on reasonable request.
Ethics statements
Patient consent for publication
Ethics approval
This study involves human participants and was approved by NDRI-USA Institutional Review Board (IRB00000634). Participants gave informed consent to participate in the study before taking part.
Acknowledgments
We would like to thank the International Association of Women in Fire and Emergency Service (Women in Fire) and the firefighters who participated in this study.
References
Supplementary materials
Supplementary Data
This web only file has been produced by the BMJ Publishing Group from an electronic file supplied by the author(s) and has not been edited for content.
Footnotes
Twitter @AlesiaJung
Contributors SJ contributed to the conception, study design and data acquisition of the study. AJ is responsible for the overall content as guarantor. AJ and LF were major contributors to the analysis, data interpretation and writing of the manuscript. LD, MB, SJ and JB also contributed to the data interpretation and writing of the manuscript. All authors have read and approved of the final manuscript.
Funding This research was supported in part by research grants awarded by the US Federal Emergency Management Agency Assistance to Firefighters Grant program to NDRI-USA (EMW-2015-FP00848) and the University of Arizona (EMW-2019-FP-00526) as well as research grants awarded by the US National Institutes of Environmental Health Sciences to the University of Arizona (T32 ES007091, P30 ES006694).
Competing interests None declared.
Provenance and peer review Not commissioned; externally peer reviewed.
Supplemental material This content has been supplied by the author(s). It has not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been peer-reviewed. Any opinions or recommendations discussed are solely those of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and responsibility arising from any reliance placed on the content. Where the content includes any translated material, BMJ does not warrant the accuracy and reliability of the translations (including but not limited to local regulations, clinical guidelines, terminology, drug names and drug dosages), and is not responsible for any error and/or omissions arising from translation and adaptation or otherwise.